 By Marie Keplinger, DPM, FACFAS
By Marie Keplinger, DPM, FACFAS
Introduction: The Challenge of Surgical Perfection
Surgery, especially in the world of foot and ankle reconstruction, is like solving a complex, 3-dimensional puzzle. Our goal is to take a structure that has adapted over a lifetime into a painful position and restore its original, functional architecture. One of the most powerful tools we have for this is the Lapidus procedure, which corrects a complex bunion deformity–what surgeons call a triplane deformity. We meticulously realign the bones in all 3 dimensions to give the patient a stable foot that will last a lifetime.
But what happens when the puzzle pieces heal in the wrong position? What do you do when the surgery is a success in terms of healing, but a failure in terms of alignment? This guide explores the surgical challenges that can arise after a Lapidus procedure and reveals the toolkit surgeons use to fix them.
 1. The Goal: What a Successful Lapidus Procedure Achieves
1. The Goal: What a Successful Lapidus Procedure Achieves
The primary goal of a Lapidus procedure is to correct hallux valgus deformity by addressing its true nature as a triplane deformity. This means the bone is misaligned in 3 different geometric planes. To achieve an adequate correction, we must fix the alignment in all 3.
- Adduction: The first metatarsal bone has angled away from the foot’s midline and toward the second toe, creating the characteristic medial bump. We must bring it back into a straight alignment.
- Dorsal Elevation: The metatarsal has tilted upward in the sagittal plane (when viewed from the side), disrupting the foot’s arch. We have to bring it back down to bear weight properly.
- Pronation: The metatarsal has rotated along its long axis, causing the toenail to face inward. We have to de-rotate it so the toe is properly aligned with the ground.
When all 3 of these planes are corrected, the result is a stable, correctly aligned foot designed to function perfectly for a lifetime.
This is the ideal outcome, but the reality is that achieving this exact anatomic position on the operating table is difficult, and sometimes, complications arise.
2. The Core Problem: Understanding “Malunion”
When a Lapidus procedure doesn’t achieve its goal, the most common issue we face is a malunion. In simple terms, a malunion means the bones have successfully fused together–the healing process worked–but they fused in an incorrect or poor position.
These malunions can be the result of placement of the first ray not in an ideal position during initially, technically complex surgery. It’s a failure of positioning, not a failure of biology.
Think of it like a series of case files. Each malunion presents a unique problem with a distinct impact on the patient. Let’s investigate the most common ones.
 3. Case Files: The 5 Common Types of Lapidus Malunions
3. Case Files: The 5 Common Types of Lapidus Malunions
3.1. The Bunion Returns (Recurrence & Undercorrection)
- Problem: This is the most straightforward malunion: the bunion deformity comes back. It happens when the angles of the foot, particularly the angle between the first and second metatarsals, were not corrected enough during the first surgery.
- Patient Impact: While an X-ray might show that the deformity has returned, it doesn’t always mean the patient is in pain. A 2020 study found that while 46% of cases had radiographic recurrence, only 12% were symptomatic enough to require a second surgery.
Key Insight: Research by Shabuya et al. revealed that the position of the sesamoids is the single most predictive factor for recurrence. The data is striking: they found that when the tibial sesamoid position was greater than 4 (out of a 7-point scale), the recurrence rate was 50%. If it was greater than 5, the rate jumped to 60%. If these bones are not adequately realigned, they exert a pull that gradually causes reoccurence.
3.2. The Upward Tilt (Elevation)
- Problem: This occurs when the first metatarsal bone heals in an upward-tilted position. This is often due to poor positioning intraoperatively or a failure to completely clean out the cartilage from the bottom part of the joint space during the initial surgery.
- Patient Impact: When the first ray is elevated, it no longer carries its share of the body’s weight. This pressure is transferred to the other toes, causing a painful condition called transfer metatarsalgia. It can also lead to the development of a stiff, arthritic big toe, known as hallux rigidus.
