
 By Dr. Jennifaye V. Brown
By Dr. Jennifaye V. Brown
Epilogue: Sometimes you have to start with the end.
“You helped our daughter, Laylah, with getting AFOs last year. They have been wonderful for her and we are happy with the service provided by Hanger. She heads down to the College of Charleston in August to live in a dorm and start freshman year. She no longer tries to hide her AFOs. You were instrumental in getting her to this point. Thank you so much! Warm regards,” Catherine.
Prologue: Background Knowledge
Charcot-Marie-Tooth (CMT) is the most common heredity lower motor and sensory neuron disease that causes progressive muscle weakness and sensory loss leading to foot deformities and debilitating gait patterns.1 There are over 100 genetic subtypes, however, the 2 major causes are genetic mutations of the peripheral myelin protein and chromosomal organization and architecture and second, genetic defects damaging the Schwann cell and the axon’s myelin sheath as well as aggregating mutant proteins in the endoplasmic reticulum causing cell death (apoptosis).2-6 This disease process is characterized as being nerve-length dependent disorder and comes in 2 forms categorized as demyelinating (CMT1) and axonal (CMT2).1
CMT1 pathophysiology involves a malformation of and inappropriate maintenance of myelin such that there is an abnormal thickening of it around peripheral nerve fibers. This abnormal thickening, which produces an onion bulb appearance causes a reduction in nerve conduction velocity leading to motor and sensory dysfunction.3,7-8 CIMT1, considered a segmental demyelination neuropathy, tends to be slow and progressive in nature whereas CIMT2 is characterized by severe functional impairments with an early onset. 3,7-8 CMT2 involves the anterior horn cell and axonal degeneration and diminution causing peripheral nerve dysfunction resulting in progressive muscle weakness, atrophy, and sensory deficits. 3,7-8 Nerve conduction velocity is relatively preserved. 3,7-8
The physical therapy examination should include an assessment of pain, range of motion addressing talocrural motion in addition to that in the hindfoot, midfoot and forefoot, weakness (and may I add isometric, concentric and eccentric as it pertains to gait), atrophy, reflexes, gait appearance (foot drop versus steppage) in addition to kinematic (motion), kinetic (force), and spatiotemporal (time/distance) features, and foot musculoskeletal deformities. The most common foot deformity is pes cavovarus, progressive in nature and described as an abnormally high arch (pes cavus) and inverted heel.9 These details are essential to get the proper AFO and shoes.10-12
The patient/client may complain of having difficulty walking at increased speeds or with running, tripping, falls, twisting or spraining their ankles and therefore, wear high top sneakers.12-13 Atrophy of muscles more distal than proximal may lead to the appearance of “stork leg deformity.”14 Complaints of creeping sensations are a result of damage to axons associated with sensory structures in leg muscles.15
First Dialogue: Client, Caregivers, and Physical Therapist
