
By Astrid Ustad, Karen Sverdrup, Gro Gujord Tangen, Øystein Døhl, Beatrix Vereijken, Pernille Thingstad, and Nina Skjæret-Maroni
Physical activity is a modifiable lifestyle factor that is well established as an important determinant for maintaining function and independence in daily life, and thus is imperative for healthy aging.

The 2020 recommendations from the World Health Organization (WHO) highlight that every minute replacing sedentary behavior (SB) with physical activity (PA) of any intensity has health benefits. This has led to a shift from focusing on achieving moderate-to-vigorous PA toward awareness concerning the complementary importance of low-intensity PA and its potential role in reducing sedentary time, which are both feasible and safe for most older adults and have been shown to be associated with lower risk of all-cause mortality. Accurate, clinically meaningful estimates of daily PA among older adults can inform targeted interventions to maintain function and independence. This study describes daily PA in older adults across levels of care as a first step contributing to the limited evidence on potential associations between PA and the use of care services.
Methods
This study used data from the Trondheim 70+ cohort in the population-based Norwegian Trøndelag Health Study (The HUNT Study), which is 1 of the largest health studies ever performed. In total, 1,042 participants age 70 years or older with valid activity data were included. PA was assessed using 2 accelerometers over 7 consecutive days and was classified into PA (walking, standing, running, and cycling) and sedentary behavior (sitting and lying). Data on received care services were retrieved from municipal registers and participants were classified into 4 levels of care: 1) independently living (n = 853, 81.9%); 2) independently living with low-level homecare services (n = 68, 6.5%); 3) recipients of homecare services (n = 62, 6%); and 4) nursing home residents (n = 59, 5.7%). Time spent in the activity types and duration of bouts are presented across levels of care.
Results
Participants’ mean age was 77.5 years (range: 70.1–105.4, 55% female). In the groups with higher level of care, participants were older and more likely to be female, had lower physical and cognitive performance, and a larger proportion was diagnosed with mild cognitive impairment (MCI) and dementia. Across levels of care, significant group differences were found in the total time spent in PA, particularly in walking and standing. Indeed, PA was lower with higher age, as were number of walking and active bouts (Figure 1).
