
 By Benjamin Raud, Chloé Gay, Candy Guiguet-Auclair, Armand Bonnin, Laurent Gerbaud, Bruno Pereira, Martine Duclos, Yves Boirie, and Emmanuel Coudeyre
By Benjamin Raud, Chloé Gay, Candy Guiguet-Auclair, Armand Bonnin, Laurent Gerbaud, Bruno Pereira, Martine Duclos, Yves Boirie, and Emmanuel Coudeyre
These authors found a dose-response relation between body mass index and the clinical consequences of knee osteoarthritis. High physical activity level was associated with low BMI and contributes to preventing the clinical consequences of KOA.
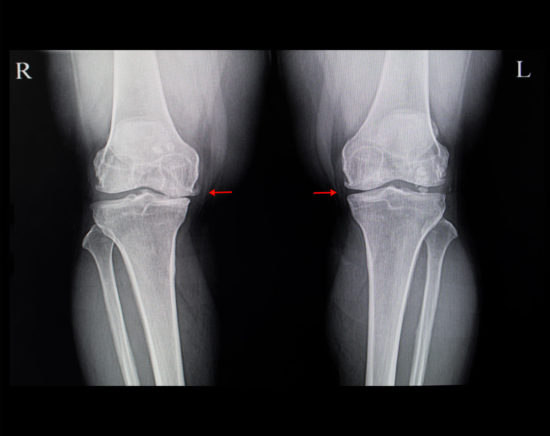
Osteoarthritis (OA) is the most common joint disease and one of the most prevalent symptomatic health problems. Knee osteoarthritis (KOA) leads to knee pain and altered joint function, with socioeconomic consequences. It generates a high proportion of health costs in many countries and has become a major public health issue. The health costs are directly related to KOA, such as knee replacement, or substantially by medication consumption.
In the many studies investigating the risk factors of KOA, overweight and obesity remain the most determinant even though they are considered modifiable. A recent meta-analysis showed a 5-unit increase in body mass index (BMI) associated with a 35% increased risk of KOA (relative risk [RR]: 1.35; 95% confidence interval [CI]: 1.21–1.51). BMI was positively associated with increased risk of KOA defined by plain radiography and/or clinical symptoms (RR: 1.25, 95% CI: 1.17–1.35) and clinical surgery (RR: 1.54, 95% CI: 1.29–1.83). Another study suggested a longitudinal association between weight gain and increased risk of symptomatic OA. The Framingham study showed an association of decreased BMI by ≥2 units at 10 years before examination and 50% decreased risk of OA for women. In another cohort study, a weight loss of >10% could reduce the clinical consequences of OA, finding a dose–response association between weight loss and pain or articular function.
Overweight and obesity are well known to increase the risk of KOA by mechanical load on weight-bearing joints. However, obesity or metabolic syndrome also increase the risk of hand OA. Hence, metabolic diseases, such as diabetes or metabolic syndrome, could have systemic effects on joints. A recent meta-analysis reported that type 2 diabetes mellitus may be a risk factor for OA whatever the location. Few studies have explored the association between obesity stage and KOA consequences on disability. A recent study showed that waist circumference could be one of the main risk factors for limiting ambulation speed in adults with KOA.
