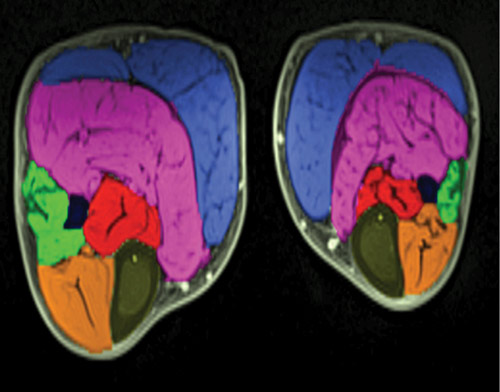
MRI images show the lower legs of a child with bi- lateral clubfoot. The smaller leg is the affected side, showing smaller muscles. (Image courtesy of Matthew Dobbs, MD.)
Analysis focuses on muscle deficits
By Erin Boutwell
Children with idiopathic clubfoot who have relapses after treatment with the Ponseti method demonstrate different soft tissue abnormalities than children whose clubfoot is permanently corrected, according to research published in the August issue of the Journal of Bone & Joint Surgery.
“Once we gain correction with the Ponseti method, we still have a number of kids who go on to have trouble with the deformity recurring,” according to Matthew Dobbs, MD, professor of orthopedic surgery at Washington University in St. Louis, MO, and study author.
Dobbs and colleagues recruited 20 patients with clubfoot who had previously undergone treatment using the Ponseti method of serial manipulation and casting. Patients were categorized as “treatment-responsive” (no relapses) or “treatment-resistant” (relapses that did not require extensive surgery), and had completed their final casting a minimum of one year prior to the study. The soft tissue composition of both limbs was evaluated using magnetic resonance imaging (MRI). Researchers measured the total cross-sectional area of the limb, as well as the relative amounts of muscle and fat, and, in unilateral patients, compared the affected and unaffected limbs.
In the six patients with unilateral treatment-responsive clubfoot, the affected limb had a 15.3% smaller mean cross-sectional area and 26.6% less mean muscle tissue than the unaffected limb. The five unilateral patients in the treatment-resistant group demonstrated a larger between-limb difference in intracompartment adiposity index (IAI, the ratio of fat tissue to overall soft tissue) than the treatment-responsive group. The treatment-resistant limbs were also characterized by more intracompartment fat tissue than the unaffected limbs. Further, these patients exhibited an even more pronounced between-limb imbalance in muscle tissue (47.8% less muscle tissue on the affected side than the unaffected side) than the treatment-responsive patients (26.6%).
Dobbs suggested that detecting soft tissue abnormalities such as muscle weakness or absence through physical clinical examination may permit more individualized prescriptions for children with clubfoot, in which casting and manipulation procedures could be personalized based on features of their individual presentation. Specifically, the findings of this MRI study may assist in identifying abnormalities associated with clubfoot presentations that are less responsive to the standard Ponseti method.
Jose Morcuende, MD, PhD, chief medical director of the Ponseti International Association, challenged the “treatment-resistant” label used within this study for cases of clubfoot that did not respond to the usual Ponseti method. Morcuende noted that, in an earlier study, co-authored by Morcuende and Dobbs and published in the October 2006 issue of Clinical Orthopaedics and Related Research, all but two of 50 “complex” idiopathic cases were successfully treated using the Ponseti method. The distinction between “resistant” and “complex,” Morcuende asserted, has more to do with the skill of the practitioner than differences in soft tissue characteristics: “It’s not the foot per se, but the hands of the doctors.”
Still, identification of children who are less likely to be treated successfully with the standard Ponseti method could be another advantage of detecting soft tissue differences.
“Knowledge of abnormalities in certain muscle groups…may lead one to increase the time in the post-corrective brace or, more likely, recommend early anterior tibial tendon transfer,” said Lewis Zionts, MD, a clinical professor of orthopaedic surgery at the David Geffen School of Medicine at UCLA.
Morcuende cautioned against using the MRI findings to recommend premature surgery for children whose soft tissue composition seems to predispose them to be resistant to Ponseti treatment.
“It will take you ten casts or twelve casts, but you can get those feet corrected,” he said.
A third possible benefit of knowing the soft tissue characteristics associated with clubfoot is a more reliable classification system to improve the prediction of treatment responsiveness, the need for which was mentioned by both Dobbs and Zionts.
“Unfortunately, current clinical examination techniques do not accurately predict the likelihood of the response to Ponseti treatment,” Zionts said.
Dobbs and his fellow authors anticipate that these MRI studies of soft tissue abnormalities may be used in the future development of a new clinical classification method for clubfoot, in which functional and structural characteristics of the affected limb are assessed.
“Our ultimate goal with this MRI study is to take it back to the physical exam, and turn this into a new classification system for clubfoot that’s going to be prognostic,” Dobbs explained, “because it shouldn’t be one global treatment for all clubfeet when all clubfeet are not alike.”
Erin Boutwell is a freelance writer based in Chicago, IL.
Sources:
Moon DK, Gurnett CA, Aferol H, et al. Soft-tissue abnormalities associated with treatment-resistant and treatment-responsive clubfoot: Findings of MRI analysis. J Bone Joint Surg Am 2014;96(15):1249-1256.

Ponseti IV, Zhivkov M, Davis N, et al. Treatment of the complex idiopathic clubfoot. Clin Orthop Relat Res 2006;451:171-176.





