
 By Sarah L. Woelfel, MA, LAT, ATC and Adam B. Rosen, PhD, ATC
By Sarah L. Woelfel, MA, LAT, ATC and Adam B. Rosen, PhD, ATC
Point of care diagnostic ultrasound can be a useful tool for the evaluation, diagnosis, treatment, and risk identification of patellar tendinopathy. Measurements of the patellar tendon that may be useful include tendon thickness, stiffness, and biomarkers of tendon quality which can provide clinicians with a more comprehensive assessment of the histological and healing progress of the patellar tendon. However, for sports medicine clinicians, appropriate training to ensure reliability and proficiency is paramount.
Patellar tendinopathy is a highly prevalent condition that affects individuals of all ages, compromising their abilities to comfortably perform activities of daily living, as well as other physical and recreational activities. While patellar tendinopathy can develop in the general population — one study from a Dutch general medical practice found that lower extremity tendinopathies have prevalence and incidence rates of 11.83 and 10.52 per 1000 person-years1 – the condition is common among physically active individuals, particularly those involved in running and jumping sports.1–4 For example, one study showed prevalence of symptoms of patellar tendinopathy was 44.6% and 31.9% for volleyball and basketball athletes, respectively.5 In a recreational running population, patellar tendinopathy was one of the top 3 most common pathological conditions along with patellofemoral pain syndrome and iliotibial band friction syndrome.6
Documented risk factors for patellar tendinopathy include being male, higher body mass index, taller height, younger age, playing surfaces, increased amount of training — including jumping and running, and sports participation.2,5,7 If mismanaged, patellar tendinopathy can lead to activity restrictions, lengthy therapeutic rehabilitation, and even the end of athletic careers.3
An umbrella term for tendon degeneration and inflammation, patellar tendinopathy can lead to daily aggravating pain that requires activity restrictions and long-term rehabilitation and care to treat and manage symptoms.3 Typically patients report pain that is localized to the anterior knee and can be related back to an increase in the frequency and intensity of physical activities that overload the patellar tendon; such overloading leads to micro-tears and the degeneration of tissue.3 Signs or symptoms used in the clinical diagnosis of patellar tendinopathy include
- pain localization at the inferior pole of the patella and inferior toward the tibial tuberosity along the patellar tendon,
- load-related pain that escalates with increased intensity or plyometric exercises that stress the patellar tendon,
- little to no pain when resting,
- decreased pain after warming-up and continuing exercise,
- then increased pain the day after exercise.4

Figure 1: Ultrasound image (ACUSON Redwood Ultrasound System, Siemens Medical Solutions USA, Inc., Issaquah, WA) of the patellar tendon with 2 observable deformities. On the right, there is a bony deformity at the distal end of the patellar tendon at the tibial tuberosity. On the left, there is a darkened spot on the patellar tendon at the inferior pole of the patella, indicating inflammation with potential disruption to the patellar tendon.
Diagnosis of patellar tendinopathy is typically clinical, but imaging is common for confirmation and to eliminate potential differential diagnoses and assess tendon integrity.4
Common imaging for the patellar tendon is magnetic resonance imaging (MRI) or diagnostic ultrasound (DU) to assess the integrity of the tendon and surrounding structures of the knee.3 Currently, the accuracy for MRI in diagnosing patellar tendinopathy is approximately 70%, while the accuracy for correctly identifying patellar tendinopathy with DU is about 83%.8 Compared to MRI, ultrasound also can provide significant real-time advantages to the practicing clinician.
Diagnostic Ultrasound
Point-of-care DU has become increasingly popular due to its wide availability, cost, safety, speed, and accessibility of the procedure. With continued growth over the last few decades, DU at the point of care has the ability to evaluate tendons for elasticity, tissue stiffness and quality, and tendon health.9 Typically, studies comparing individuals with patellar tendinopathy with healthy individuals have found differences in ultrasonographic measures, depending on the method used and the location of interest. Different ultrasonographic methods (eg, compression elastography, shear-wave elastography, spatial frequency analysis, etc.) can be utilized to evaluate a variety of tendon properties including anthropometrics, tendon integrity, tissue quality, and stiffness of the patellar tendon. Diagnostic ultrasound can be useful in sports medicine settings for early diagnosis of patellar tendinopathy or tendon abnormalities and has the potential to be used during tendon evaluations as an objective outcome for evaluating the effectiveness of treatment and rehabilitation protocols for patellar tendinopathy.