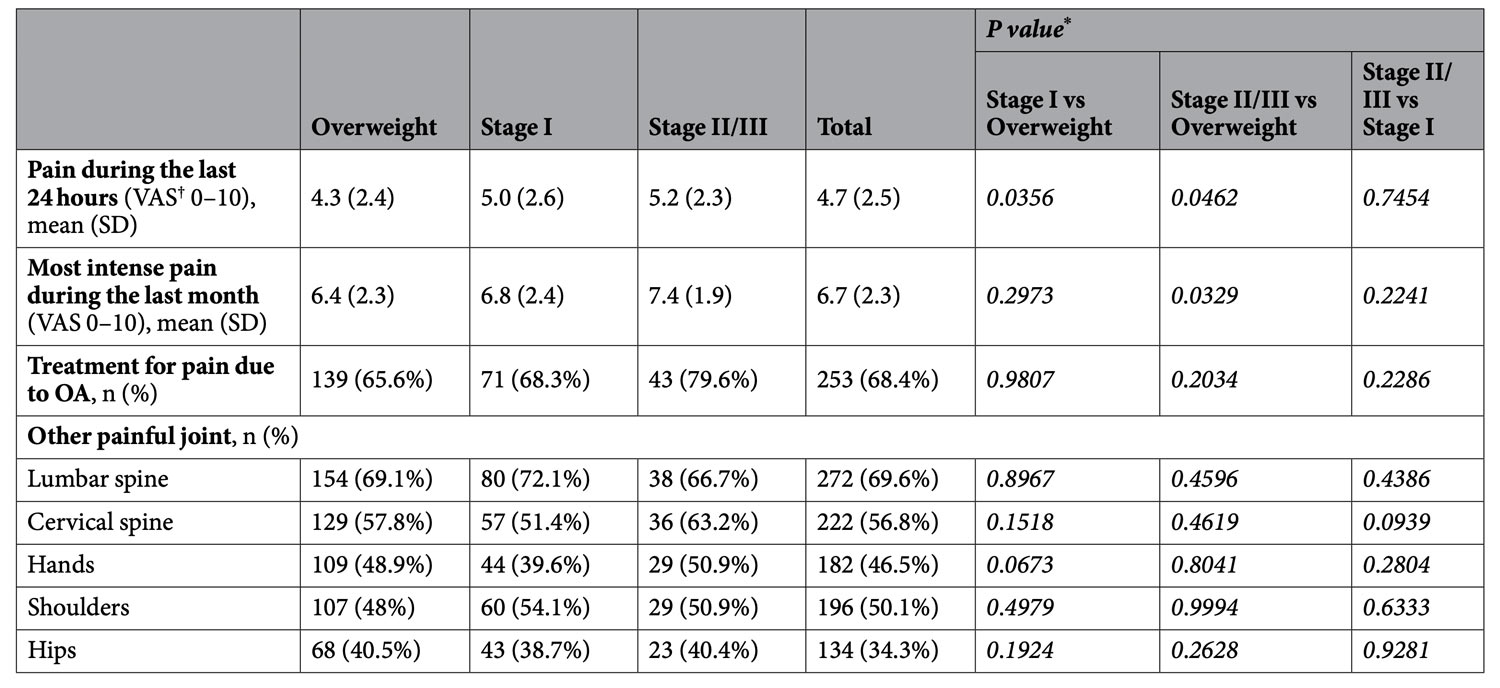
Table 1. Description of pain reported by participants. *Generalized linear mixed models with resorts as a random effect and adjusted for sex, age and number of comorbidities. †VAS: visual (0, no pain; 10, very severe pain).
Regular physical activity (PA) as well as caloric restriction can reduce the clinical consequences of KOA and potentially contribute to weight loss. However, the impact of BMI on level of PA in people with OA is unknown. A recent study measured the level of PA in a normal-weight population versus unhealthy and healthy overweight and obese participants. PA was lower for unhealthy overweight and healthy and unhealthy obese participants than healthy overweight and normal-weight participants. More specifically, a recent meta-analysis found that people with KOA were the least active according to PA guidelines. Other studies of KOA suggest that being overweight or obese is associated with lower quality of life and higher risk of disability and may affect knee joint impact rates and cause incremental pain. Also, overweight and obesity are risk factors for pain in the global population.
Despite obesity being a risk factor for KOA, we have few data on the association of obesity severity and its clinical and functional consequences. This study aimed to describe the association between KOA and BMI gradation in terms of pain, physical disability, level of PA, and fears and beliefs concerning KOA.
Methods
This study is part of a larger cross-sectional study of people with KOA older than 18 years of age that took place in France between September and November 2014 in 9 spa therapy resorts dedicated to OA. Every thermal establishment provided identical care for the patients, and procedures were similar for each center. For each patient, OA was the indication that led to prescribing spa therapy.
Participants were classified according to their BMI in three groups: overweight (BMI 25–30 kg/m2), stage I obesity (BMI 30–35 kg/m2) and stage II/III obesity (BMI ≥ 35 kg/m2). The groups were compared in terms of pain, physical disability, level of physical activity (PA) and fears and beliefs concerning KOA.
For specifics, see full article at https://www.nature.com/articles/s41598-020-60587-1.
