
 By Dr. Jennifaye V. Brown
By Dr. Jennifaye V. Brown
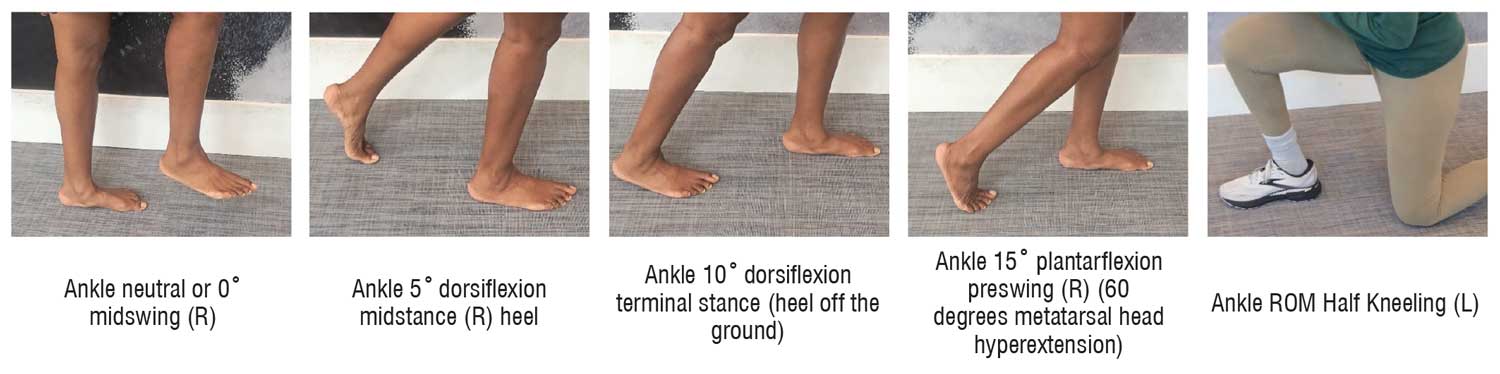
McCormick et al1 have described surgical interventions to restore ankle range of motion (ROM) due to foot drop and physicians conducted a thorough review of and outcomes of these different approaches. Throughout the article, the focus was on restoring to neutral or zero degrees of ankle dorsiflexion in hopes of not having to use ankle foot orthosis (AFO). The purpose of the AFO is to position the foot so that it is parallel to the floor during swing phase which is the only time it is normally held isometrically at 0 degrees of talocrural joint dorsiflexion.2-4 Otherwise, the AFO should provide ankle stability in stance phase during which the ankle ROM varies between 5 degrees of plantarflexion (loading response), 5 degrees of dorsiflexion (midstance), 10 degrees of dorsiflexion (terminal stance) and 15 degrees of plantarflexion (preswing) via eccentric or concentric muscle activity, the latter needed for push off at preswing.2-4 Additionally, individuals with foot drop need more than neutral talocrural joint dorsiflexion for other functional activities such as sit↔stand, getting up from the floor, squatting, and stair negotiation, particularly step over step.5 Furthermore, AFOs should be person-centered in that they reflect the personalities and function for activities engaged in during daily living.6-8
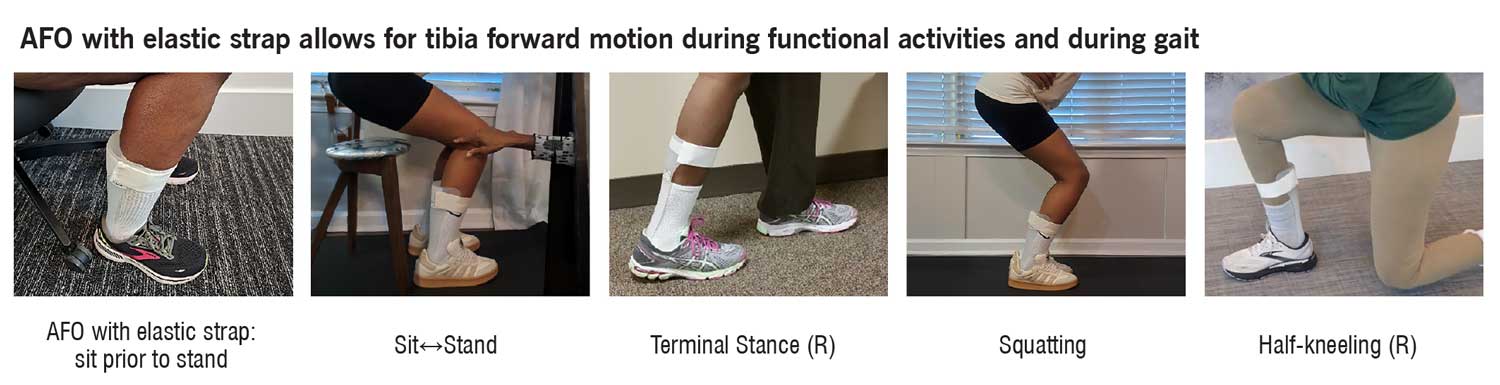
I have a suggestion for physical therapy practitioners who analyze daily activities and provide therapeutic interventions to achieve energy efficient and effective movement strategies for daily living skills. Simply, loosen the restrictive traditional AFO VELCRO® strap at the proximal tibia and or ankle joint or replace it with the appropriate tension of VELSTRETCH® that accommodates the muscle strength present. More elasticity for stronger muscles with isolated movement and less elasticity for muscles that cannot generate enough force to move segments of the lower extremity. Then proceed to practice gait on a variety of surfaces, sit↔stand, squatting, stair negotiation step over step, and getting up and down from the floor as these functional activities require tibial movement forward and backward and the elastic tension strap allows for that movement. Create therapeutic exercises and or break down activities into component parts in which tibial movement occurs via concentric, eccentric and or isometric muscle activity as it pertains to specific segments of gait during stance and swing phase and those other functional activities. The exercise program should entail a flexibility component open and closed chain and the exercises should vary in type (weight bearing and non-weight bearing) and order (isometric, concentric and eccentric muscle contractions) as well as reflect the individual’s social determinants of health.9-10 Also, include neuromuscular retraining and an aerobic component of different intensities.9-10 For example, the exercises and physical activities for a mother with a newborn who wants to safely push the stroller without falling should be distinctly different for the retired elderly male who wants to return to golf with his caddy and walk 6 holes of the 12-hole course.