Daily PA, duration of active bouts, and number of daily walking bouts were lower for participants receiving higher levels of care. While standing was the dominant type of PA, walking appeared predominantly in short bouts at all care levels.
The highest number of walking bouts was achieved in the shortest duration category (10–30 seconds) and thereafter steadily fewer bouts in the longer duration categories (Figure 2b). For active bouts (including the activities walking, standing, running, and cycling), most bouts had a duration between 1 and 10 minutes at all care levels (Figure 2a). The daily number of active bouts with longer durations (10–60 and ≥ 60 minutes) were substantially lower at higher care levels.
Discussion
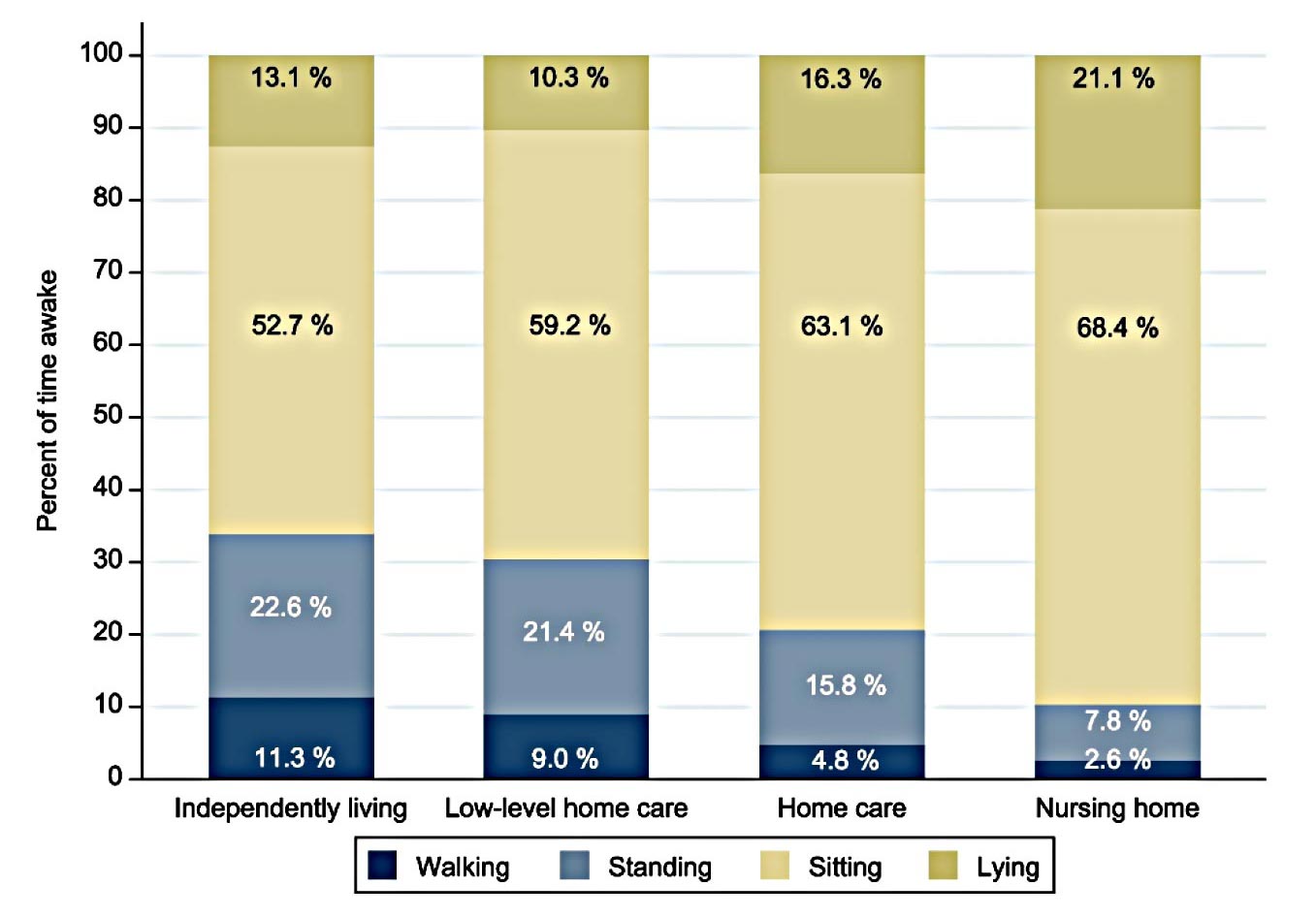
Figure 1. Distribution of activity types in percentage of time awake by level of care.
The results in this study revealed that low-intensity activities constitute the primary component of everyday PA in older adults. The total time spent in PA, particularly in walking and standing, were lower at higher care levels compared to independently living older adults, as were duration of active bouts, and number of daily walking bouts. Furthermore, standing was the dominant type of PA and walking appeared predominantly in short bouts at all care levels.
The current study showed that standing was the primary type of PA in older adults. While previous studies mainly focused on intensity or SB, few have classified activity types in older adults using wearable sensors. Classifying physical behavior into activity types can provide accurate estimates of both low- and higher-intensity PA, which can be used to further elaborate recommendations for daily PA in older adults.
The current study introduces a new perspective on how older adults accumulate PA by examining bout durations. By not capturing short bouts of standing and walking, earlier studies likely have underestimated PA, especially since self-reporting low-intensity activities is challenging due to the ubiquitous nature of daily living PA. Additionally, intensity-based cut-point approaches are limited in capturing short bouts, as they analyze data in longer epochs, typically 15–60 s, in contrast to the 5-s windows used in this study. Describing daily PA based on activity types and bout durations could be valuable in guiding future research on interventions aimed at reducing SB by providing more accurate estimates that capture even short bouts of PA.
The current study showed that there are substantial age and sex differences in daily PA in older adults. PA was lower with higher age for both sexes, but while men and women spent nearly equal time walking, women spent more time standing. This finding contributes important information for understanding daily PA among older adults.