Tendon Anthropometrics
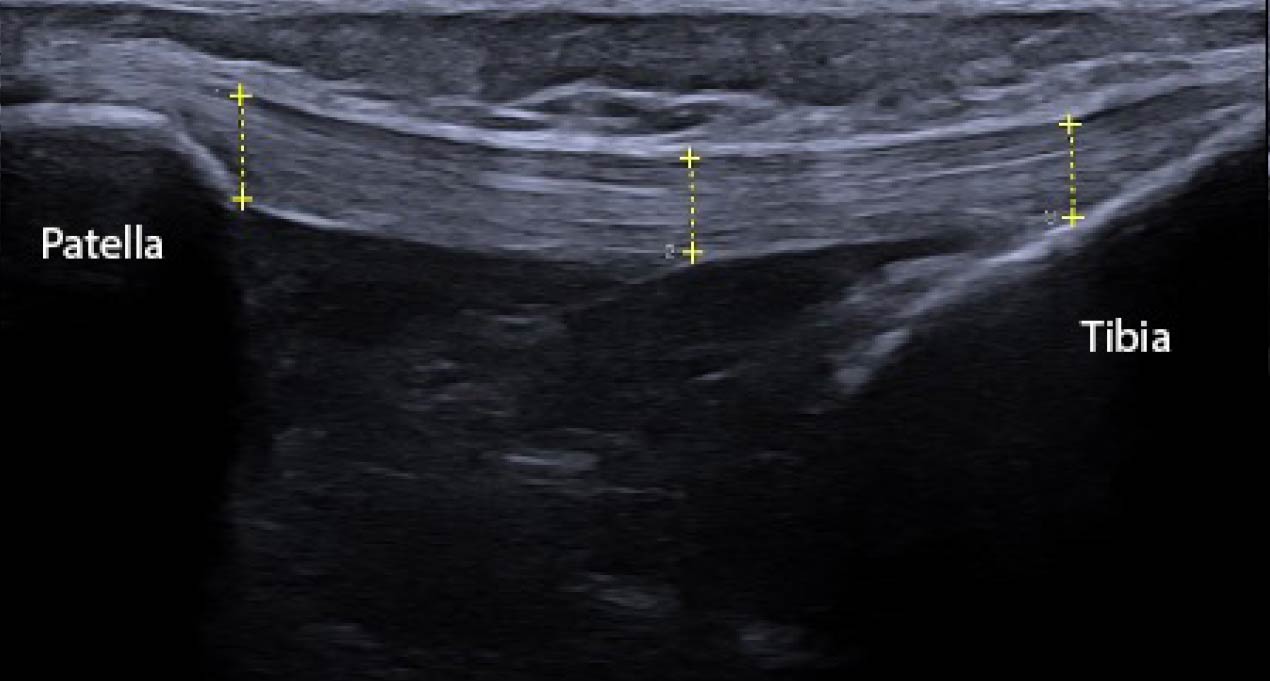
Figure 2: Ultrasound image (ACUSON Redwood Ultrasound System, Siemens Medical Solutions USA, Inc., Issaquah, WA) of the length of the patellar tendon. There are 3 locations where clinicians may choose to measure the thickness of the patellar tendon (proximal, middle, distal). Thickening of the tendon is a common pathological sequalae of patellar tendinopathy, particularly at the inferior pole of the patella.