 Jennifaye V. Brown, PT, MSPT, PhD, NCS, CAPS is an American Physical Therapy Association 4-time 10-year board certified neurologic physical therapist in Charleston, South Carolina, specializing in stroke rehabilitation, specifically gait analysis and treatment, AFO design, and the redesign of lived spaces allowing individuals with disabilities to age in place. She is the author of the book, Brace Yourself: Everything You Need to Know About AFOs After Stroke.
Jennifaye V. Brown, PT, MSPT, PhD, NCS, CAPS is an American Physical Therapy Association 4-time 10-year board certified neurologic physical therapist in Charleston, South Carolina, specializing in stroke rehabilitation, specifically gait analysis and treatment, AFO design, and the redesign of lived spaces allowing individuals with disabilities to age in place. She is the author of the book, Brace Yourself: Everything You Need to Know About AFOs After Stroke.
-
McCormick KL, Patel D, Chien BY, Greisberg JK, Vulcano E. Surgical management of foot drop. Orthop Rev (Pavia). 2024;16:120047. Published 2024 Oct 3. doi:10.52965/001c.120047
-
Johnston TE, Keller S, Denzer-Weiler C, Brown L. A Clinical Practice Guideline for the Use of Ankle-Foot Orthoses and Functional Electrical Stimulation Post-Stroke. J Neurol Phys Ther. 2021;45(2):112-196. doi:10.1097/NPT.0000000000000347
-
Choo YJ, Chang MC. Effectiveness of an ankle–foot orthosis on walking in patients with stroke: a systematic review and meta-analysis. Sci Rep. 2021;11:15879. doi.org/10.1038/s41598-021-95449-x
-
Adams JM, Cerny K. Observational gait analysis a visual guide. Thorofare, NJ: SLACK Incorporated; 2018.
-
Hyodo K, Masuda T, Aizawa J, Jinno T, Morita S. Hip, knee, and ankle kinematics during activities of daily living: a cross-sectional study. Braz J Phys Ther. 2017;21(3):159-166. doi:10.1016/j.bjpt.2017.03.012
-
Vinci P, Gargiulo P. Poor compliance with ankle-foot-orthoses in Charcot-Marie-Tooth disease. Eur. J Phys Rehabil Med. 2008;44 (1): 27–31.
-
Brown JV, Best S, Suhr J. Ankle Foot Orthoses: The Impact of Appearance, Function, and Fit in Individuals with Stroke. Lower Extremity Review. 2021;13(11):39-50. Available at: https://lermagazine.com/cover_story/ankle-foot-orthoses-the-impact-of-appearance-function-and-fit-in-individuals-with-stroke
-
Brown JV, Cotton J, Best S, Suhr JA. Communicating key features of an ankle foot orthosis from a patient’s perspective: a case study. NSAH Journal. 2020; 17(1):6-20.
-
Adhikari SP, Tretriluxana J, Dev R, Eglitis E, Shrestha N, et al. FITT-CORRECT: Updated dynamic and evidence-based principle of exercise prescription. J Nov Physiother Rehabil. 2021; 5: 005-009.
-
Winstein C, Stein J, Arena R. Guidelines for adult stroke rehabilitation and recovery. Stroke. 2016; 47(6):e98-e169. doi:10.1161/STR.0000000000000098






This is a DYNAMIC master clinician doing some critical thinking! I am so happy that we have such a knowledgeable physical therapist clinician who really considers the individuals functional context in addition to their pathophysiology. It is not often that clinicians consider social determinants of health and the ICF model so fluidly in practice when designing AFOs. I wonder if she has a book?