Results
Participants: We included 391 individuals with BMI ≥ 25 kg/m2: 223 (57.0%) were overweight, 111 (28.4%) had stage I obesity, and 57 (14.6%) had stage II/III obesity. BMI groups did not differ by sex, age, OA duration and joint replacement. The mean number of comorbidities was 1.1 (SD 1.1) for overweight people as compared with 2.4 (SD 1.2) and 2.6 (SD 1.1) for stage I and stage II/III obesity groups (p<0.0001). The BMI groups significantly differed in terms of comorbidities for diabetes, hypertension, and anxiety or depression:
- 9.4%, 20.7% and 19.3% of the overweight, stage I and stage II/III groups, respectively, were followed up for diabetes (p = 0.0094);
- 34.5%, 51.4% and 56.1%, respectively, reported hypertension (p = 0.0011);
- and 14.3%, 18% and 29.8%, respectively, reported anxiety or depression (p = 0.0236).
- The BMI groups did not differ in terms of renal failure, gastrointestinal bleeding, physical impairment limiting activity, or cardiovascular disease.
According to the Osteoarthritis Research Society International (OARSI) phenotypes, 96.5% of stage II/III participants had polyarthritis with comorbidities profiles, as compared with 90.1% of stage I and 57.8% of overweight participants (p < 0.0001).

Table 2. Description of WOMAC, IPAQ and KOFBeQ scores. *Generalized linear mixed models with spa therapy resorts as a random effect and adjusted for sex, age and number of comorbidities. †Statistical test could not be used because of small numbers in stage II/III obesity group.
Pain. After adjustment for sex, age and number of comorbidities, pain intensity during the last 24 hours increased significantly with BMI gradation (p = 0.0367) (Table 1). For the most intense pain during the last month, only overweight and stage II/III groups differed significantly. Pain intensity during the last 24 hours was >4/10 for 46.8% of overweight individuals versus 60% for stage I individuals (p = 0.0493) and 65.5% for stage II/III individuals (p = 0.0343). Overall, 79.6% of participants with stage II/III obesity reported receiving treatment for pain due to OA versus 68.3% and 65.6% of stage I and overweight participants (p = 0.4199).
Participants reported another painful joint (Table 1), with no significant difference between groups.
Multiple-joint OA was reported by 91.5%, 90.1% and 96.5% of participants in overweight, stage I and stage II/III obesity groups, respectively.
Physical disability. [Based on Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) function scores] the BMI groups significantly differed in physical disability (p = 0.0409). The stage II/III obesity group was significantly more impaired than the overweight group (p = 0.0115).
Physical activity level. Using the short form of the International Physical Activity Questionnaire (IPAQ), we estimated continuous scores in metabolic equivalent minutes per week (MET-min/week) for vigorous, moderate, walking and total activity, as PA level (low, moderate or high). The IPAQ PA level and continuous score are described in Table 2. The PA level significantly differed among BMI groups (p = 0.0219). The proportion of participants with low and moderate PA level increased with BMI gradation and the proportion with high PA level decreased with BMI gradation. The BMI groups significantly differed by IPAQ continuous scores in MET-min/week: moderate activity (p = 0.0051), walking (p = 0.0201), and total activity (p = 0.0002). The walking and total activity continuous scores decreased with BMI gradation. Time spent sitting significantly differed among groups (p = 0.0025). The IPAQ moderate activity, walking and total activity continuous scores, such as time spent sitting, significantly differed between overweight and stage II/III obesity groups and between stage I and stage II/III obesity groups.
Fear and beliefs concerning KOA. Using the 11-item Knee Osteoarthritis Fears and Beliefs Questionnaire (KOFBeQ), five scores were estimated: a total score and 4 sub-scores for fears and beliefs about activities of daily living, physicians, disease, and sports and leisure activities. Higher scores indicate greater fears and beliefs; these are described in Table 2. The total score, daily activity score and physician score significantly differed among BMI groups (p = 0.0204, p = 0.0389 and p = 0.0413, respectively), with significantly higher scores for the stage II/III obesity group. The disease and sports or leisure activities scores did not differ between groups.
