
 By Kelsey Millonig, DPM, MPH, FACFAS, DABPM, DABFAS
By Kelsey Millonig, DPM, MPH, FACFAS, DABPM, DABFAS
Charcot neuroarthropathy is a complex condition that often leads to considerable challenges due to its complex nature. One primary concern is the management of soft tissue complications, including chronic wounds and surgical dehiscence, which are prevalent among Charcot patients. These complications can significantly impact limb functionality and the patient’s quality of life. Therefore, understanding and addressing these issues is crucial for optimizing patient outcomes. By employing preventative measures, conducting thorough assessments, and strategically using reconstructive techniques, one can effectively manage Charcot soft tissue complications to promote better patient outcomes.
Prevention Strategies
Patient Optimization Before Surgery: Preventing soft tissue complications in Charcot patients begins with meticulous pre-operative preparation. Comprehensive patient optimization is essential to enhance the outcomes of reconstructive surgery. This involves thorough lab work; reviewing A1C levels, albumin, and pre-albumin; and conducting a full metabolic bone profile, including assessments of vitamin D, calcium, thyroid levels, and parathyroid hormone. An extensive vascular workup is also crucial, encompassing non-invasive studies and arterial duplexes, with consultations from vascular specialists if required. Additional steps include ensuring smoking cessation, managing edema effectively, and handling comorbid conditions such as chronic kidney disease. Identifying and addressing any existing infections pre-operatively, through wound assessment or osteomyelitis diagnosis, is critical. Prophylactic use of intranasal calcitonin is also advised, based on its minimal risk and potential benefit.
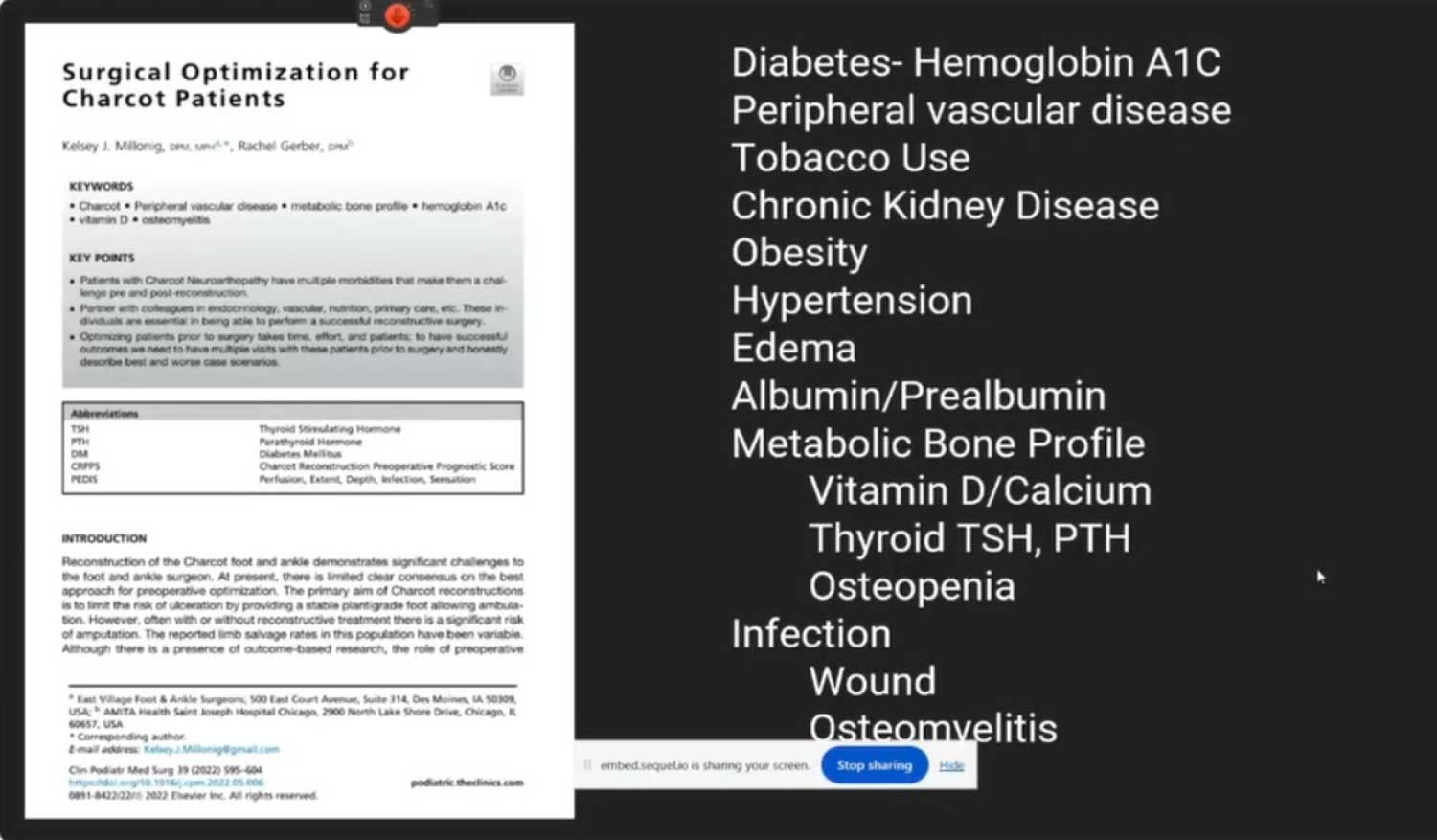 Importance of Vascular and Infection Assessments: Ensuring proper blood flow is pivotal in the pre-operative phase. Vascular assessments must go beyond basic non-invasive tests to include comprehensive arterial duplex imaging; also consider pre-surgical vascular consultations to address any concerns about limb perfusion. Accurately diagnosing and managing any infections before surgery is vital; thorough assessments involve clinical evaluations, lab work, and imaging where CT scans are preferred over MRIs due to the latter’s potential to misdiagnose Charcot as osteomyelitis. The objective is to mitigate infection risk, manage edema, and optimize circulatory health to enhance surgical outcomes.
