By Diego Ailton Prudêncio, Nicola Maffulli, Filippo Migliorini, Thiago Teixeira Serafim, Luis Felipe Nunes, Luciana Sayuri Sanada, and Rodrigo Okubo
Achilles tendinopathy (AT) is one of the most frequent overuse injuries in athletes, yet there is still a gap in the evidence for the efficacy of any modality of treatment in high-quality studies.
 Achilles tendinopathy (AT), a clinical syndrome characterized by pain, swelling, and loss of function, is one of the most frequent overuse injuries in the ankle and foot. In most patients, the condition improves with conservative interventions, the first line management option, which can be combined with a variety of other agents. Conservative therapies for the management of AT include kinesiotherapy, electrotherapies, cryotherapy, dry needling, bandaging, and splints. Exercise programs are the most widely studied interventions for the management of AT, and eccentric (the muscle contracts while being lengthened), concentric, isometric, and isokinetic contractions have all been used, alone or in combination. Surgery is generally undertaken when appropriately conducted conservative management has failed.
Achilles tendinopathy (AT), a clinical syndrome characterized by pain, swelling, and loss of function, is one of the most frequent overuse injuries in the ankle and foot. In most patients, the condition improves with conservative interventions, the first line management option, which can be combined with a variety of other agents. Conservative therapies for the management of AT include kinesiotherapy, electrotherapies, cryotherapy, dry needling, bandaging, and splints. Exercise programs are the most widely studied interventions for the management of AT, and eccentric (the muscle contracts while being lengthened), concentric, isometric, and isokinetic contractions have all been used, alone or in combination. Surgery is generally undertaken when appropriately conducted conservative management has failed.
While the evidence base for conservative therapy for AT continues to evolve, there is still a gap in the evidence for its effectiveness in high-quality studies. Toward this end, the study authors performed a systematic review and meta-analysis to investigate the efficacy of eccentric exercise (EE) in improving pain and function in adult patients with mid-portion Achilles tendinopathy compared to other forms of exercise.
Methods
A search was performed in PubMed, BIREME, SportDiscus, Cinahl, Web of Science, and PEDro, in November 2022. The search was limited to human studies published in Portuguese, English, or Spanish, due to the language capabilities of the researchers. The methodological quality was evaluated using the Risk of Bias 2 tool (RoB2) of the Cochrane collaboration, and the meta-analysis was performed using the Review Manager 5.1 program.
The study authors included randomized clinical trials (RCTs) with mid-portion Achilles tendinopathy in whom a program of EE was compared to another conservative modality, and in whom the outcome measure was assessment of pain and/or disability. Regarding the studies selection, the authors of this article were interested in identifying the effects and harms associated with an intervention.
A meta-analysis was performed to synthesize study data and verify the effect size of the intervention. Heterogeneity was tested by P value and I2.* If P > 0.10 and I2 < 50%, the heterogeneity was considered low enough to conduct a meta-analysis with a fixed-effect model. If P < 0.10, I2 > 50%, there was a high level of heterogeneity, and a random effect model was used. Sensitivity analysis was conducted by 1-by-1 exclusion method for individual studies. Descriptive analysis was performed if the heterogeneity was too large (I2 > 85%).
* Per Cochrane training materials, I2 informs the proportion of the variance in observed effect is due to variance in true effects rather than sampling error–it does not directly inform us abut the distribution of effects. A high I2 estimate is not necessarily synonymous with important heterogeneity.
 Results
Results
Of the 2,024 articles that were identified, 8 fulfilled the inclusion criteria, all of which were RCTs. The included studies reported a total of 401 Achilles tendons in 371 patients (54.2% male; ages 19–77, mean 46.6 years); 2 studies included individuals with bilateral and unilateral AT. Clinical examination (7 of 8) was the most common criterion for the diagnosis of AT; 3 studies used ultrasound, and 1 added the Victorian Institute of Sport Assessment-Achilles (VISA-A) questionnaire and the VAS pain scale to complete the diagnosis. All studies included only patients with tendinopathy of the main body of the Achilles tendon. The minimum duration of symptoms was 3 months.
