

iStockphoto.com #155073233
As obesity and overweight affect more adolescents, this disease, once attributed to middle age and older, is striking an aggressive course that all clinicians will need to address.
By Neil H. White, MD
With the increasing prevalence of overweight and obesity and with 18.5% (or 13.7 million) of youth already being obese,1 type 2 diabetes (T2D) in youth is becoming an important part of every healthcare practitioner’s daily practice. Recent data from the SEARCH Study2 found that 10.8% of youth (0-19 years old) with diabetes had T2D, with the percentages varying considerably by race/ethnicity, with higher prevalence of T2D in Blacks (25.5%), Hispanics (23.7%), Asian/Pacific Islanders (23.8%), and American Indian/Alaska Natives (64.1%) than Non-Hispanic Whites (3.5%), with the majority of youth (97%) with T2D being adolescents.
In addition, it is becoming apparent that when type 2 diabetes appears in youth, it has a more aggressive course. Specifically, those who develop T2D during the teenage years progress to poor glycemic control more rapidly and have an earlier onset of life-altering and life-limiting complications than those who develop T2D as adults. As we have known for years in adults, T2D is a major source of morbidity, mortality, reduced quality of life and high healthcare expenditures. Now this condition, once thought a condition of middle aged and older adults, has now extended into the age range for youth and adolescents. It is important that all healthcare providers be aware of this changing landscape related to diabetes in youth.
In light of these realities, the American Diabetes Association (ADA) recently developed a Position Statement regarding guidelines for the evaluation and management of youth-onset type 2 diabetes.3 These guidelines have also been adopted by the ADA as part of their 2019 Standards of Medical Care in Diabetes.4 These guidelines are based on the published literature as of the time they were developed and the consensus of an expert panel; they address the pathophysiology, screening, diagnosis, and treatment of T2D and its comorbidities and complications in youth. The most notable components of these guidelines address the importance of screening and early diagnosis, management to achieve good glycemic control, and identifying diabetes-related complications and comorbidities to diminish their long-term impact on health and quality and length of life.
Risk-based screening and diagnosis of T2D in youth

iStockphoto.com #938340642
Until recently, screening of children for diabetes was done primarily in those who were symptomatic based on hyperglycemia. However, given the rapidly increasing rates of overweight and obesity in youth worldwide and the increasing prevalence of T2D in youth over the past 20 years, screening of overweight/obese youth is now recommended. Metabolic dysfunction, a major comorbidity of overweight/obesity in youth, can lead to early dysglycemia, which may progress to diabetes without being recognized, unless proper screening of high-risk youth is performed. Therefore, early recognition, diagnosis, and treatment of T2D in youth are critical to reduce the long-term morbidity and mortality associated with this serious health condition.
The guidelines3,4 recommend that all overweight or obese youth who are over 10 years of age or who have already entered puberty and have one or more additional risk factors (see page 36) be screened using a fasting plasma glucose, a 2-hour plasma glucose on an oral glucose tolerance test (OGTT), or an HbA1c. The diagnosis of diabetes is based on the American Diabetes Association criteria:
- HbA1c: diabetes >6.5%; prediabetes 5.7%-<6.5%;
- Fasting glucose: diabetes >126 mg/dL; prediabetes 100-<126 mg/dL;
- 2-h glucose: diabetes >200 mg/dL; prediabetes 140-<200 mg/dL.
Abnormal results should be confirmed on repeat testing. However, the most recent 2019 Standards of Care suggests that two abnormal results in one blood test may confirm the diagnosis. If confirmed, treatment of diabetes should be initiated. If normal, screening for diabetes or prediabetes should be repeated at least every 3 years, or sooner if symptoms occur.
Management of T2D in youth to achieve the best possible glycemic control
Those diagnosed with prediabetes (HbA1c 5.7%-<6.5%; fasting glucose 100-<126 mg/dL; 2-h glucose 140-<200 mg/dL) and their families should receive comprehensive lifestyle education—healthy nutrition guidance, counseling to decrease sedentary behavior and increase physical activity—aiming to prevent continued weight gain or achieve weight loss.