Basic measurements that can be obtained with DU include tendon length, width, and thickness. Tendon length and width primarily provide more information regarding the basic structure of the patellar tendon, with the potential of observing obvious tendon abnormalities (Figure 1). Some abnormalities may include increased or decreased tendon length due to limb length or subject height.10 Other deformities that may be observed when measuring tendon length and width are obvious tears or partial tears in the tendon, but those abnormalities may require further evaluation via MRI.
Tendon thickness, meanwhile, may provide more information regarding the condition of the tendon that is clinically relevant. Pathological tendons present with tissue disorganization, which manifests upon evaluation and imaging as a thicker tendon compared to healthy tendons.11 In addition, scanning the entire length of the patellar tendon may yield differences along the continuum of the patellar tendon, for example at the origin at the inferior pole of the patella or the insertion at the tibial tuberosity (Figure 2). One study that evaluated patellar tendons in athletes found that the proximal patellar tendon was significantly thicker in those with patellar tendinopathy.12 While another study evaluated patellar tendons in beach volleyball players and noted that individuals with no tendinosis had an average patellar tendon thickness of 4.7/4.8 mm (dominant vs non-dominant knee) while symptomatic athletes demonstrated an average thickness of 7.6/7.0 mm( P <0.001 for dominant knee; P = 0.001 for non-dominant knee).13 Therefore thickness may be an important metric for clinicians to capture.
Ultrasound Elastography
Ultrasound elastography (USE), first introduced in the 1990’s by Ophir et al,14 has the ability to characterize tendon tissue and their response to stress.15 Elastography measures the elastic modulus to quantify tendon elasticity. Compared to other imaging options, this measure provides a wide variation of parameters that allows for greater discrimination between tissues and pathologies.15 Young’s elastic modulus, a common metric used to reflect the elastic properties of the tendon, can be estimated by calculating the slope of the elastic portion of the stress-strain curve.15 There are a few different categories of elastography, including compression elastography (CE) and sheer-wave elastography (SWE).
Compression Elastography