I am humbled and always in awe that people request my services for a physical therapy examination regarding an ankle foot orthosis (AFO). I was referred to Laylah who has a diagnosis of Charcot-Marie-Tooth (CMT) and was unhappy with her last set of AFOs. She had completed her physical therapy and wanted a new pair that would allow her to fully engage in the activities of life as a teenager which included traveling with her parents and exploring the thought of going to college. Laylah would have to walk a whole lot more than she was accustomed to and wanted to be comfortable amongst her peers in the new environment of collegiate life. I was up for the challenge with the focus on optimizing Laylah’s ability to participate in life and not so much trying to change a disease process known to be progressive in nature at the body structure function level.1-6, 16 The narrative was hers, not what I knew about CMT. I made this a ‘team’ effort with Laylah being the center of attention and her parents having a supportive role to confirm and clarify her truths. An interprofessional team with a patient-centric approach is highly recommended in the literature.11 Lastly, after completing the examination for an AFO, I prescribed some advanced gait activities to prepare for bilateral AFO use and met with them at the orthotist’s office.13,17-18
Second Dialogue: Client, Caregivers, Physical Therapist, and Orthotist
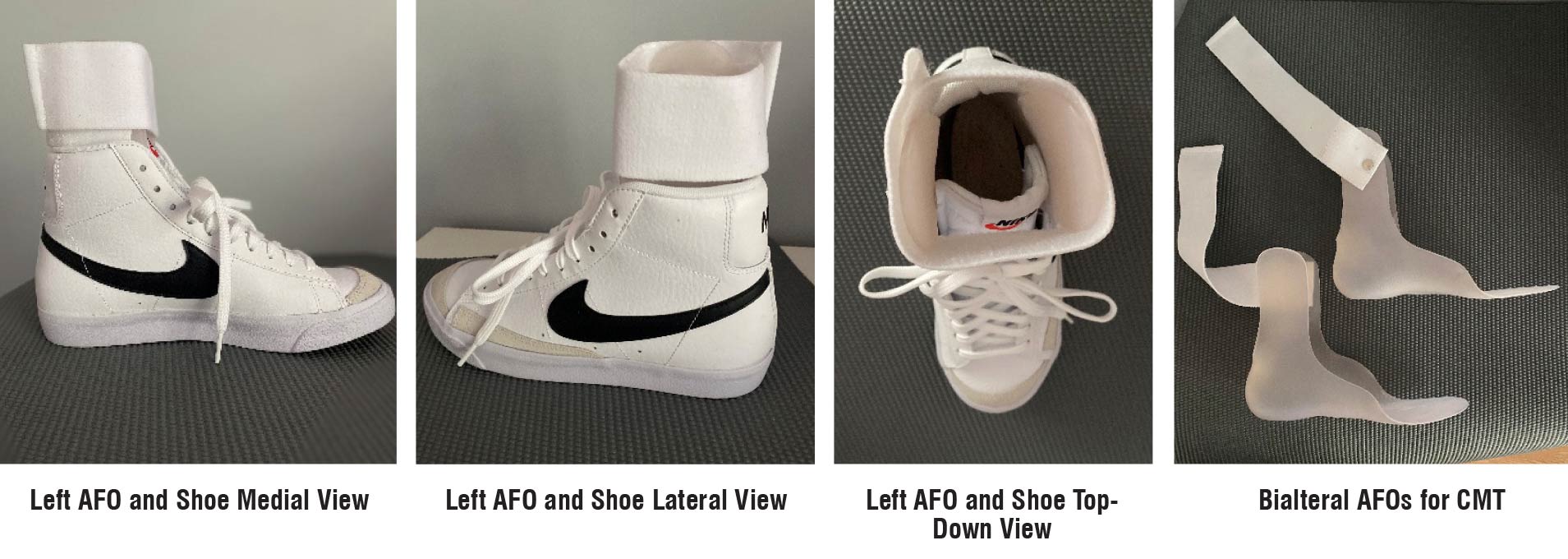
Laylah was able to speak about what she wanted and wore shoes similar to what she wears and would wear daily at the appointment with the orthotist. She preferred high top sneakers because they supported her ankles once fatigue sets in. I conveyed the findings of my physical therapy examination which supported the decision to get an AFO that primarily had medial lateral support and free range for plantarflexion and dorsiflexion as well as a flexible foot play to accommodate toe hyperextension needed for preswing and accentuated push off if she wanted to walk faster. Research indicates that predictors of walking recovery (and in Laylah’s case, also walking sustainability and endurance) are walking speed and the ability to generate lower extremity propulsion at push off.19 Furthermore, research indicates meaningful gait changes occur when AFOs are tailored to the patient which includes not only musculoskeletal and neuromuscular impairments but the perceptions of the AFO’s appearance, fit and function.20-26 The orthotist, Dave Adams, CPO was someone I had worked with before and he knew my style of AFO fabrication: total contact and contoured fit with the edges beveled and thinned out away from the skin; original thickness of the thermoplastic only in the areas of sustained weakness but other areas flexible to allow dynamic stability and mobility between the hindfoot, midfoot and forefoot; and last, tension straps added based on the isometric, concentric and eccentric strength of the anterior, posterior and lateral leg muscles that controlled the foot. After some questions from Dave to Laylah, her parents and me and a few suggestions from him, it was time for the casting process. I knew Laylah was in good hands, and therefore left to get to another appointment. Everyone that I have sent to Dave gets educated on an AFO wearing schedule and what to look for in terms of complications from wearing the AFO such as skin irritations or pain, be it neuromuscular or musculoskeletal in origin. Here is the kicker: I never received a call from Laylah or her parents indicating that she was having problems with her AFOs during the spring and summer season before entering college. Laylah was so pleased with the fit and function, her family took it upon themselves to order another pair. I did not know until I asked them (the parents) if they would read my book for clarity and understanding.27 And not only did they read it and provide edits, but wrote the kind words in the epilogue.