Participants in the groups with higher levels of care were older, had worse cognitive and physical function, and were more often female compared to independently living participants. There was no significant difference in daily PA between the low-level homecare group and those living independently at home. Women spend about 35 min more time per day on PA than men. Therefore, the differences in daily PA across care levels are likely influenced by the higher proportion of women at higher care levels. These findings indicate that studies aiming to describe the association between daily PA and care level should consider these factors. As a first step in contributing to the limited evidence on daily PA related to the use of care services, the current study provides clinically relevant measures of PA in older adults. These measures can be further used to investigate potential associations between daily PA and care services.
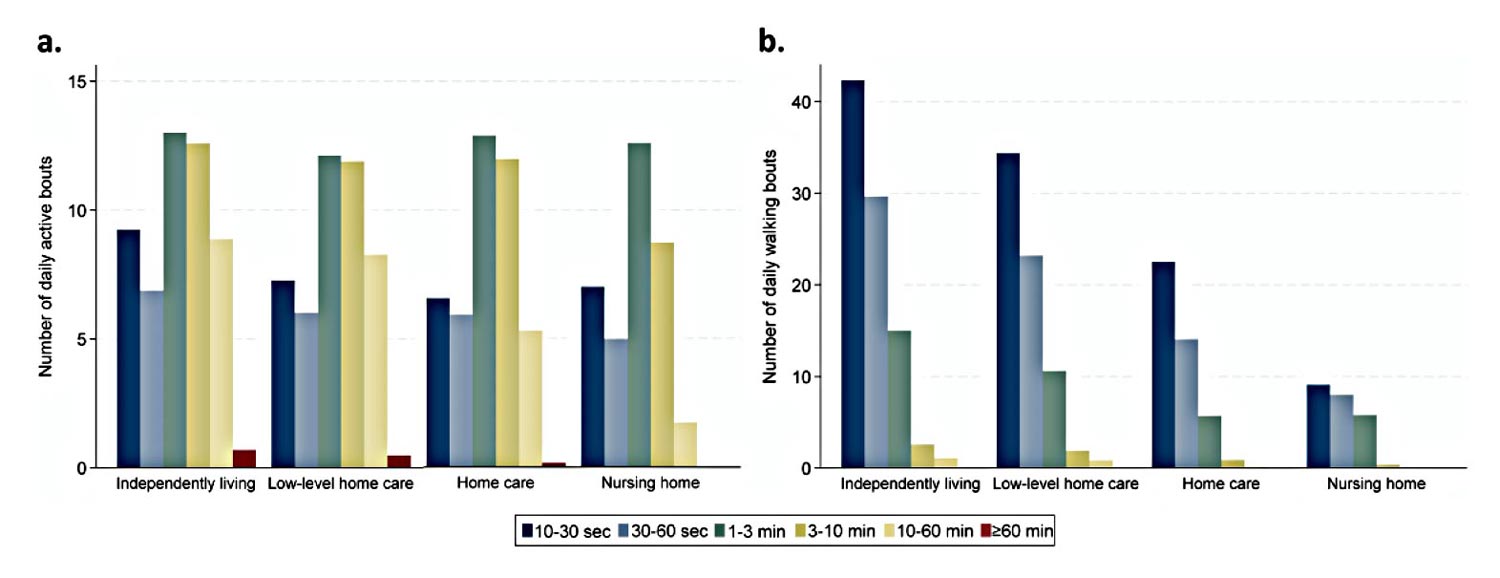
Figure 2. Number of daily active bouts (a) and number of daily walking bouts (b) in categories of bout duration by level of care. Walking bouts contain walking only, while active bouts contain the activity types walking, standing, running, and cycling. Note that the scale of the y-axis is different in the 2 plots.
Investigating not only the total volume of PA but also bout durations provide valuable information about daily activity in older adults, as the study authors observed that daily PA occurs over a wide range of durations. Walking bouts and active bouts, the latter also containing standing, should be seen in context to each other as both provide insight into patterns of accumulated PA in older adults. The study results showed that walking is distributed over many daily bouts and appears predominantly in short bouts lasting less than a minute, consistent with previous studies. The distribution of walking bouts showed a consistent pattern with gradually fewer bouts with longer lengths, although number of bouts were significantly lower with higher levels of care.