Figure 3: B-mode image of the patellar tendon (left) and an elastogram of the same region of interest (right). On the elastogram, areas of increased stiffness are indicted by dark red. Specific regions of interest can be assessed and quantified, demonstrated by the three diameter circles, which can provide different shear velocities for each region.
Compression elastography (CE) is characterized by the application of repeated manual compression on tissues by utilizing a hand-held US transducer to reproduce tissue displacements, or strain on the tendon, to exhibit relative elasticity.15 Using rhythmic and regular compressions of the area, the evaluator is able to target a specific area of interest to observe qualitative strain on the tissue. These strains are collected, and a specialized software is used to display a color-coded elastogram, typically displayed next to the conventional ultrasound image on the screen. In the color-coded elastogram, red frequently indicates soft (high-strain), blue indicates hard (low-strain), green and yellow indicate intermediate stiffness (medium-strain).16 More deformation is observable in softer tissues, which then experience larger strain than stiffer tissues which experience lesser strain.15 Successful and accurate measurements with CE depend on the depth of the targeted tissues and probe position, which make this technique more difficult to execute and operator-dependent.17 If the stress distribution within the tissue is not uniform or standardized during CE, this can affect the Young’s elastic modulus measurement that describes the elasticity of the tissue.15
Compression elastography has been proven to differentiate between normal and pathologic tissues. In a study comparing CE evaluation of symptomatic and asymptomatic patellar tendons in 75 athletes (average age 33 yrs), symptomatic tendons (n = 38) showed higher strain scores compared to asymptomatic patellar tendons.18 In addition, neovascularization was detected in 58% of the symptomatic tendons. Another study utilizing CE to investigate patellar tendons (N = 70 patellar tendons) in 35 volleyball athletes found that symptomatic patellar tendons were softer compared to asymptomatic.19
And according to Porta et al, CE showed good values for intra-observer and inter-observer agreement in patients with patellar tendinopathy and had an easy training curve.20
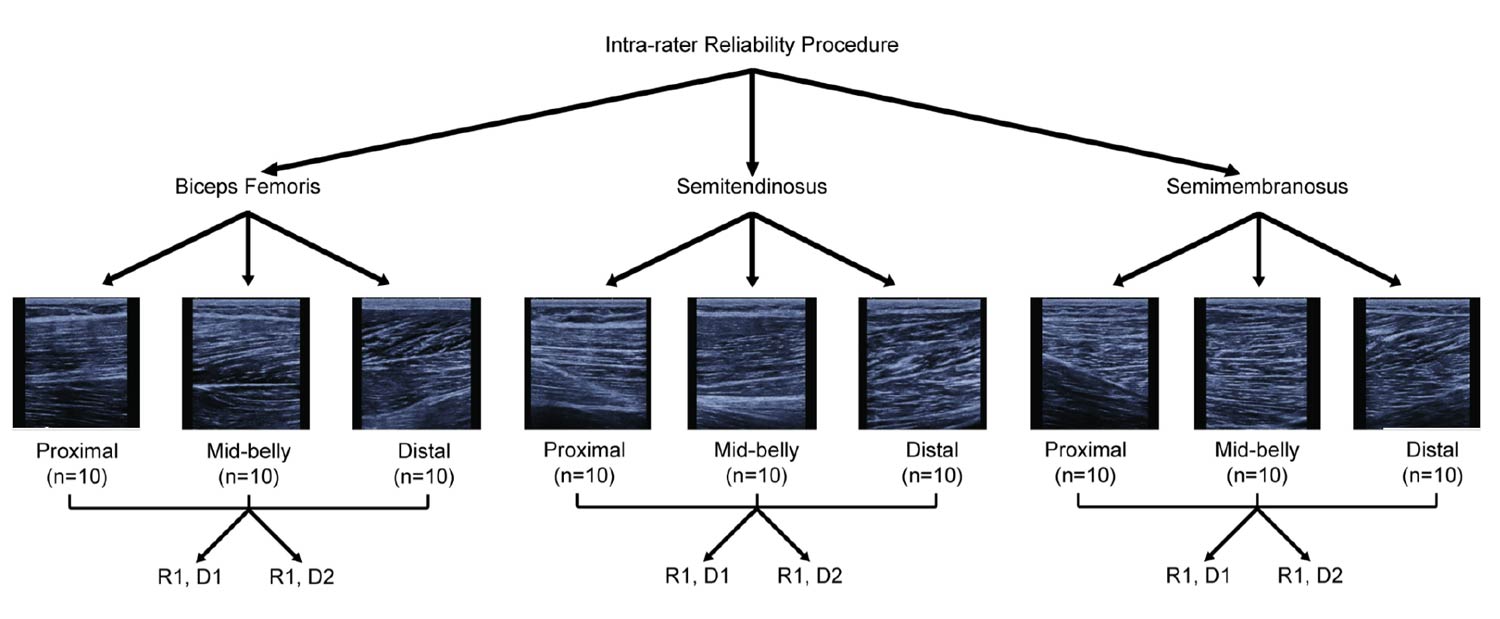
Figure 4: This SFA parameter extraction of the biceps femoris from Crawford et al31 is an example of the spatial distribution of the acoustic scatters within select regions of interest. These authors noted that such analyses may provide objective determination of tissue organization as a result of injury and subsequent rehabilitation.