The Real Story: Communication
The success of this outcome was embedded in the dialogue. Conversations had were about communicating to be heard and acknowledge what was heard by offering solutions that took into consideration social determinants of health from the perspective of a teenager. As I say, we as healthcare providers are experts in our professional roles, but the people we serve are experts in their lived experiences. We should be able to communicate impairments from disease processes with the clarity and simplicity of a glass of refreshing water but package it with the hope that the water will tastes as good as sweet tea. I am so glad to be a part of a team that recognizes my strength in gait analysis and treatment as well as lower extremity examination and recommendations for AFOs. When the orthotist and the physical therapist work together as a team, the patient/client wins every time.
Jennifaye V. Brown, PT, MSPT, PhD, NCS, CAPS is an American Physical Therapy Association 4-time 10-year board certified neurologic physical therapist in Charleston, South Carolina, specializing in stroke rehabilitation, specifically gait analysis and treatment, AFO design, and the redesign of lived spaces allowing individuals with disAbilities to age in place. She is the author of the book, Brace Yourself: Everything You Need to Know About AFOs After Stroke. Visit her YouTube channel @jvbneuropt for more information regarding stroke rehabilitation.
- Nagappa M, Sharma S, Taly AB. Charcot-Marie-Tooth Disease. [Updated 2024 Jun 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK562163/
- Kazamel M, Boes CJ. Charcot Marie Tooth disease (CMT): historical perspectives and evolution. J Neurol.2015;262(4):801-5. doi: 10.1007/s00415-014-7490-9
- Magy L, Mathis S, Le Masson G, Goizet C, Tazir M, Vallat JM. Updating the classification of inherited neuropathies: Results of an international survey. Neurology. 2018;90(10):e870-e876. doi:10.1212/WNL.0000000000005074
- Pareyson D, Saveri P, Pisciotta C. New developments in Charcot-Marie-Tooth neuropathy and related diseases. Curr Opin Neurol. 2017;30(5):471-480. doi: 10.1097/WCO.0000000000000474
- Laurá M, Pipis M, Rossor AM, Reilly MM. Charcot-Marie-Tooth disease and related disorders: an evolving landscape. Curr Opin Neurol. 2019;32(5):641-650. doi: 10.1097/WCO.0000000000000735
- Fridman V, Bundy B, Reilly MM et al. Inherited Neuropathies Consortium. CMT subtypes and disease burden in patients enrolled in the Inherited Neuropathies Consortium natural history study: across-sectional analysis. J Neurol Neurosurg Psychiatry. 2015;86(8):873-878. doi: 10.1136/jnnp-2014-308826
- Fortun J, Li J, Go J, Fenstermaker A, Fletcher BS, Notterpek L. Impaired proteasome activity and accumulation of ubiquitinated substrates in a hereditary neuropathy model. J Neurochem. 2005;92(6):1531-1541. doi: 10.1111/j.1471-4159.2004.02987
- Saporta AS, Sottile SL, Miller LJ, Feely SM, Siskind CE, Shy ME. Charcot-Marie-Tooth disease subtypes and genetic testing strategies. Ann Neurol. 2011;69(1):22-33. doi:10.1002/ana.22166
- Rose KJ, Hiller CE, Mandarakas M, Raymond J, Refshauge K, Burns J. Correlates of functional ankle instability in children and adolescents with Charcot-Marie-Tooth disease. J Foot Ankle Res. 2015 Nov 5;8:61. doi:10.1186/s13047-015-0118-1
- Mathis S, Magy L, Vallat JM. Therapeutic options in Charcot-Marie-Tooth diseases. Expert Rev Neurother. 2015;15(4):355-366. doi:10.1586/14737175.2015.1017471
- Corrado B, Ciardi G, Bargigli C. Rehabilitation management of the Charcot-Marie-Tooth Syndrome: A systematic review of the literature. Medicine (Baltimore). 2016;95(17):e3278. doi:10.1097/MD.0000000000003278
- Guillebastre B, Calmels P, Rougier PR. Assessment of appropriate ankle-foot orthoses models for patients with Charcot-Marie-Tooth disease. Am J Phys Med Rehabil. 2011;90(8):619-27. doi.org/10.1097/PHM.0b013e31821f7172
- Kikuchi K. clinical characteristics of gait disturbance in Charcot-Marie-Tooth Disease and future directions in physical therapy. Cureus. 2025;17(6):e85581. doi:10.7759/cureus.85581
- Njegovan ME, et al. Rehabilitation medicine approach to Charcot-Marie-Tooth disease. Clin Podiat Med Surg. 1997; 14:99-116.