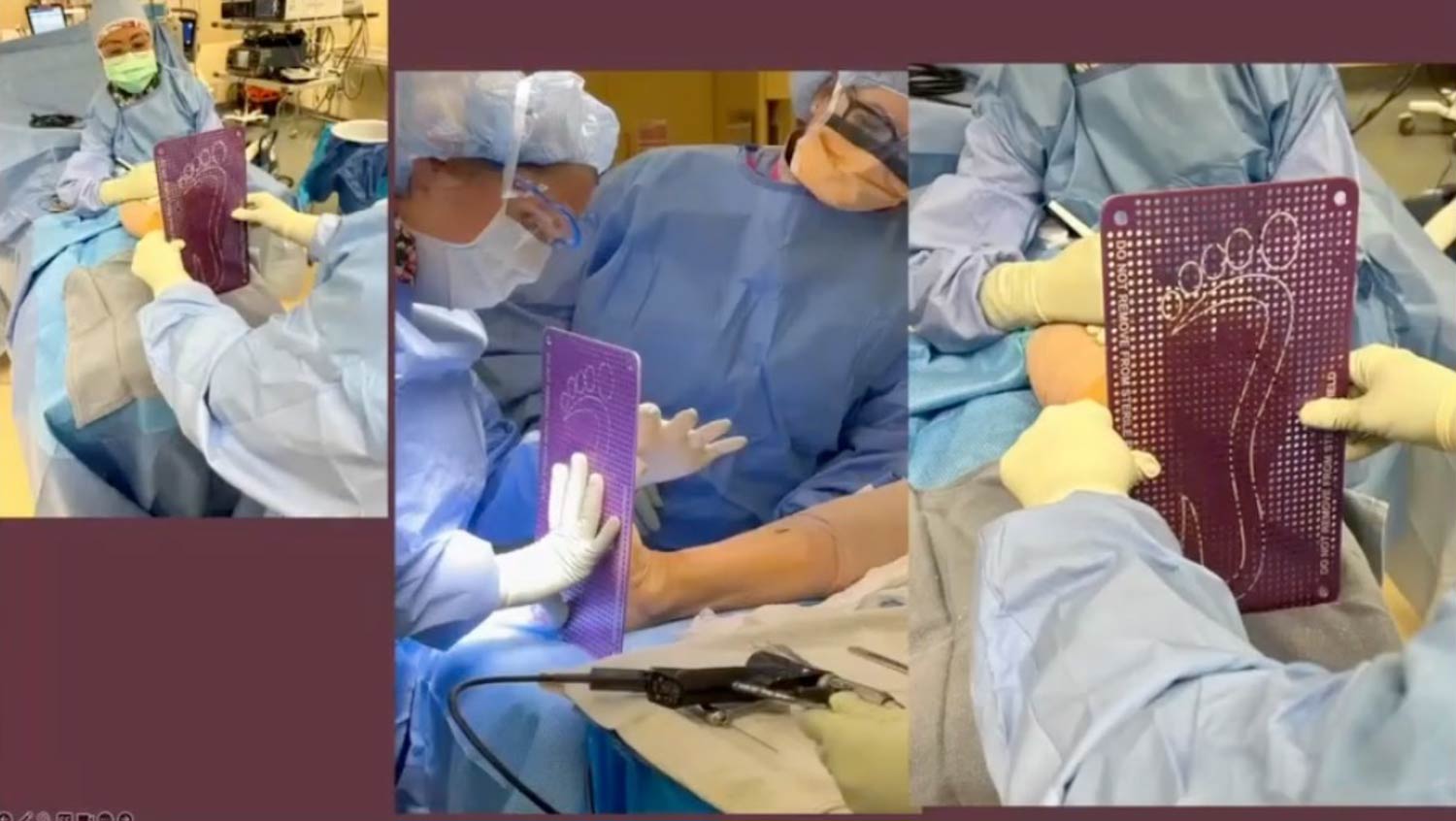
Surgeon’s Tip: To prevent elevation, here is a good technique in the operating room. Before putting in the final screws or plates, place a wide, flat metal plate with small indentations under the patient’s foot. My assistant then secures the leg while I simulate weight-bearing. When the plate is removed, I inspect the temporary marks left on the sole of the foot. If the marks are evenly distributed across all 5 metatarsal heads, I know the alignment is acceptable. If not, I’ll adjust the position before finalizing the fixation (see image).
 3.3. The Short Step (Excessive Shortening)
3.3. The Short Step (Excessive Shortening)
- Problem: While every Lapidus procedure involves some shortening of the bone, excessive shortening occurs when too much bone is removed during joint preparation. The surgical technique plays a major role. The curettage technique, which involves scraping the joint surfaces, causes significantly less shortening than the wedge resection technique, where a slice of bone is removed.
- Patient Impact: A first metatarsal that is too short disrupts the foot’s natural arch, or parabola. Similar to an elevated ray, this causes an overload of the lesser rays. A finite element study identified a critical threshold: when shortening exceeds 6 mm, the load on the central rays becomes excessive.
3.4. The Downward Press (Excessive Plantar Flexion)
- Problem: This is the opposite of elevation. The first metatarsal is healed pointing too far downward (plantar flexed). This is often the result of poor positioning in the operating room.
- Patient Impact: A plantarflexed metatarsal causes an overload of the sesamoid complex. This leads to significant pain and callus formation directly under the ball of the foot, making walking uncomfortable.
3.5. The Outward Point (Overcorrection)
- Problem: Also known as hallux varus, this malunion occurs when the surgeon has overcorrected the hallux valgus deformity. This causes the hallux to point away from the other toes, creating an unsightly gap and potential pain with shoewear.
- Patient Impact: Patients with this condition are often asymptomatic. The toe might look unusual on an X-ray, but it doesn’t cause pain or functional problems. However, if the toe rubs on shoes or becomes symptomatic, it requires surgical correction.
Each of these malunions represents a distinct anatomical puzzle that has been solved incorrectly. Fortunately, for every problem, foot and ankle surgeons have developed a specific set of tools and techniques to provide a solution.