Shear-wave Elastography

Shear-wave elastography (SWE) can also be utilized to characterize absolute tissue elasticity of soft tissues. SWE involves a perpendicular stress applied to the tissue which produces shear-waves. These waves are then measured with radiofrequency images to create a colored tissue displacement map that is used to calculate shear-wave velocity and shear modulus.17 Thus, we are allowed to assess the elastogram to evaluate the tendon tissue for elasticity in a more objective way compared to CE since there is no repeated manual compression utilized in this technique. The displacement will display different colors as noted above: red typically defines hard tissue consistency, blue as soft consistency, and green and yellow as in-between. Modifications on tissue elasticity can potentially be detected earlier than observable deformities with conventional ultrasound images most often termed B-mode images in the literature (Figure 3).15 Studies that investigated SWE demonstrated increased stiffness in symptomatic tendons and increased stiffness in the proximal and mid-patellar region.21,22
Specifically for patellar tendinopathy, patients tend to have increased stiffness and have a significant correlation between the increased stiffness and intensity of pain and dysfunction.23 This same study also demonstrated that symptomatic patellar tendons displayed higher shear modulus and were larger and stiffer in patients with proximal patellar tendinopathy.23,24 It has also been suggested that SWE can aid in the prediction of impeding tendon failure, thus helping clinicians make informed clinical decisions in implementing preventative rehabilitation protocols.17 Hsiao et al discovered decreased elasticity (decreased elastic modulus) in the patellar tendon in an older age group (aged 60-70 years) compared to 2 younger age groups (20-30 and 50-60 years), thus suggesting the ability to detect aging tendons before visible abnormalities are observed using other imaging methods.25
According to several studies, SWE has been shown to produce excellent intra-observer and inter-day reliability and moderate to excellent inter-observer reliability.23,26,27 Consequently, SWE has been considered more objective, quantitative, and reproducible when compared to CE, since CE requires a certain level of replicability of manual compression with measurements.15,17 Some limitations of SWE involve sensitivity to angle, pressure, and orientation of the probe along with shallow depths of penetration or region of interests, depending on the specific transducer or ultrasound machine.
Spatial Frequency Analysis
 Spatial frequency analysis (SFA) is a specific ultrasound method that can characterize musculoskeletal tissue organization from ultrasound images and distinguish between pathological and healthy tendon tissue.28–31 SFA is relatively new and can potentially be used for the diagnosis of patellar tendon injury or as a helpful measure for tracking tendon tissue adaptation during the rehabilitation process post-injury.28–31 Analyzing B-mode images of the patellar tendon will display a speckle pattern in which the brightness of the image depends on the spatial distribution of the acoustic scatters within the tendon.32 The structure and alignment of the tendon tissues determines the characteristic pattern and intensity.32,33 One study suggests that disruptions to the speckle pattern occurs with tendon damage and can be observed in patients with tendinopathy and was successful in classifying tendon tissues.33 Typically higher SFA translates to a well-structured speckle pattern with bands containing mostly parallel fibrils while lower SFA has a less clear banded pattern and more disorganization.34
Spatial frequency analysis (SFA) is a specific ultrasound method that can characterize musculoskeletal tissue organization from ultrasound images and distinguish between pathological and healthy tendon tissue.28–31 SFA is relatively new and can potentially be used for the diagnosis of patellar tendon injury or as a helpful measure for tracking tendon tissue adaptation during the rehabilitation process post-injury.28–31 Analyzing B-mode images of the patellar tendon will display a speckle pattern in which the brightness of the image depends on the spatial distribution of the acoustic scatters within the tendon.32 The structure and alignment of the tendon tissues determines the characteristic pattern and intensity.32,33 One study suggests that disruptions to the speckle pattern occurs with tendon damage and can be observed in patients with tendinopathy and was successful in classifying tendon tissues.33 Typically higher SFA translates to a well-structured speckle pattern with bands containing mostly parallel fibrils while lower SFA has a less clear banded pattern and more disorganization.34
In a case report published by Crawford et al in 2021, a patient had a bilateral debridement of the patellar tendon, and the head researcher evaluated the patellar tendon regularly utilizing SFA ultrasound methods.28 In this case, they measured the Peak Spatial Frequency Radius (PSFR) of the patellar tendon at four different knee joint angles over the course of the 12-month rehabilitation period and assessed pain and dysfunction via the Victorian Institute of Sport-P (VISA-P). Over the course of the study, they observed an increase in PSFR throughout the rehabilitation protocol, indicating an increase in collagen organization. In another study, Kulig et al analyzed patellar tendon tissue for spatial frequency parameters in volleyball players and determined that symptomatic athletes demonstrated greater collagen disorganization compared to non-athlete controls and asymptomatic volleyball athletes.35 These authors suggested that painful symptoms are associated with degeneration rather than inflammation only and that assessing patellar tendons with DU can help track changes in tendon structure to determine the proper course of treatment and rehabilitation.