For youth diagnosed with T2D (HbA1c >6.5%, or fasting glucose >126 mg/dL, or 2-h glucose >200 mg/dL), a culturally sensitive, comprehensive lifestyle program including nutrition counseling and a recommendation for at least 30-60 minutes of moderate physical activity at least 5 days a week and aimed at decreasing the percent overweight by at least 7% should be actively pursued. However, in the majority of cases, lifestyle management alone is inadequate for achieving and maintaining glycemic control in overweight and obese youth. Therefore, in addition to lifestyle intervention, it is recommended that pharmacologic intervention be initiated at the time of diagnosis in youth with T2D. Of the many medication classes and medications approved for treatment of diabetes in adults, only metformin and insulin are currently approved in youth (<18 years old). Therefore, metformin and insulin are the mainstays of therapy. Details for prescribing can be found in the Standards of Care.4
Screening and management of complications of T2D in youth
Risk Factors for T2D in Youth3,4
- Overweight or obese (BMI > 85%ile for age and sex);
- History of being the product of a pregnancy complicated by diabetes or gestational diabetes;
- Family history of T2D in a first- or second- degree relative;
- Being from a racial/ethnic minority (Non-Hispanic Black; Hispanic; American Indian or Alaska Native)
- Findings associated with the “metabolic syndrome” or insulin resistance, including
a. Hypertension
b. Dyslipidemia
c. Acanthosis nigricans
d. Polycystic Ovary Syndrome (PCOS), in females;
e. Small-for-gestational age (SGA) birth weight.
Several studies, which are summarized and referenced in the ADA’s Position Statement and the 2019 Standards of Care,3,4 suggest a more rapid and relatively aggressive development and progression of diabetes-related complications in youth-onset T2D compared to adult-onset T2D and type 1 diabetes. A large percentage of youth with T2D have dyslipidemia, hypertension, and/or microalbuminuria. In my pediatric endocrinology practice, we have already had one patient with T2D who developed severe neuropathy after only 8 years and required amputations after having diabetes for only 9 years. One young woman had a heart attack after only 7 years of diabetes. We believe these patients are the canary in the coal minev.
According to the SEARCH study,2 while the overall prevalence of peripheral diabetic neuropathy is 7% in youth with type 1 diabetes, the prevalence in youth with T2D is 3-fold higher at 22%. Moreover, case fatality is increased in youth with T2D compared with type 1 diabetes of similar age and duration, driven by cardiovascular disease deaths. Therefore, unlike the recommendations in youth with type 1 diabetes that screening for complications begin after 5 years of disease, the guidelines suggest that screening for complications in youth with T2D be done annually starting at the time of diagnosis.
Click here to download a PDF with English and Spanish versions
While measurement of blood pressure should be part of every clinic visit, youth with T2D should have an annual eye examination (to detect retinopathy), and annual urine albumin assessment and serum creatinine (to detect kidney involvement). They should also have an annual evaluation of lipids and cardiovascular risk factors, as well as liver enzymes (to detect nonalcoholic fatty liver disease), and careful evaluation of the feet to identify diabetic peripheral neuropathy or vascular compromise. This evaluation should include:
- close inspection to look for sores, ulcers, callus, and infection;
- assessment of circulatory sufficiency (color, pulses, and capillary refill);
- assessment of sensation, including small myelinated fibers (temperature or pinprick); large myelinated fibers (vibration, reflexes, or proprioception), and loss of protective sensation (ability to feel the 10-gram monofilament).
All people with diabetes should receive education about foot care. For those with any abnormality in their foot examination, no matter how minor, this education should be intensified and reinforced regularly. As indicated, professional, specialized foot care should be recommended and strongly encouraged to prevent the devastating consequences of diabetic peripheral neuropathy.