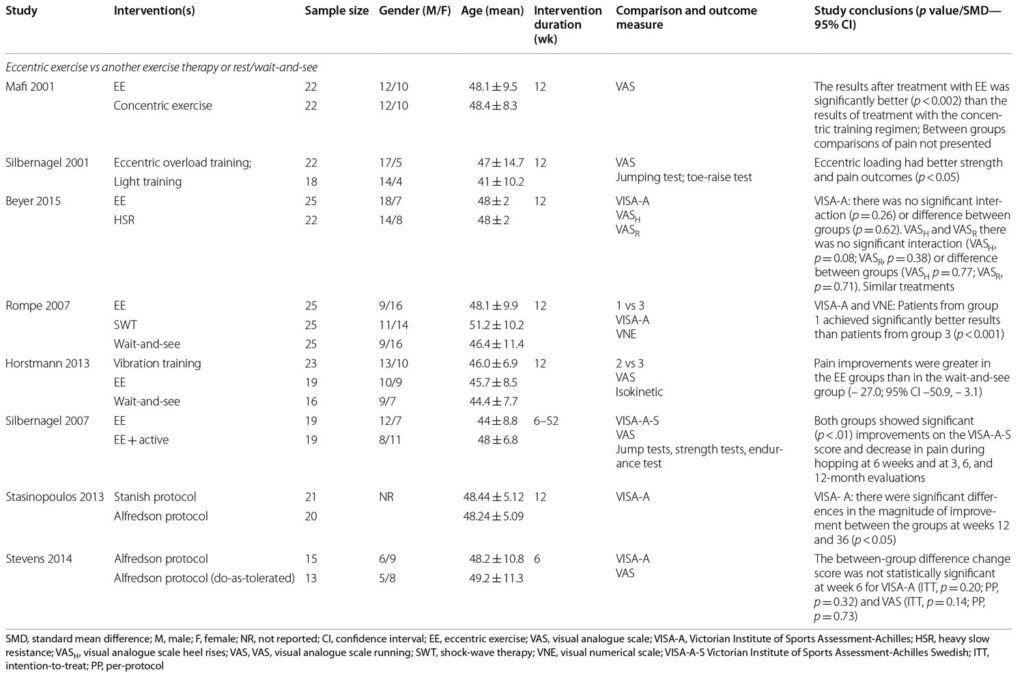
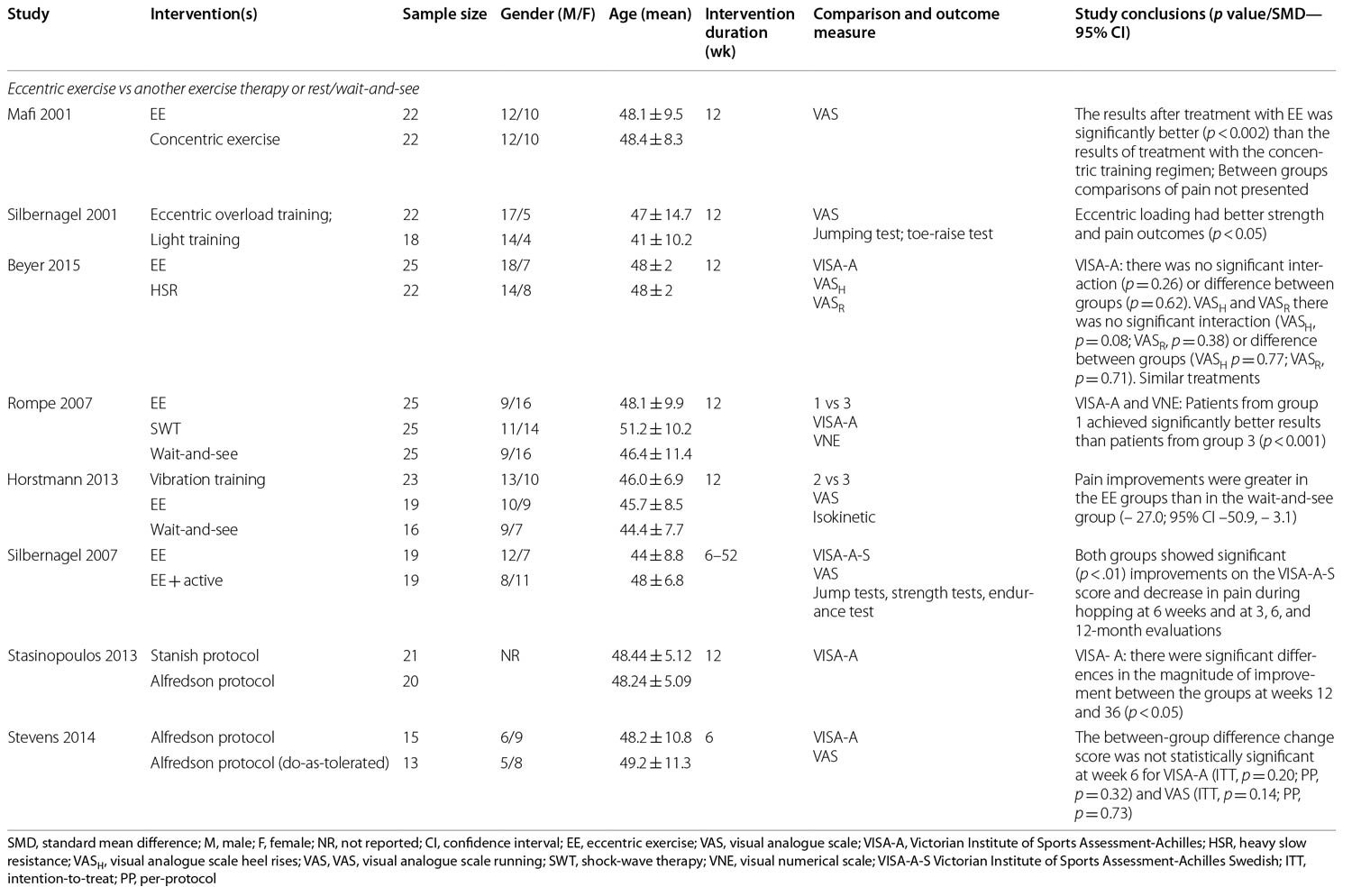
Six studies included 2 intervention groups: 1 was EE compared to another exercise modality, such as concentric exercise, light training, heavy slow resistance (HSR), and with another protocol of EE. Two articles included 3 groups: EE, electrotherapy, and wait-and-see and EE, vibration training, and wait-and-see. Most studies (75%) applied the intervention for 12 weeks. All articles evaluated change in pain; 7 verified function/disability; and 3 verified patient satisfaction with treatment.
Five of the studies used the VISA-A scale to assess pain and symptoms, 2 used functional tests (jump tests, toe-raise test, hop test, side-step test), 1 used isokinetic strength, and 2 assessed range of motion (ROM). One study also used the VISA-A to evaluate pain evolution. The other articles used the Visual Analogue Scale/Numerical Visual Scale (VAS/NVS). Most of the articles performed the evaluations at the beginning and end of the treatment, with 1 study undertaking follow-up at 36 weeks, 1 at 6 months, and 3 at 1-year. Four studies showed better outcomes in the EE treatment group, and 1 article did not present statistically significant differences. Among the 3 articles comparing 2 EE protocols, 1 presented better results with Alfredson et al’s1,2 protocol—a program of EE to treat AT while the uninjured limb is used to return (concentrically) to the initial position—and 2 did not find statistically significant differences between groups (Table 1).