Clinical Implications
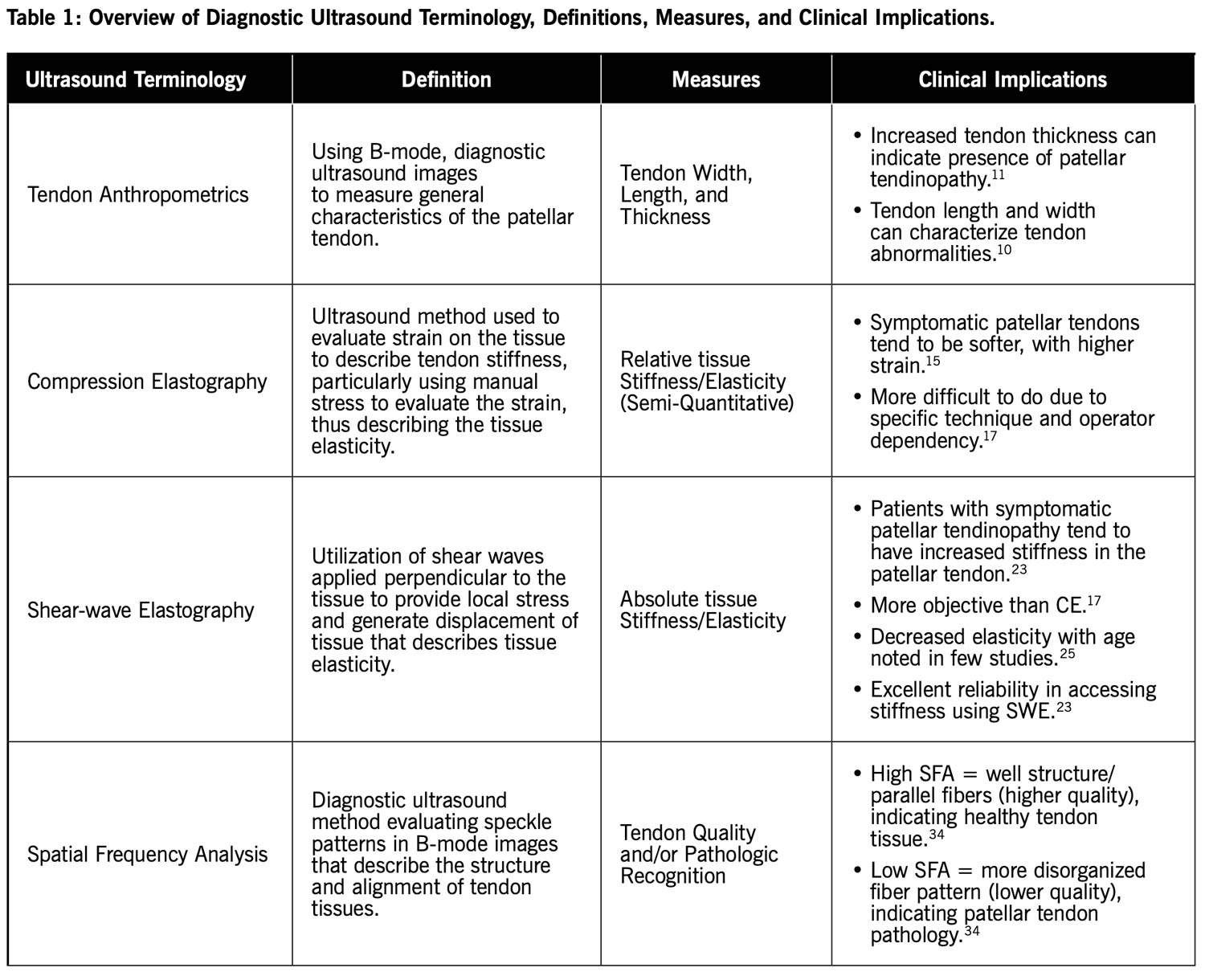
Diagnostic ultrasound is cost-effective, non-invasive, reliable, and efficient as an imaging tool that can assist clinicians with the evaluation and diagnosing of conditions like patellar tendinopathy at the point of care. Utilizing DU can provide information related to the intrinsic characteristics of the patellar tendon that can more accurately describe the current state of an abnormal patellar tendon (Table 1). These can be leveraged to provide guidance to clinicians in terms of understanding the pathology, creating treatment and rehabilitation protocols for altered tendon morphology, and informing clinical decision making.
