lerEXPO Highlights
By Mark J. Mendeszoon, DPM
 Introduction: The Clinical Problem
Introduction: The Clinical Problem
Chronic mid-substance Achilles tendinosis is a common and challenging condition encountered by foot and ankle specialists. Unlike acute Achilles rupture, this disorder develops insidiously from repetitive microtrauma and progressive degeneration. Patients frequently report vague posterior ankle pain or a minor “tweak” that evolves into chronic dysfunction. Because successful management depends on accurate diagnosis and biomechanical correction, a firm understanding of Achilles anatomy, vascularity, and pathophysiology is essential. This piece synthesizes these foundational principles to clarify the nature of chronic mid-substance Achilles tendinosis.
Anatomy and Vascular Considerations
Gross and Functional Anatomy
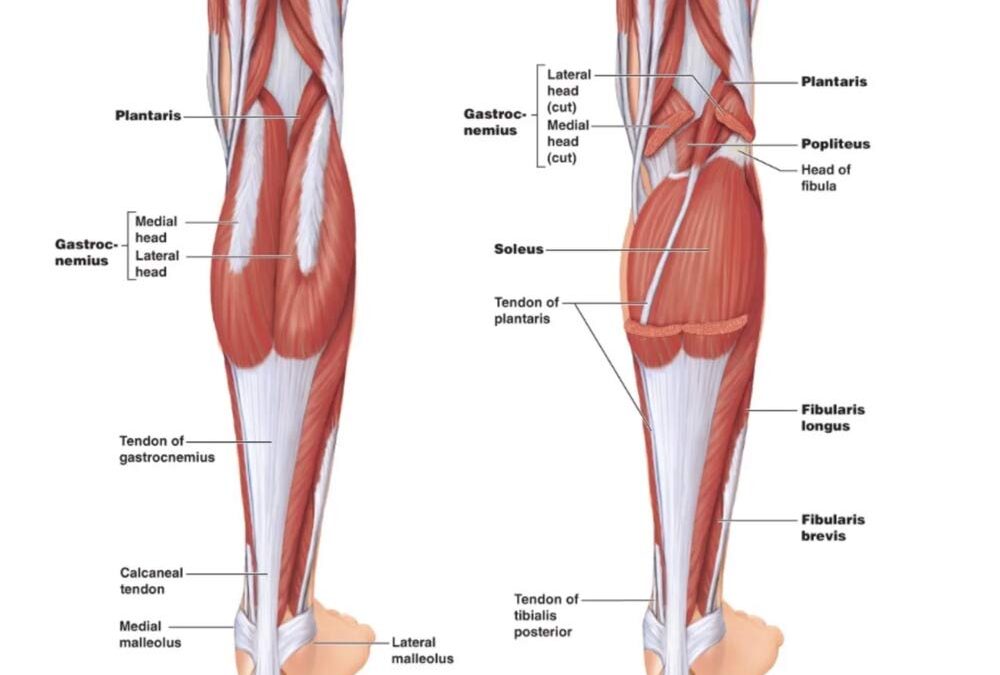
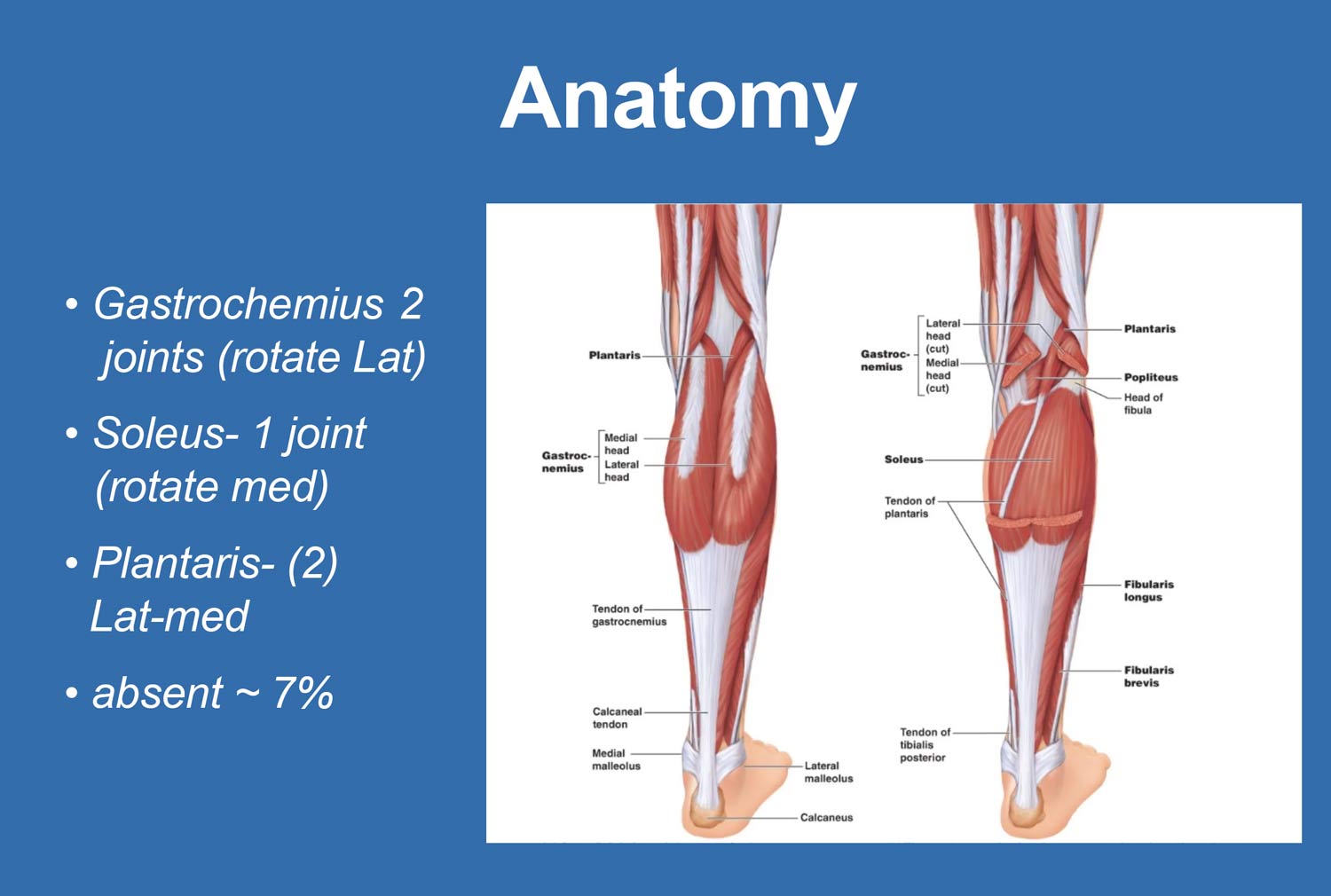
The Achilles tendon is formed by the confluence of the gastrocnemius and soleus muscles. The gastrocnemius, a biarticular muscle, contributes lateral rotational force, while the soleus, a monoarticular muscle, contributes medial rotation. These opposing forces create inherent torsion within the tendon during gait. The plantaris tendon, when present, plays a minimal role and is congenitally absent in approximately 7% of individuals.