Importance of Vascular and Infection Assessments: Ensuring proper blood flow is pivotal in the pre-operative phase. Vascular assessments must go beyond basic non-invasive tests to include comprehensive arterial duplex imaging; also consider pre-surgical vascular consultations to address any concerns about limb perfusion. Accurately diagnosing and managing any infections before surgery is vital; thorough assessments involve clinical evaluations, lab work, and imaging where CT scans are preferred over MRIs due to the latter’s potential to misdiagnose Charcot as osteomyelitis. The objective is to mitigate infection risk, manage edema, and optimize circulatory health to enhance surgical outcomes.
Assessing Soft Tissue Complications
Identifying Infection: Clinical and Laboratory Methods: When a Charcot patient presents with soft tissue complications, the primary investigation should focus on determining if there is an infection. This includes assessing the clinical appearance of the wound, conducting laboratory tests, and considering imaging options. White blood cell labeled bone scans or MRIs are valuable tools for identifying osteomyelitis, however neither is completely definitive. Gathering cultures and biopsies from the operating room provides direct insights, and taking an antibiotic holiday of at least 2 weeks before a definitive bone biopsy is advised. Cultures should be comprehensive, covering aerobic, anaerobic, acid-fast bacteria, and fungal types.
Role of Imaging in Diagnosis: Imaging plays a critical role in diagnosing soft tissue complications. Despite being a common choice for detailed imaging, an MRI may not reliably differentiate between Charcot changes and infections such as osteomyelitis, leading to a potential misdiagnosis. For evaluation of the deformity and bone quality, CT scans are preferred.
Evaluating Biomechanical Considerations: Addressing underlying biomechanical issues is essential for long-term success in treating soft tissue complications. Often, recurring wounds are not just soft tissue problems but signify biomechanical instability or deformities that need correction. For example, lack of plantar flexion or previous surgical failures may necessitate procedures like ankle fusion to rectify the problem and achieve sustainable healing. Surgical interventions should thus complement biomechanics to prevent wound recurrence and support overall structural stability.
