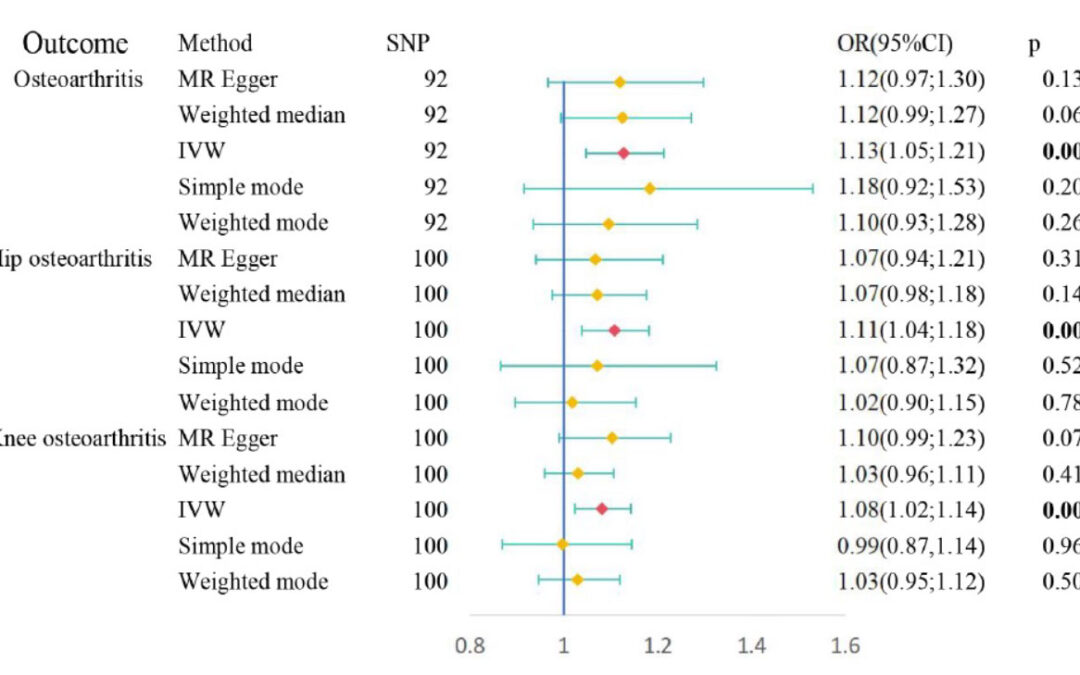
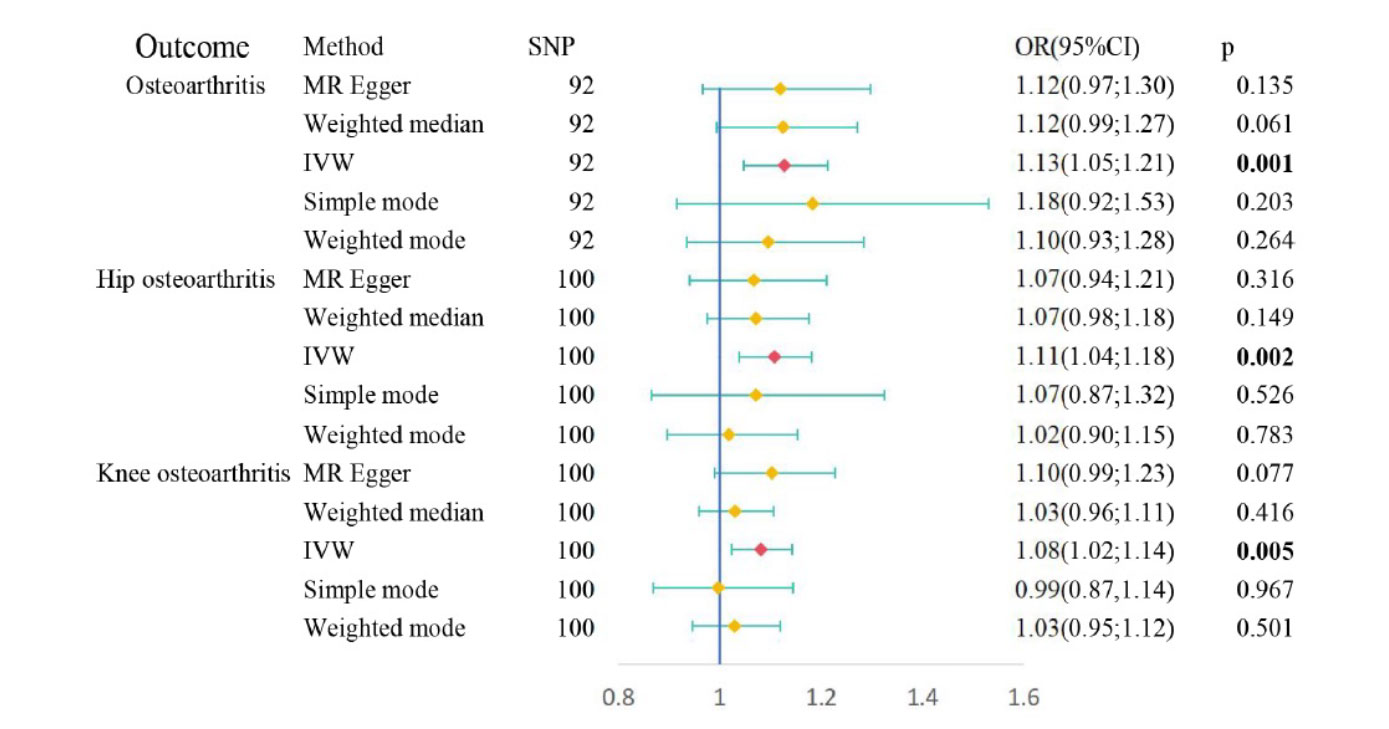
Figure: Causal relationships between obstructive sleep apnea and osteoarthritis risk performed by Mendelian randomization. IVW, inverse variance-weighted approach;SNP, single nucleotide polymorphism;
This study, the first of its kind, aimed to explore the connection between Obstructive Sleep Apnea (OSA) and osteoarthritis (OA) and evaluate causality using Mendelian randomization (MR), utilizing large-scale observational study data and genetic datasets. Cross-sectional observational analysis identified significant relationships between OSA and OA, while findings based on the MR study did support a causal role. The analysis of potential mediating factors found that BMI was an important factor between OSA and OA.
Previous studies found that the prevalence of OSA among individuals with OA was significantly higher than that in the general population, 66% versus 17%, respectively.
Sleep, as a period of physiological recovery, creates an environment conducive to cell proliferation, migration, and differentiation, with cell division and protein synthesis peaking during sleep. OSA causes airway collapse, leading to oxygen deprivation and disruption of sleep rhythm. Previous studies revealed that OSA can cause increases in inflammatory, oxidative stress, and metabolic abnormalities, such as abnormal blood lipids, uric acid, and blood sugar, which may lead to the future development of OA.
In this study, the MR analysis provided evidence of a causal relationship between OSA and OA, substantiated by rigorous examinations of horizontal pleiotropy and heterogeneity. These findings were further reinforced by 2-way MR analysis, eliminating the possibility of reverse causality.