The only variable for which a meta-analysis was possible was pain (5 articles), analyzed with the VAS/NVS and compared EE with another conservative treatment. RoB2 score showed 62.5% of the studies presenting “some concerns” and 37.5% (5 and 3 articles, respectively) presenting “high risk” of bias. The analysis of heterogeneity resulted in the I2 value of 91%, showing heterogeneity between the studies. The Mean Difference found in the treatment effect was − 1.21 (− 2.72 to − 0.30), with 95% confidence interval, with a significant positive effect for the treatment of pain in AT with EE, with the result in favor of EE compared to CG or other exercises in pain improvement (Figure 1). The rest/wait-and-see approaches do not provide significant benefits when compared to EE. In addition, controlled tendon loading can continue during the intervention, though further studies are needed to determine which activities are beneficial, and the recommended frequency and intensity.
Discussion
In the 8 studies evaluating the effect of pain and disability of EE with another type of exercise, 4 presented favorable EE results for pain, and 1 presented similar results between interventions. Regarding the effect on disability, 2 articles were in favor of EE.
One study investigated EE and concentric exercise. This study found improvement in pain and function/return to activity in both groups, with EE producing significantly better results, and suggested that EE produced significantly better results than concentric exercises because of the energy efficiency of eccentric exercises on the calf muscles, with comparable muscle force developed at lower loads on the tendon during movement. In addition, EE may produce changes in the metabolism of neural transmission in the tendon, inducing alterations in the perception of pain.
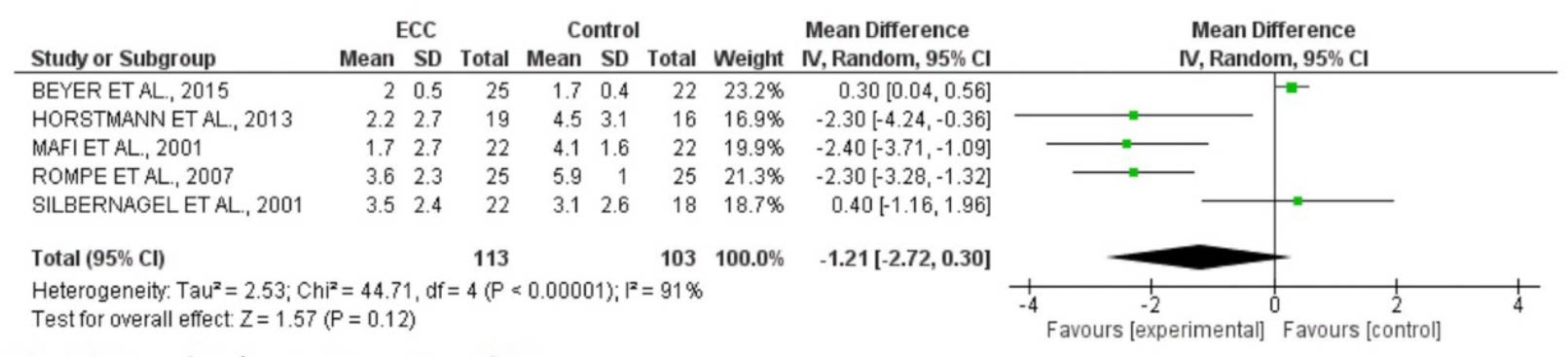
Figure 1. Meta-analysis for intervention with EE.
Two studies compared EE with rest/wait-and-see. The first studied verified improvement in pain and function of the EE group, which, despite not presenting a statistical difference, showed considerably better results than the control group. They reported a successful outcome in the EE group of 50% to 60% of patients, reporting that EE is inexpensive, although it is technique dependent. The wait-and-see protocol was the most convenient and easy intervention to implement, but also the least effective. The second study in this group showed significant improvement in the EE group, including a significant reduction in pain on palpation, compared to the control group. While interventions improved pain 2cm proximal to the insertion of the Achilles tendon in the calcaneus, only EE reduced pain at the musculotendinous junction as well. They reported that pain reductions following EE correlated with reduction in neovascularization in patients with tendinopathy, although such changes were not actually observed.
