
 Studies show that lower extremity amputation rates in patients with diabetes vary widely, sometimes even within individual healthcare systems. What’s more difficult to determine is why these variations exist and what can be done to improve access to care for all patients.
Studies show that lower extremity amputation rates in patients with diabetes vary widely, sometimes even within individual healthcare systems. What’s more difficult to determine is why these variations exist and what can be done to improve access to care for all patients.
By Larry Hand
Lower extremity amputation rates in patients with diabetes vary by geography, within individual healthcare systems, by costs, and by payer. But hard-and-fast reasons for the variation remain difficult to pin down scientifically, and many experts believe the best way to level the playing field is to do a better job of preventing amputations in all patients.
Hongjun Yin, PhD, assistant professor of pharmacy practice for the Georgia Campus-Philadelphia College of Osteopathic Medicine in Suwanee, GA, and colleagues analyzed patient and hospital data on lower extremity amputations among diabetic patients in 2007 and found, among other things, that expected factors such as age, race, and length of hospital stay accounted for only about 55% of cost variance.1That leaves more than 40% undetermined.
“Our paper identified some patient, hospital, and state-related factors that are related to inpatient cost variation associated with diabetes-related lower extremity amputation [DLEA]. We also found forty percent of the variations in DLEA hospital costs remain to be examined,” Yin wrote in an email to LER.

Yin and colleagues analyzed data from the 2007 US Agency for Healthcare Research and Quality Healthcare Cost and Utilization Project and obtained state-level data from the US Census Bureau and the Kaiser Family Foundation. They used regression models to explore inpatient costs and variables at patient, hospital, and state levels.
They found that, for 9066 diabetic lower limb amputations (66% male, 57% white, mean age 62 years), mean total cost came to $17,103 per patient. However, that ranged from $9381 in Tennessee to $23,282 in New York.
Lengths of stay ranged from 5.3 days in South Dakota to 19.3 days in Hawaii. Nevada had the lowest percentage of foot-level amputations compared with leg amputation at 52%, while South Dakota had the highest percentage of foot-level amputations at 80.1%.
The researchers linked patient and hospital factors, including age, race, length of stay, level of amputation, and hospital type, to 55.3% of the cost variance. As for state-level factors, only number of beds per hospital contributed to the variance.
“We found the greater the number of hospital beds per 10,000 residents, the lower the total cost. This may be a result of (a) competition, (b) economies of scale, or (c) that patient populations where more hospital beds are available may be admitted in an earlier stage of disease,” Yin wrote.
In-system variation
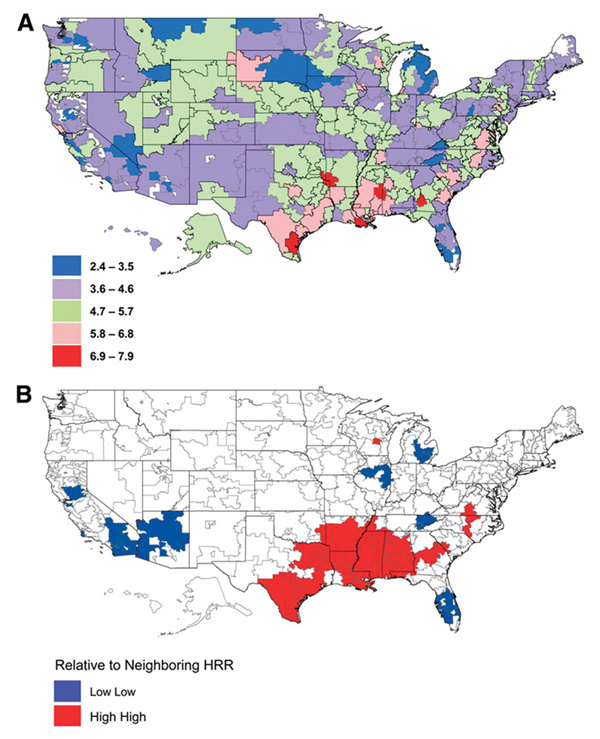
Maps of incidence of lower extremity amputations (LEA) among diabetic Medicare beneficiaries by hospital referral region (HRR) in 2008. A: Map of LEA incidence per 1000 persons on Medicare with diabetes by HRR in 2008. B: Local index of spatial autocorrelation map of LEA incidence showing spatially correlated HRRs of highest incidence of LEA and lowest incidence of LEA in 2008. (Reprinted with permission from reference 7.)