The Reconstructive Elevator Concept
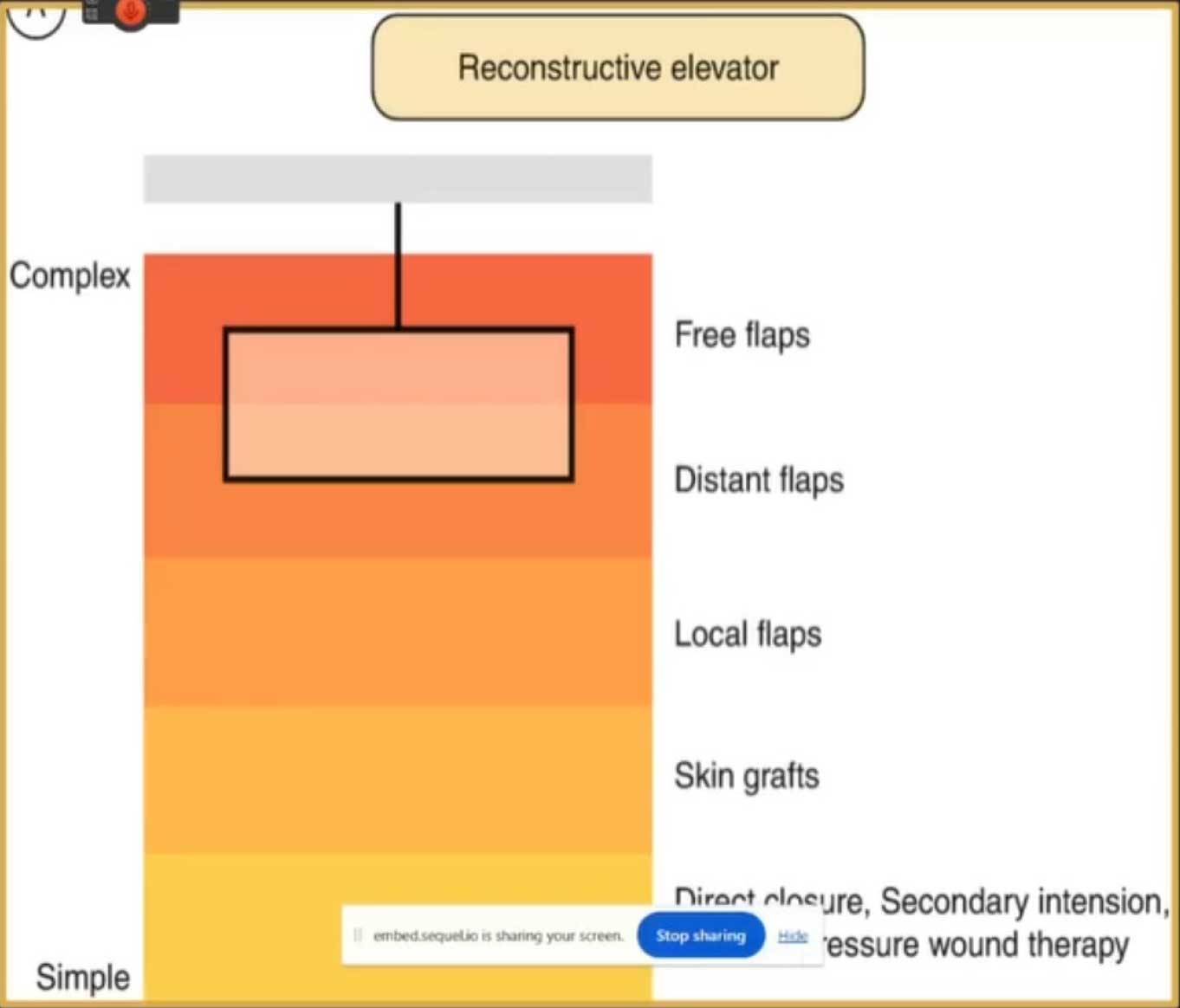
Source: Suh YC, Suh HP, Hong JP. Soft-Tissue Injury. In: Hong SK, Kim D, Jeon S. (eds) Primary Management of Polytrauma. Springer, Singapore. https://doi.org/10.1007/978-981-10-5529-4_8. ©2019.