4. The Surgeon’s Toolkit: Solutions for Correcting Malunions
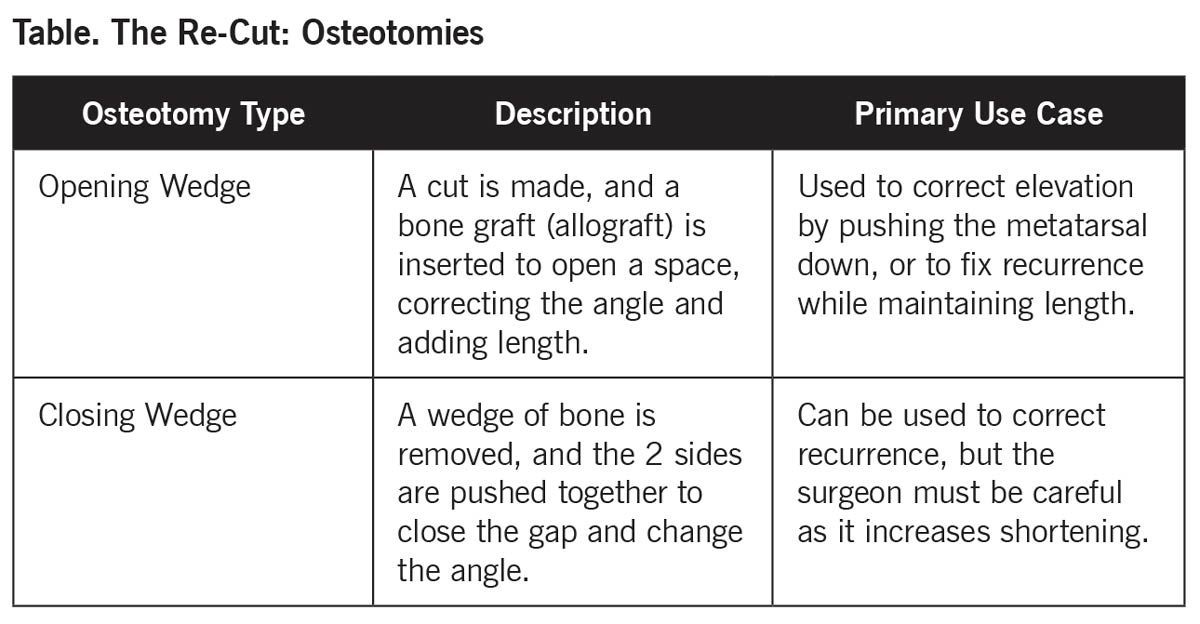
4.1. The Re-Cut: Osteotomies
An osteotomy is a procedure where a surgeon strategically cuts a bone to realign it. For malunions where successful arthrodesis has been achieved but simply angled incorrectly, osteotomies are the primary solution. (Table)
4.2. The Stabilizer: First MTPJ Arthrodesis (Fusion)
An arthrodesis is a procedure where a joint is surgically fused, making it stable and permanently immovable. In this case, the procedure involves fusing the main joint of the hallux (the first metatarsophalangeal joint, or MTPJ).
This procedure is ideal for 2 particularly difficult problems where a simple osteotomy won’t be enough.
- Excessively Short First Ray: When the bone is too short to be effectively lengthened with an osteotomy alone, fusing the big toe joint in conjunction with a bone graft re-establishes the proper length and restores the arch of the foot.
- Symptomatic Hallux Varus (Overcorrection): Fusion provides a reliable, tried and true method to get the toe into a good, permanent position, eliminating the risk of the deformity returning a second time.
A common concern is that fusing the big toe joint will limit activity, but studies show up to a 96% return to normal activity, making this an incredibly effective and reliable solution.
5. Conclusion: The Art of the Second Chance
The Lapidus procedure is a powerful but technically demanding surgery. When the bone heals in a less-than-perfect position, it presents a significant challenge for both the patient and the surgeon. However, the field of foot and ankle surgery is built on problem-solving.
For every type of malunion–whether it’s recurrence, elevation, shortening, or overcorrection–surgeons have a specific tool in their toolkit. From precise bone cuts (osteotomies) to stabilizing joint fusions (arthrodesis), there is a clear and effective solution for each problem.
When you’re going into these cases, you want the best result the first time, but you definitely want it on the second run. You don’t want to have to go back and continue to reoperate. The goal is to fully understand why the first procedure failed and apply the right solution to ensure the patient gets the best possible outcome–a second chance at a well aligned, pain-free foot.
As a highly trained podiatric surgeon, L. Marie Keplinger, DPM, specializes in successfully treating foot and ankle conditions created by sports injuries, trauma, degenerative diseases and complex deformity. Orthopaedic fellowship-trained, Dr. Keplinger’s expertise includes reconstructive foot and ankle procedures, tendon repair, arthroscopy, as well as total ankle replacements.
This article is a summary of Dr. Keplinger’s presentation, “1st Ray Shortening and Elevation Post-Lapidus, How Do I Address it?” from the APMA Surgical Complications Virtual Seminar on January 18, 2025 . To view the full presentation with questions and answers—and see the agenda for the program, visit https://apmasurgical.lerexpo.com/ . Continuing education credits are available for this and many of the lerEXPO programs.