Discussion
This study describes the clinical consequences of KOA severity in a KOA population by level of obesity. We found a graded relation between obesity stages and clinical consequences of KOA. Indeed, the results showed a progressive increase between degree of obesity based on BMI and clinical consequences. Participants with higher BMI had higher pain scores, were more disabled, and reported more often anxiety and depression, which agrees with previous studies. In addition, the higher the obesity stage, the less the participant performed PA, which increases the risk of leading a sedentary lifestyle.

The relationship between obesity severity and OA onset has been largely described in the literature. But to our knowledge, this is the first study to describe the clinical consequences of KOA by degree of obesity. Indeed, most studies have determined these two components in all obese people but not by BMI category. Thus, given the size of our sample, we could distinguish overweight individuals from those with grade I or II obesity and higher. Another strength of this study is the amount of data collected. Indeed, a large number of clinical variables were analyzed, which provided a broader picture when assessing daily life consequences on KOA.
The three obesity groups did not differ in location of pain. These findings agree with the hypothesis of a “chronic micro-inflammatory state” that in conjunction with weight could play a major role in the initiation and perpetuation of OA. Weight loss would be the best way to decrease chronic inflammation by reducing inflammatory mediators and also reduce mechanical load on bearing joints. Individuals with high BMI are at increased risk of metabolic syndrome, which is based on the co-occurrence of multiple risk factors (hypertension, high lipid levels) or type 2 diabetes mellitus or coronary heart disease. Insulin resistance and micro-inflammation play a role in the development of chronic lesions. Micro-inflammation involved in the initiation and perpetuation of KOA is linked to level of insulin resistance, and insulin resistance is associated with the location and proportion of fat mass. Losing fat mass could play a major role in decreasing this micro-inflammation and reducing the clinical consequences of KOA.
We found the same gradual response between BMI and VAS pain score in the last 24 hours, which suggests higher pain for people with severe obesity and lower pain for overweight people. This finding may explain why weight loss may be directly associated with pain level and that the strategic approach to decrease pain could allow individuals to do more exercise. A recent study showed that in women with OA, disease-related pain was positively associated with cortisol production, particularly with greater pain intensity. Pain is a potential stressor and activator of the hypothalamic-pituitary-adrenal axis, which has been related to increased visceral obesity.
Strategies to control pain is a great part of the therapeutic proposition because it is a barrier to weight loss and PA. The psychological impact of obesity can be a barrier to PA and associated with severity of obesity. It could explain the association between BMI and the frequency of reported anxiety or depression. Strategies to increase the level of PA cannot be the same with different psychological profiles, which emphasizes the need for personalized medicine.
PA or rehabilitation is widely recognized as one of the first non-pharmacological lines of treatment for OA and is recommended for all patients. This study demonstrated that disability in patients with KOA, based on WOMAC function score, was associated with severity of obesity. With increasing obesity stage, OA increasingly led to altered function, thereby reducing the amount of PA performed, even though PA helps to improve function. Proposing PA as the first treatment aims to decrease fat mass, increase insulin sensitivity and decrease pain and micro-inflammation. However, we cannot expect severely obese individuals to do the same amount of PA as other people because they require psychological reinsurance. We found presence of anxiety and depression associated with BMI severity. This mental association with BMI severity should be more explored in future research, using validated instruments such as the Hospital Anxiety and Depression Scale (HADS) that evaluated the severity of anxiety and depression symptomatology. Obesity severity might be a stress factor recognized as a cardiovascular risk.
Concerning the representativeness of our sample, the individuals we studied are representative of samples studied in the literature and because of the high number of participants (n = 391), many different phenotypes of KOA were included. Indeed, the mean age was 67.3 years, and 71% were women. The mean WOMAC function score was 38.5. Our population was close in terms of age, sex and function to the 915 patients in the Tubach et al study.
Conclusion
We found level of obesity directly associated with clinical consequences of KOA, with a gradual dose–response relation by increasing BMI. High PA level was associated with low BMI and contributed to preventing the clinical consequences of KOA. The role of body fat mass in terms of clinical benefits of PA could be studied.
This article has been excerpted from “Level of obesity is directly associated with the clinical and functional consequences of knee osteoarthritis” by the same authors, which was published online Feb. 27, 2020, in the journal Scientific Reports. https://www.nature.com/articles/s41598-020-60587-1. Editing has occurred, including the renumbering of figures, and references have been removed for brevity. Use is per CC BY 4.0.