When managing Charcot soft tissue complications, the “reconstructive elevator” framework provides a strategic and tiered approach to selecting surgical techniques. This concept allows healthcare professionals to begin with simpler methods and progress to more advanced techniques as needed, optimizing the treatment process for each unique case.
Initial Options: Dermal Grafts and Local Flaps: The initial steps in the reconstructive elevator focus on dermal grafts and local flaps. Dermal grafts provide a scaffold for vascular growth, thereby promoting healing. Specifically, placental grafts can be placed over exposed bone to initiate tissue regeneration, provided there is no infection. Simple techniques like these can sometimes accomplish the task without resorting to more complex procedures.
Local flaps, including advancement, transpositional, and rotational flaps, are valuable for their ability to close defects by mobilizing adjacent tissue. These techniques require a solid understanding of surgical principles and are considered workhorses due to their versatility in closing various defects.
Advancing to Fascia Cutaneous and Adipofascial Flaps: For small to medium defects, fascia cutaneous and adipofascial flaps offer reliable coverage with good blood supply. These flaps are beneficial for their aesthetic outcomes and lower donor-site morbidity compared to muscle flaps. A popular example is the reverse sural artery flap, which requires thorough pre-operative vascular evaluation, particularly regarding peroneal arterial blood flow. Understanding these flaps’ dependence on specific blood vessels is crucial to avoid complications such as venous congestion.