In a paper published in January this year in the Journal of Diabetes, researchers at New York University School of Medicine in New York City found that, despite a similar standard of care and equal access to care at three hospitals within their system (one independent hospital, one private hospital, and one Veterans Administration [VA] hospital), VA patients had higher amputation rates than the geographically adjacent public and private hospitals.2
“We infer that patient-specific risk factors explain the disparate amputation rates across these institutions,” the researchers wrote. They found that just the presence of a foot ulcer on initial presentation led to a “markedly increased rate of amputation.”
Also, the researchers wrote, presentation of more serious ulcers at the VA and public hospitals during the study period suggest that patients may have had obstacles to getting care prior to this study, even though studies3-6 have shown that VA patients get more foot care and diabetes education than other patients.
Neighborhood clusters
In a November 2011 study in Diabetes Care, David J. Margolis, MD, PhD, professor of dermatology at the Perelman School of Medicine at the University of Pennsylvania in Philadelphia, and colleagues found that lower extremity amputation rates among Medicare patients vary widely across the US and tend to cluster in neighborhoods with either high or low rates.7 They proposed that differences in preventive care and treatment decisions may have caused the variations.
“We found variation that was as much as three- to four-fold differences between different regions of the country, which is remarkable. If you look at other clinical findings and biochemical findings that are risk factors, or believed to be risk factors, for amputation, most will increase the risk fifty percent or even one hundred percent,” Margolis told LER. “We weren’t really able to make findings go away by adjusting for factors such as age, gender, or race, or just the incidence of diabetes.”

Margolis and colleagues, building on a similar study published in 2001,8 found that high rates of amputations occurred in clusters of neighborhoods in Texas, Oklahoma, Louisiana, Arkansas, and Mississippi. They also found that patient variables associated with amputation rates included socioeconomic status, percentage of African Americans, age, diabetes, mortality rate, and having a foot ulcer. Amputations were less common in areas with lower diabetes prevalence and more common in areas with a higher percentage of African Americans, higher prevalence of foot ulcers, and higher prevalence of mortality among patients with foot ulcers.
Margolis said he and his colleagues tried extensively to link such traditional factors as socioeconomic status, age, comorbidities, and race to rate variations but always came back to the conclusion that variations are based on location. (The title of their study begins, “Location, location, location…”)
Researchers now need to look at those areas with high amputation rates and low amputation rates, he said, “and see if physicians are trained differently or if patients have different understandings of their disease. Or maybe lower extremity amputations are more accepted in certain areas. There may be different perceptions about what an amputation really is in different regions, or it could be something as simple as patients understanding how to be compliant with care.”

Clinicians and patients
Then there’s the clinician factor.
“If there is one truism, one thing that isn’t variable about care around the United States and around parts of Europe and the world, it’s variability,” David G. Armstrong, DPM, MD, PhD, a professor of surgery and codirector of the Southern Arizona Limb Salvage Alliance (SALSA) at the University of Arizona College of Medicine in Tucson, told LER.
“It appears that individual clinicians can make a difference, for better or for worse. We often find that centers with lower rates have people in place who are more willing to go the route of limb preservation,” Armstrong added. “In other centers with higher rates, there are often people who think that someone with a sore is just going to get another one. ‘We might as well cut the leg off now and get them into a prosthetic and back to living their life.’ The trouble is both of these people are correct, but one is probably more correct than another.”
Variability may be inevitable, but that doesn’t make it a lesser problem. Armstrong compared its impact to those of some of the major disasters of the industrialized world, such as Three Mile Island, Love Canal, and Bhopal.
Dane K. Wukich, MD, chief of the Division of Foot and Ankle Surgery and assistant professor of orthopedic surgery at the University of Pittsburgh School of Medicine, agrees.
“I think it’s an enormous problem because diabetes costs our country an enormous amount of money each year,” Wukich told LER.
He thinks variation in amputation rates largely results from variations in socioeconomics and access to care, not only among regions and states but within local areas.
“Within cities, you can see it as people coming from different neighborhoods,” Wukich said.
He also thinks that education about how serious the problem of variability among amputation rates is needs to be ramped up for both clinicians and patients.
“I think you need a paradigm shift in this area,” he said.
Mark Hinkes, DPM, chief of podiatric medicine at the VA Medical Center in Nashville, TN, and author of the book Healthy Feet for People with Diabetes, agrees that a paradigm change can indeed come from better education.
“There has to be a revolution in learning, not only for patients, but for providers and for administrators. This paradigm can be turned around with appropriate instruction,” Hinkes said.
It’s vascular
Patients should be made more aware of how problems develop, Hinkes said, including risks related to diabetic peripheral neuropathy and peripheral vascular disease.
He thinks physicians should do more preoperative vascular evaluations before amputations.
“If we could identify where a stenosis is in the vascular tree, we have amazing twenty-first century technologies to treat critical limb ischemia,” he said. “Physicians need to stay abreast of the latest technology.”