Microscopic Structure
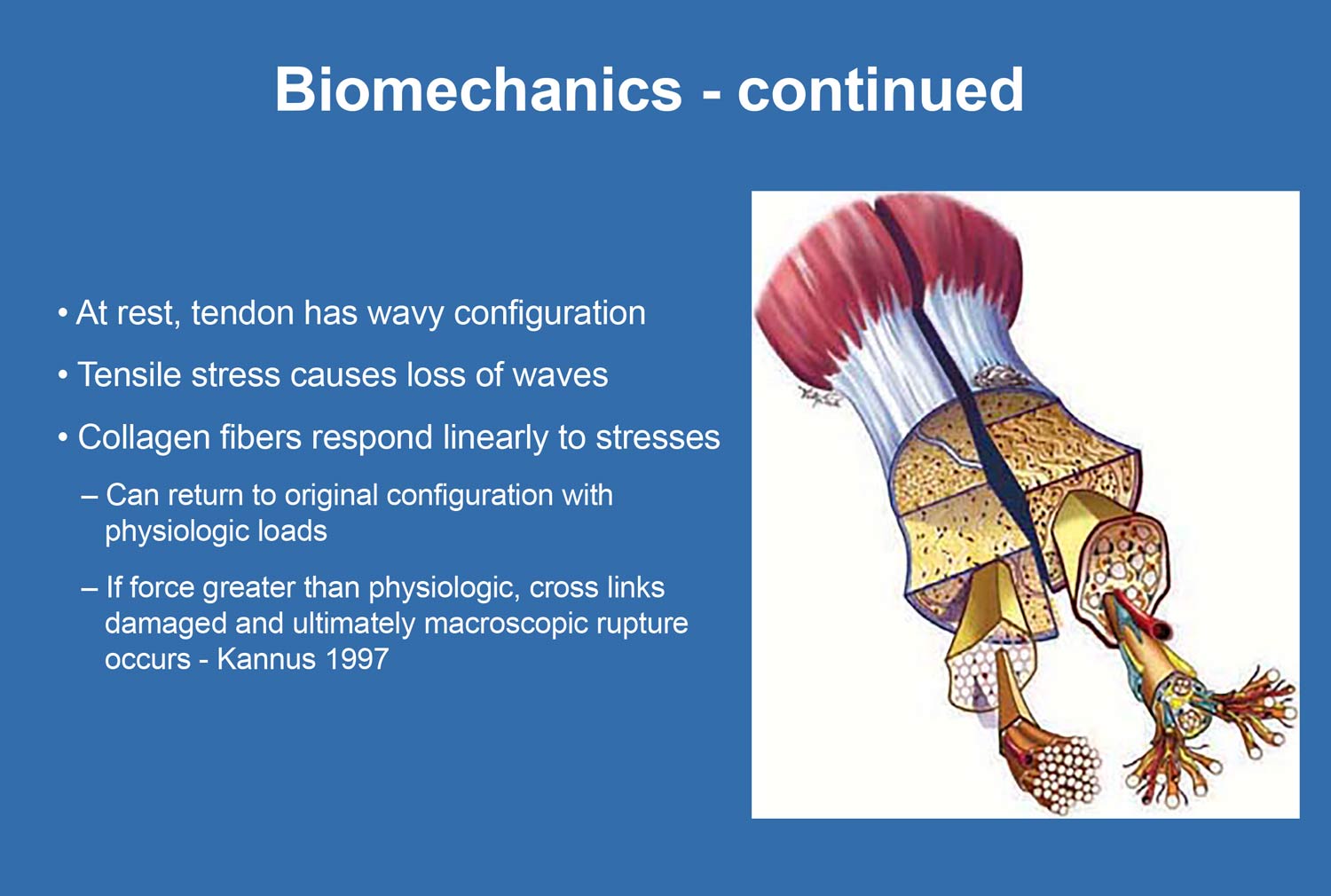
The Achilles tendon is composed of a hierarchical collagen arrangement designed for tensile strength. Collagen fibrils bundle into fibers, which form fascicles bound by endotenon. In healthy tendon, approximately 70% of the tissue consists of Type I collagen, arranged in parallel, linear, and characteristically wavy fibers that allow elasticity and load absorption.
Paratenon and Tendon Environment
Unlike tendons that change direction sharply and require a synovial sheath, the Achilles tendon follows a relatively straight course and is surrounded by a paratenon. This structure facilitates gliding but predisposes the tendon to paratenonitis rather than tenosynovitis, an important clinical distinction.
Vascular Supply and the Watershed Zone
The Achilles tendon has a limited blood supply, receiving circulation proximally from the musculotendinous junction and distally from the calcaneal insertion. Its most important vascular contribution arises from mesotenial vessels on the ventral surface. The area of poorest perfusion—the watershed zone—lies approximately 2–6 cm proximal to the calcaneal insertion. This hypovascular region corresponds to the most common site of degeneration and represents a biological weak point that limits healing capacity and predisposes the tendon to chronic tendinosis.
 Pathophysiology of Achilles Tendinosis
Pathophysiology of Achilles Tendinosis
Terminology Clarification
Chronic Achilles pain is frequently mislabeled as tendinitis, implying inflammation. Histopathologic evidence demonstrates that chronic mid-substance pathology is degenerative rather than inflammatory. The correct terminology is:
- Tendinopathy: A general term describing tendon pathology
- Tendinosis: A chronic intra-substance degenerative condition characterized by collagen disorganization and scar formation
Histopathological Changes
Healthy tendon demonstrates uniform, parallel collagen fibers with a wavy configuration. In chronic tendinosis, this structure is lost. Collagen fibers become disorganized, intersect irregularly, and stain basophilic, reflecting scar tissue formation. Notably, inflammatory cells are absent, confirming the degenerative nature of the condition.