Complex Techniques: Muscle and Free Flaps: In cases requiring more robust support, muscle flaps provide substantial vascularity and bulk, making them suitable for covering exposed or infected bone. Despite their benefits, muscle flaps are limited in the foot and ankle due to their small size and rotation arc. It’s critical to understand muscle flap classification based on vascular supply to ensure success.
Free flaps represent the most complex reconstructive option, reserved for intricate cases and often necessitating a multidisciplinary team. They involve transferring tissue with its vascular supply to a recipient site, usually requiring vascular anastomosis, making them suitable for severe defects where simpler methods are inadequate.
Surgical Planning and Techniques
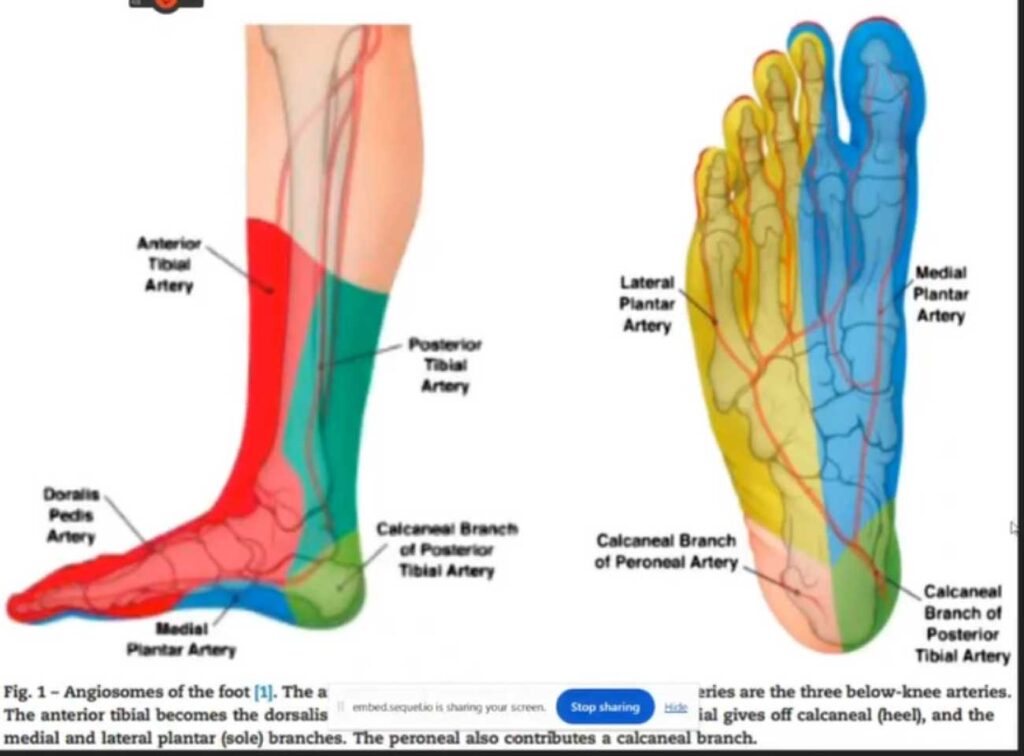
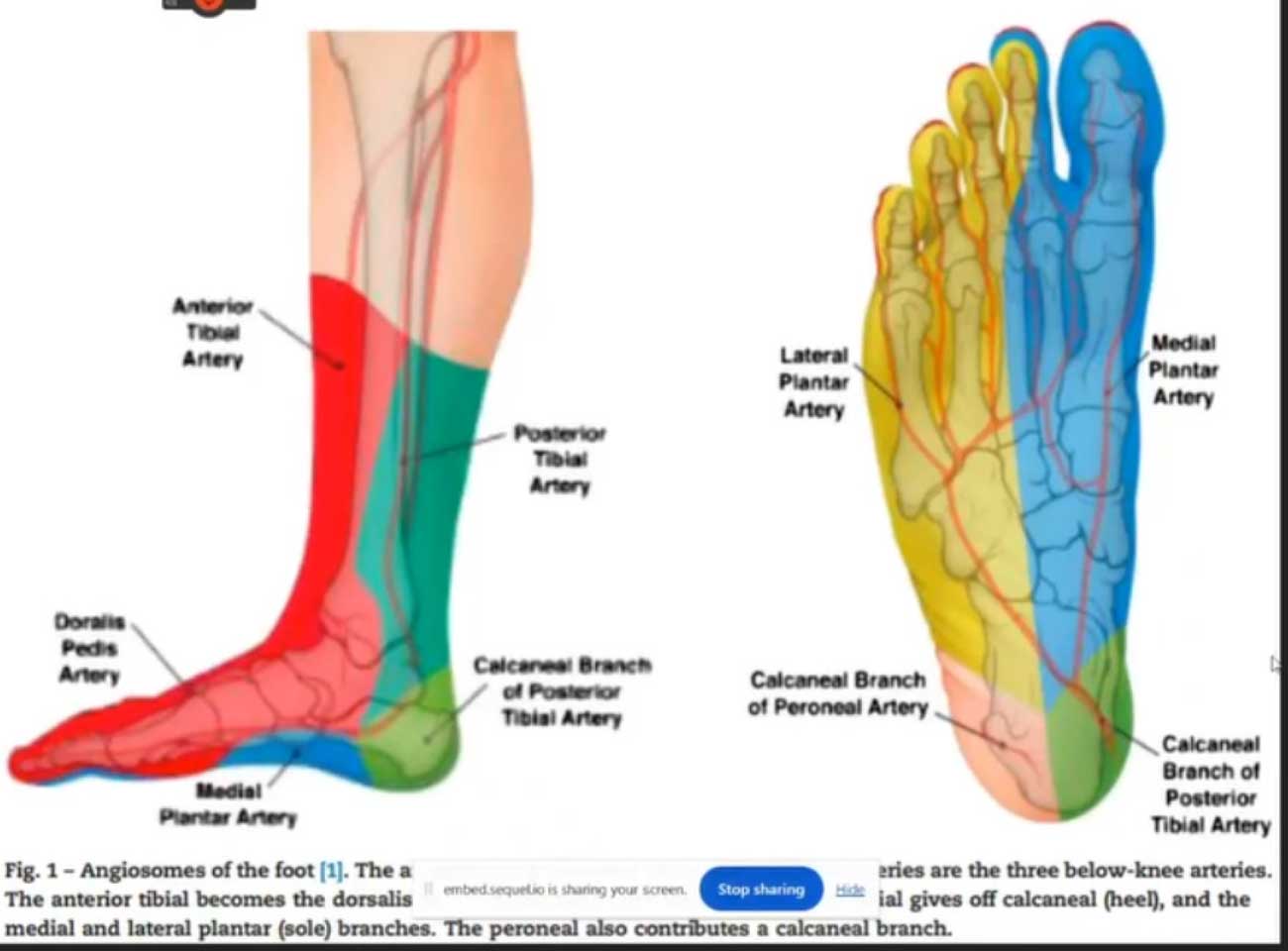
Successful management of Charcot soft tissue complications heavily relies on comprehensive surgical planning. Selecting incision sites that respect the patient’s unique vascular anatomy is paramount. Utilizing the concept of angiosomes and choke vessels–natural blood pathways–ensures optimal blood flow to healing tissues. For this reason, incisions are ideally placed within angiosomes, avoiding areas with compromised blood supply.