Conclusions
Type 2 diabetes mellitus, previously referred to as adult-onset diabetes mellitus, maturity-onset diabetes mellitus, non-insulin-dependent diabetes mellitus or type II diabetes, had been considered a disease of adults only and of youth from some Native American groups. Today, however, T2D has become a major disorder affecting youth and adolescents, especially among those who are overweight or obese. The nature of this disorder and its complications in youth has emerged as a major public health issue for the 21st century. Timely diagnosis using risk-based screening, aggressive management of glycemia and regular screening, and attention to the potentially devastating life-altering and life-limiting complications and comorbidities are essential to improve the quality and length of life for these individuals. While more basic, clinical, and translational research is needed, every clinician can play a role in halting T2D and its complications among youth.
Dr. Neil H. White is Professor of Pediatrics in the Division of Endocrinology & Diabetes at the Washington University in St. Louis School of Medicine in St. Louis, Missouri. He has participated in many NIH-sponsored, multicenter clinical trials including the TODAY (Treatment Options for type 2 Diabetes in Adolescents and Youth) Study. The writing of this review is partially supported by grant number P30DK092950 from the National Institute of Diabetes and Digestive and Kidney Disorders to the Washington University Center for Diabetes Translation Research.
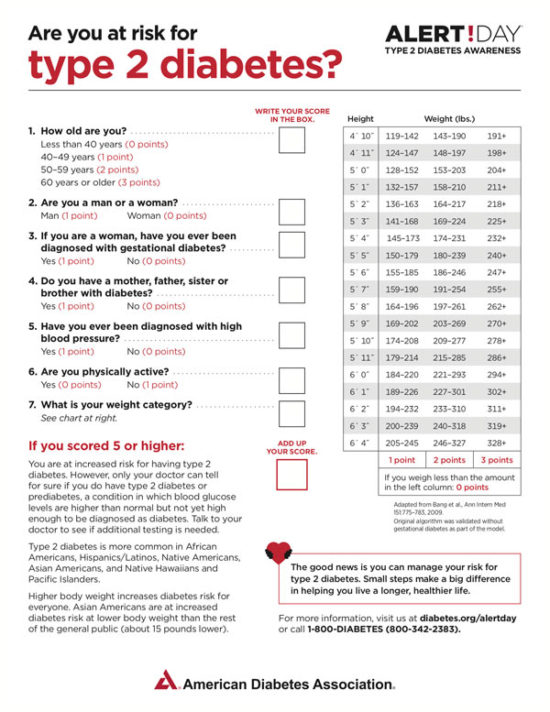
March 26 is Diabetes Alert Day
![]() One in three Americans is at risk for developing type 2 diabetes, a serious disease that can lead to complications such as kidney disease, blindness, and amputations. But type 2 diabetes doesn’t have to be permanent–it can be prevented or delayed with healthy lifestyle modifications.
One in three Americans is at risk for developing type 2 diabetes, a serious disease that can lead to complications such as kidney disease, blindness, and amputations. But type 2 diabetes doesn’t have to be permanent–it can be prevented or delayed with healthy lifestyle modifications.
Held the last Tuesday of March each year, American Diabetes Association Alert Day® encourages everyone to take the Type 2 Diabetes Risk Test (see page 35) and participate in workplace-friendly activities that will teach them about reversing the risk for diabetes.
Contact your local ADA affiliate (www.diabetes.org) for An Alert Day toolkit.
- Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of obesity among adults and youth: United States, 2015–2016. NCHS data brief, no 288. Hyattsville, MD: National Center for Health Statistics. 2017.
- Pettitt DJ, Talton J, Dabelea D, et al. Prevalence of diabetes in U.S. youth in 2009: the SEARCH for diabetes in youth study. Diabetes Care. 2014 Feb;37(2):402-408.
- Arslanian S, Bacha F, Grey M, Marcus MD, White NH, Zeitler P. Evaluation and management of youth-onset type 2 diabetes: a Position Statement by the American Diabetes Association. Diabetes Care. 2018; 41(12):2648-2668.
- American Diabetes Association: Children and adolescents: standards of medical care in diabetes—2019. Diabetes Care 2019; 42(Supplement 1):S148-S164.