Collagen Degeneration
A hallmark of tendinosis is the replacement of strong, organized Type I collagen with inferior Type III collagen. This transformation results in tendon thickening, reduced tensile strength, and diminished ability to tolerate physiologic loads. The structurally compromised tendon is therefore more susceptible to further injury and potential rupture.
Biomechanics and Etiology
Intrinsic Risk Factors
Intrinsic factors weaken tendon integrity and predispose individuals to degeneration. These include genetic collagen disorders (eg, Ehlers-Danlos syndrome) and exposure to medications such as fluoroquinolone antibiotics and systemic corticosteroids, both of which are associated with increased risk of tendinopathy and rupture.
Extrinsic and Mechanical Factors
Extrinsic factors are often the primary initiators of tendon injury and include repetitive overload, abrupt training changes, and inappropriate footwear. Runners who rapidly increase mileage or intensity are particularly vulnerable. These factors overwhelm the tendon’s adaptive capacity, leading to cumulative microtrauma.
Equinus as a Primary Deforming Force
Equinus, or tightness of the gastrocnemius–soleus complex, is a central contributor to Achilles tendinosis. Chronic tensile stress eliminates the tendon’s protective wavy collagen configuration, reducing flexibility and increasing strain. Accurate assessment requires examination with the foot locked in neutral or slight supination to avoid peroneal substitution. Management must include consistent static stretching, while ballistic stretching should be avoided due to the risk of further tissue damage.
Torsional and Pronatory Stress
The Achilles tendon functions in multiple planes. Due to opposing rotational forces from the gastrocnemius and soleus, the tendon experiences torsion with each step. Pathomechanics such as overpronation amplify this torsional stress, creating a sharp angle between the leg and foot during gait. Repetitive pronaetory torque places excessive rotational load on the tendon fibers, accelerating degeneration in the vulnerable mid-substance region.
 Clinical Evaluation and Diagnosis
Clinical Evaluation and Diagnosis
Patient Presentation
Patients with chronic mid-substance Achilles tendinosis typically present with:
- Localized mid-substance tendon pain
- Visible or palpable tendon thickening
- Decreased athletic or functional performance
Symptoms are often ignored initially, allowing progressive degeneration and scar formation.
Physical Examination
On examination, chronic tendinosis is characterized by thickened, fibrotic tendon tissue with minimal warmth or inflammation. This contrasts with acute injury, which presents with tenderness, crepitus, and inflammatory signs.
Imaging
Imaging supports clinical diagnosis and assesses severity:
- Radiographs may reveal intratendinous calcifications or ossification.
- Ultrasound effectively demonstrates fiber disruption and allows dynamic assessment.
- MRI provides detailed evaluation of tendon structure and is considered the gold standard, though often reserved for refractory cases due to insurance constraints.
Conclusion
Chronic mid-substance Achilles tendinosis is a degenerative condition arising from the interaction between compromised vascularity, intrinsic tendon structure, and repetitive biomechanical stress. The hypovascular watershed zone, collagen degeneration from Type I to Type III, and the cumulative effects of equinus and pronatory torsion form the foundation of this pathology. Recognizing tendinosis as a non-inflammatory process is essential for appropriate management. A thorough understanding of anatomy, biomechanics, and etiology allows clinicians to design targeted treatment strategies aimed at reducing pathological load, restoring function, and preventing progression or rupture.
Mark J. Mendeszoon is a multi-board-certified podiatrist who treats all surgical and non-surgical conditions of the leg, ankle, and foot in both adults and children. Specializing in trauma, sports medicine, diabetic foot and ankle conditions, and reconstructive foot and ankle surgery including Total Ankle Joint Replacement Surgery.
This article summarizes Dr. Mendeszoon’s presentation, “Cutting Edge Treatment of Chronic Mid-Substance Achilles Tendinosis,” delivered at the 2025 No-Nonsense Seminar (March 7–9). To view the full presentation with audience questions and answers–and to see the complete agenda for the 3-day program–visit https://nononsense2025.lerexpo.com. Continuing education credits are available for this and many other lerEXPO programs.






A good overview of the condition and there’s some great information on etiology/physiology but the title of the article says “cutting edge treatment” and there is no discussion about treatment options.