Wukich also suggested the apparent increase in number of amputation prevention centers might help in educating patients, clinicians, and others involved in healthcare.
“Setting those up so that, once an ulcer develops, people get into a good formal program is the way to go to reduce amputations,” he said.
Armstrong agrees. He said that, within a three-week period early this year, people from the US, China, UK, Australia, and Saudi Arabia were visiting SALSA to learn more about setting up such centers.
“This is becoming a common service within a hospital,” he said. “Usually, the philosophy of a clinic comes from presence or absence of a dedicated team taking care of this.”
Everything’s local
But even a dedicated center with teams of providers considering all options for patients can still have variations in outcomes and costs because of outside influences, Armstrong said.
“All medical care is local, just like politics is local,” he said. “All of these things are informed, positively or negatively, by the population that a person is in and by policies from farther away.”
As an example, he cited SALSA’s own experience since Arizona Medicaid removed podiatric care from reimbursement in 2009. Over a five-year period, SALSA had about a 38% increase in hospital admissions for diabetic foot infections, about a 45% increase in mean charges, and an almost 30% increase in lengths of stay, while severe aggregate outcomes, including amputations and deaths, increased more than 30%. Armstrong and his colleagues presented this information at the American Diabetes Association meeting in Chicago last year.9
This is a case for which policymakers could also use some education.
“Policymakers don’t look bad when amputation rates are high. They look bad when they have to add another $350,000 to the budget, which by the way, in Arizona, that was about the total cost of the direct [podiatric] fund,” Armstrong said, referring to $351,000 out of an $8 billion budget. “That also causes increases in variability.”
Hinkes agrees that more education needs to be directed toward policymakers and payers.
“Medicare will pay for an amputation, but it won’t pay for a preventive foot exam,” he said. “Medicare does pay for a retinal photograph to prevent blindness, a complication of diabetes, but not for many other key prevention measures.”
He said he is working passionately toward providing more education for everyone, based on his experience as chair of amputation prevention programs at two Veterans Affairs hospitals. At a VA hospital in Salem, VA, “in two years we reduced lower extremity amputations by 27% and saved $1.2 million,” he said. Over a five-year period in Nashville, he added, amputations have gone down by 40%, and the hospital has saved $1.8 million.
Hinkes is in the process of developing a web-based survey that either physicians or patients can use to answer 48 questions about topics such as social history and vascular and neurological history. He has created an algorithm to stratify patients into internationally accepted risk categories and has added evidence-based information to that to come up with recommendations about risk factors.
The survey tool was undergoing the patent process in January, Hinkes said.
“It will tell us in advance which patients are likely to develop an ulcer and have an amputation,” he said.
Larry Hand is a writer in Massachusetts.
1. Yin H, Radican L, Kong SX. A study of regional variation in the inpatient cost of lower extremity amputation among patients with diabetes in the United States. J Med Econ 2013;16(6):820-827.
2. Blumberg SN, Warren SM. Disparities in initial presentation and treatment outcomes of diabetic foot ulcers in a public, private, and Veterans Administration hospital. J Diabetes 2014;6(1):68-75.
3. Kerr EA, Gerzoff RB, Krein SL, et al. Diabetes care quality in the Veterans Affairs Health Care System and commercial managed care: The TRIAD study. Ann Intern Med 2004;141(4):272-281.
4. Reiber GE, Koepsell TD, Maynard C, et al. Diabetes in nonveterans, veterans, and veterans receiving Department of Veterans Affairs health care. Diabetes Care 2004;27(Suppl 2):B3-B9.
5. Nelson KM, Chapko MK, Reiber G, Boyko EJ. The association between health insurance coverage and diabetes care; data from the 2000 Behavioral Risk Factor Surveillance System. Health Serv Res 2005;40(2):361-372.
6. Piette JD. Satisfaction with care among patients with diabetes in two public health care systems. Med Care 1999;37(6):538-546.
7. Margolis DJ, Hoffstad O, Nafash J, et al. Location, location, location: Geographic clustering of lower-extremity amputation among Medicare beneficiaries with diabetes. Diabetes Care 2011;34(11):2363-2367.
8. Wrobel JS, Mayfield JA, Reiber, GE. Geographic variation of lower-extremity major amputation in individuals with and without diabetes in the Medicare population. Diabetes Care 2001;24(5):860-864.
9. Skrepnek GH, Mills JL, Armstrong DA. Foot-in-wallet disease: Tripped up by ‘cost saving’ reductions. Presented at the 73rd Scientific Sessions of the American Diabetes Association, Chicago, June 2013.