Minimally Invasive Surgery (MIS) techniques are also recommended to minimize incision size, which can reduce subsequent soft tissue complications. In addition, pre-operative planning should address any underlying biomechanical issues to prevent recurrent soft tissue breakdown. Proper assessment and staging of existing infections, through clinical examination and appropriate imaging, ensure that surgical interventions are appropriately timed and likely to succeed. By integrating these considerations, surgeons can effectively manage soft tissue complications, ultimately enhancing patient recovery and reducing the risk of recurrence.
 A Comprehensive Approach
A Comprehensive Approach
Managing Charcot soft tissue complications demands a multifaceted and systematic approach that emphasizes prevention, assessment, and strategic intervention. Proactively optimizing a patient’s overall health–including managing comorbid conditions, conducting comprehensive lab and vascular workups, and ensuring smoking cessation–lays a solid foundation for minimizing complications. When soft tissue issues arise, assuming and thoroughly evaluating for infection is critical, utilizing advanced imaging, lab tests, and biopsy/cultures to confirm the presence and nature of infections.
The concept of the “reconstructive elevator” guides clinicians in selecting appropriate interventions, beginning with simpler techniques such as dermal grafts and local cutaneous flaps, and progressing to more advanced methods like fascial cutaneous or free flaps when necessary, allowing movement to the most appropriate treatment even if it is more advanced. Addressing underlying biomechanical problems is crucial for the success of soft tissue repair and to prevent recurrence. By employing careful surgical planning, which includes precise incision placement and the potential use of MIS, healthcare providers can achieve optimal outcomes in managing Charcot neuroarthropathy complications.
Kelsey J. Millonig, DPM, MPH, FACFAS, is double-board certified fellowship trained foot and ankle surgeon with the East Village Foot and Ankle Surgeons in Des Moines, IA. She completed her medical education at Des Moines University earning dual degrees in Doctor of Podiatric Medicine and Masters in Public Health. She was the first podiatrist in the world to be selected as a research intern at the World Health Organization Headquarters in Geneva, Switzerland. Dr. Millonig completed her surgical residency at Franciscan Foot and Ankle Institute in Seattle, WA. She then completed her complex deformity correction and orthoplastic reconstructive fellowship at the Rubin Institute of Advanced Orthopedics International Center for Limb Lengthening in Baltimore, MD.
Dr. Millonig has served as a global health medical missionary in several countries including the Yucatan Crippled Children’s Project and Uganda Clubfoot Care Project. She is also a fellow member of the International Foot & Ankle Foundation. She has authored multiple articles in medical journals and textbooks. Dr. Millonig frequently lectures nationally, has earned several scholarly awards, and held multiple leadership positions in numerous national podiatric and public health committees with the American College of Foot and Ankle Surgery, American Public Health Association, American Podiatric Medical Association, and American Association for Women Podiatrists.
Dr. Millonig offers expertise in limb deformity correction and limb lengthening including congenital and pos-traumatic conditions, orthoplastic reconstruction, nerve injury, minimally invasive surgery, and neuropathic limb salvage.
This article is a summary of Dr. Millonig’s presentation titled, “Management of Charcot Soft Tissue Complications,” from the APMA Surgical Complications Virtual Seminar, January 18, 2025. To view the 20-minute slide presentation with questions and answers, visit https://apmasurgical.lerexpo.com/. Continuing education credits are available for many lerEXPO programs.