Silbernagel et al3 compared light training (eccentric plus concentric) and EE, and verified improvement in palpation, walking, and activity pain, as well as improvement in functional tests and ROM for the EE group, with no statistically significant differences between the groups. The authors also reported that the exercise load has to be relatively high for better results. Beyer et al4 presented a comparison of the EE and HSR groups. Both interventions showed significant gains in improving physical activity and pain, but without statistical difference between groups: the treatments are similar to each other, although patient satisfaction tended to be higher after 12 weeks with HSR (100%) than EE (80%).
Three studies compared EE with EE. The first applied the same treatment protocol, but only 1 group was released for physical activity. Both groups presented improvement in pain and function during the evaluations, with no statistically significant differences between the groups. The study demonstrated no negative effects in patients who continued physical activity (such as running and jumping) when using pain monitoring during rehabilitation and the authors believe that important factors in tendon improvement are intensity and type of load. The second study compared Alfredson’s and Stanish’s protocols. The former reduced pain and improved function to a greater extent than the latter. The protocol recommends the completion of 180 eccentric repetitions per day, and has been widely adopted in research and clinical practice. Stanish et al’s5 protocol for the management of AT includes eccentric and static stretching exercises and is based on 3 principles: length, load, and contraction velocity. According to the study authors, the protocol by Alfredson et al1,2 reduced pain and improved function more efficiently because patients exercised both calf muscles (gastrocnemius and soleus) only eccentrically, with more series and with more repetitions every day for the same treatment period. In addition, the load of EE in the Alfredson’s protocol1,2 was increased according to the patients’ symptoms, and the exercises were performed at low speed, which is supposed to allow suitable tissue adaptation.
The third study applied only the Alfredson’s protocol.1,2 One group was asked to perform 180 repetitions, and the other performed until tolerated. A statistically significant difference was found for improvement in function in each group at 3 weeks and for pain in the “do-as-tolerated” group; statistically significant differences between the groups in improvement of function were evident at week 3, but by 6 weeks there was no statistical differences between the groups for pain and function.
Conclusion
The available evidence supports the use of EE in the management of AT. Continuous load on the Achilles tendon does not adversely affect the results of pain and function, suggesting the possibility of practicing some physical activities during the intervention. Some of the studies analyzed herein report that EE and HSR produce similar results, but more studies are needed to confirm this. Also, the rest/wait-and-see approaches probably do not play a role in the management of AT.

- Alfredson H, Pietila T, Jonsson P, Lorentzon R. Heavy-load eccentric calf muscle training for the treatment of chronic achilles tendinosis. Am J Sports Med. 1998;26:360–6.
- Stevens M, Tan C. Effectiveness of the Alfredson protocol compared with a lower repetition-volume protocol for midportion Achilles tendinopathy: a randomized controlled trial. J Orthep Sports Phys Ther. 2014;44:59–67. https://doi.org/10.2519/jospt.2014.4720.
- Silbernagel KG, Thomeé R, Thomeé P, Karlsson J. Eccentric overload training for patients with chronic Achilles tendon pain—a randomised controlled study with reliability testing of the evaluation methods. Scand J Med Sci Sports. 2001;11:197–206.
- Beyer R, Kongsgaard M, Kjær BH, et al. Heavy slow resistance versus eccentric training as treatment for achilles tendinopathy: a randomized controlled trial. Am J Sports Med. 2015. https://doi.org/10.1177/0363546515584760.
- Stanish WD, Rubinovich RM, Curwin S. Eccentric exercise in chronic tendinitis. Clin Orthop Relat Res. 1986;2085:65–8.