This study also showed that episodes of walking are significantly interspersed with episodes of standing in older adults. The lengthened durations of active bouts, and a considerably lower total number of active bouts compared to walking, reveals that periods of standing are a dominant component of upright activities in older adults’ daily life. Furthermore, this study showed that prolonged uninterrupted walking does not occur often. Independently living older adults averaged only about 1 daily walking bout lasting longer than 10 minutes, indicating that most older adults either do not engage in prolonged walks or break them up in shorter walking periods.
One of the most prominent differences between care levels was the lower number of walking bouts with higher levels of care, which was consistent across all bout duration categories. A larger number of bouts implies that individuals have more transitions between activity types, reflecting larger variation in daily PA, which previously was observed in individuals with better health status. The observed differences in daily PA variation between care levels might reflect individuals’ ability to live independently. This information could be clinically relevant in identifying individuals at risk of functional decline at an early stage and targeting interventions to help them regain or maintain their independence. This study showed that individuals living independently have higher variation in their daily PA than those receiving care services. This suggests that older adults unable to maintain variation in PA may be at risk of requiring care services. The potential of daily PA variation as indicator of functional decline together with targeted interventions focusing on increasing variation by breaking prolonged SB, should be further investigated in longitudinal studies.
Another interesting finding regarding indicators related to functional decline is the observed difference between the low-level homecare group, which receives only safety alarm and/or food service, and the homecare group. The first group did not differ substantially from independently living older adults, neither in total PA volume nor bouts. Although active bouts with durations up to 10 minutes were maintained in the homecare group compared to the low-level homecare group, a significantly lower number of active bouts lasting longer than 10 minutes was observed among those receiving homecare. This difference may indicate that those receiving a higher level of care have stopped going outdoors, and instead engage in everyday indoor activities of shorter durations. Individuals classified in the low-level homecare group may be well-suited for effectively implementing preventive measures. Implementing interventions at this stage aimed at preserving independence, such as increasing PA, may hold great potential for reducing or delaying the need for additional care services. This is crucial for maintaining independence and the quality of life for the individuals and their close ones. According to the findings in this study, prioritizing activity type–specific measures, especially those aimed at maintaining variation and active bout durations at this stage, may hold potential to reduce or delay the need for additional care services.
Conclusions
This study offers novel insights into daily PA patterns and addresses a current evidence gap concerning the free-living PA of older adults across levels of care. The current study shows that low-intensity activities constitute the primary component of everyday PA and advocates for placing larger emphasis on the significant role these activities play in maintaining daily PA at older age. As daily PA, duration of active bouts, and the number of daily walking bouts were lower with higher levels of care, these findings suggest that activity types and bout durations are related to the ability to live independently. These measures may be clinically relevant for assessing PA in older adults. Accurate estimates of daily PA among older adults can be used for evaluation of physical behavior and targeted interventions to maintain function and independence in older adults.
Astrid Ustad is a PhD candidate with the Department of Neuromedicine and Movement Science, Faculty of Medicine and Health Science, Norwegian University of Science and Technology (NTNU), Trondheim, Norway.
Karen Sverdrup, PhD, is a researcher with the Norwegian National Centre for Ageing and Health, Vestfold Hospital Trust and with the Department of Geriatric Medicine, Oslo University Hospital, Norway.

Gro Gujord Tangen, PhD, PT, is affiliated with the Norwegian National Centre for Ageing and Health, Vestfold Hospital Trust and with the Department of Geriatric Medicine, Oslo University Hospital, Norway. She is also an associate professor with Oslo Metropolitan University.
Øystein Døhl, PhD, is a researcher with the Department of Neuromedicine and Movement Science, Faculty of Medicine and Health Science, NTNU, Trondheim, and is affiliated with the Department of Finance, Trondheim Municipality, Norway.
Beatrix Vereijken, PhD, is a professor with the Department of Neuromedicine and Movement Science, Faculty of Medicine and Health Science, NTNU, Trondheim, Norway.
Pernille Thingstad, PhD, is a researcher with the Department of Neuromedicine and Movement Science, Faculty of Medicine and Health Science, NTNU, Trondheim, and is affiliated with the Department of Health and Welfare, Trondheim Municipality, Norway.
Nina Skjæret-Maroni, PhD, is an associated professor with the Department of Neuromedicine and Movement Science, Faculty of Medicine and Health Science, NTNU, Trondheim, Norway.