- Boentert M, Dziewas R, Heidbreder A, et al. Fatigue, reduced sleep quality and restless legs syndrome in Charcot-Marie-Tooth disease: a web-based survey. J Neurol. 2010;257(4):646-652. doi:10.1007/s00415-009-5390-1
- Carter GT, Weiss MD, Han JJ, Chance PF, England JD. Charcot-Marie-Tooth disease. Curr Treat Options Neurol. 2008;10 (2): 94-102. doi.org/10.1007/s11940-008-0011-3
- Kedlaya D, Meier R.H. Physical medicine and rehabilitation for Charcot-Marie-Tooth disease. E-medicine. Article Last Updated: Jan 8, 2007. Accessed March 10, 2026. https://hmlfunctionalcare.com/wp-content/uploads/2021/06/CMT-Disease.pdf
- Dudziec MM, Lee LE, Massey C, et al. Home-based multi-sensory and proximal strengthening program to improve balance in Charcot-Marie-Tooth disease Type 1A: a proof of concept study. Muscle Nerve. 2024;69:354-61. doi:10.1002/mus.28032
- Awad LN, Reisman DS, Pohlig RT, Binder-Macleod SA. Identifying candidates for targeted gait rehabilitation after stroke: better prediction through biomechanics-informed characterization. J Neuroeng Rehabil. 2016 Sep 23;13(1):84. doi:10.1186/s12984-016-0188-8
- Kim A, Frecklington M, Philps A, Stewart S: The effect of ankle-foot orthoses on gait characteristics in people with Charcot-Marie-Tooth disease: a systematic review and meta-analysis. J Foot Ankle Res. 2024;17(3):e70003. doi:10.1002/jfa2.70003
- Guillebastre B, Calmels P and Rougier PR. Assessment of appropriate ankle-foot orthoses models for patients with Charcot-Marie-Tooth disease. Am J Phys Med Rehabil. 2011; 90(8):619-627. doi: 10.1097/PHM.0b013e31821f7172
- Phillips MF, Robertson Z, Killen B, et al. A pilot study of a crossover trial with randomized use of ankle-foot orthoses for people with Charcot-Marie-Tooth disease. Clin Rehabil. 2012;26: 534–544. doi: 10.1177/0269215511426802
- Ramdharry GM, Day BL, Reilly MM, et al. Foot drop splints improve proximal as well as distal leg control during gait in Charcot-Marie-Tooth disease. Muscle Nerve. 2012; 46:512–519. doi:10.1002/mus.23348
- Vinci P, Paoloni M, Ioppolo F, Gargiulo P, Santilli V. Gait analysis in a patient with severe Charcot-Marie-Tooth disease: a case study with a new orthotic device for footdrop. Eur J Phys Rehabil Med. 2010;46(3):355-361.
- Brown JV, Best S, Suhr J. Ankle Foot Orthoses: The Impact of Appearance, Function, and Fit in Individuals with Stroke. Lower Extremity Review. 2021;13(11):39-50. Accessed March 25, 2026. https://lermagazine.com/cover_story/ankle-foot-orthoses-the-impact-of-appearance-function-and-fit-in-individuals-with-stroke
- Brown JV, Cotton J, Best S, Suhr JA. Communicating key features of an ankle foot orthosis from a patient’s perspective: a case study. NSAH Journal. 2020; 17(1):6-20.
- Brown JV. Brace Yourself: Everything You Need to Know About AFOs After Stroke. IngramSpark; 2025.