Obesity and inflammation are potential pathogenic mechanisms by which OSA leads to OA. Previous studies, through bioinformatics analysis, have found that shared inflammation genes between OSA and OA are significantly enriched in the TNF pathway and the IL-17 pathway.
The correlation between OSA and BMI has been a focal point of research for quite some time. The sleep fragmentation due to OSA can result in a state of effective sleep deprivation, which, in turn, can cause daytime drowsiness, a reduction in physical activity, and, consequently, an increase in body weight. One key factor contributing to weight gain in individuals with OSA is insulin resistance. Studies have indicated that the development of insulin resistance in the context of sustained intermittent hypoxia is closely tied to the disruption of leptin signaling pathways.
These authors observed significant mediated effects of BMI on the associations between OSA and OA risk. In particular, other obesity and insulin resistance markers mediated no association between OSA and OA risk, among which the mediated proportion of BMI was 36.9%, consistent with previous research. These findings suggested that OSA may increase obesity and finally aggravate OA.
A high BMI or obesity leads to overloading the joints due to excess weight, which, in turn, leads to the destruction of articular cartilage. Others attributed it to excess fat tissue, which secretes hormones and proinflammatory cytokines, contributing to low-grade systemic inflammation. Given that BMI is a relatively controllable mediating factor, effectively managing BMI in OSA patients could potentially reduce the incidence of OA.
Source: Yang Z, Lv T, Jin L, et al. The relationship between obstructive sleep apnea and osteoarthritis: evidence from an observational and Mendelian randomization study. 2024: Front. Neurol. 15:1425327. doi: 10.3389/fneur.2024.1425327