Point of care DU use in the orthopedic and sports medicine field is rapidly developing. There are clear benefits to implementing this imaging tool to inform practice and improve patient care. But the use of DU is limited depending on settings, accessibility, and user proficiency. Clinicians seeking to implement ultrasound into their daily routine require proper training in the physical utilization of this technology and the ability to interpret images to maximize the benefits of DU at the point of care.
Sarah L. Woelfel MA, LAT, ATC, is a first year, PhD student studying Biomechanics and Kinesiology at the University of Nebraska at Omaha.
Adam B. Rosen PhD, ATC, is an Associate Professor in the School of Health and Kinesiology, Director of the Athletic Training Program at the University of Nebraska at Omaha and co-director of the UNO Sports Medicine and Biomechanics Laboratory.
- Albers IS, Zwerver J, Diercks RL, et al. Incidence and prevalence of lower extremity tendinopathy in a Dutch general practice population: a cross sectional study. BMC Musculoskelet Disord. 2016;17(1):16.
- Theodorou A, Komnos G, Hantes M. Patellar tendinopathy: an overview of prevalence, risk factors, screening, diagnosis, treatment and prevention. Arch Orthop Trauma Surg. 2023;143(11):6695-6705.
- Rosen AB, Wellsandt E, Nicola M, Tao MA. Clinical management of patellar tendinopathy. J Athl Train. 2022;57(7):621-631.
- Malliaras P, Cook J, Purdam C, Rio E. Patellar tendinopathy: clinical diagnosis, load management, and advice for challenging case presentations. J Orthop Sports Phys Ther. 2015;45(11):887-898.
- Lian ØB, Engebretsen L, Bahr R. Prevalence of jumper’s knee among elite athletes from different sports: a cross-sectional study. Am J Sports Med. 2005;33(4):561-567.
- Benca E, Listabarth S, Flock FKJ, et al. Analysis of running-related injuries: the Vienna study. J Clin Med. 2020;9(2):438.
- Zwerver J, Bredeweg SW, Van Den Akker-Scheek I. Prevalence of jumper’s knee among nonelite athletes from different sports: a cross-sectional survey. Am J Sports Med. 2011;39(9):1984-1988.
- Warden SJ, Kiss ZS, Malara FA, et al. Comparative accuracy of magnetic resonance imaging and ultrasonography in confirming clinically diagnosed patellar tendinopathy. Am J Sports Med. 2007;35(3):427-436.
- Sigrist RMS, Liau J, Kaffas AE, et al. Ultrasound elastography: review of techniques and clinical applications. Theranostics. 2017;7(5):1303-1329.
- Hohenberger GM, Dreu M, Kreuzthaler H, et al. Patellar tendon length is associated with lower extremity length but not gender. Inidan J Orthop. 2020;54(3):352-357.
- Skou ST, Aalkjaer JM. Ultrasonographic measurement of patellar tendon thickness—a study of intra- and interobserver reliability. Clin Imaging. 2013;37(5):934-937.
- Nishida Y, Nishino T, Tanaka K, et al. An objective measure of patellar tendon thickness based on ultrasonography and MRI in university athletes. J Clin Med. 2021;10(18):4092.
- Pfirrmann CWA, Jost B, Pirkl C, et al. Quadriceps tendinosis and patellar tendinosis in professional beach volleyball players: sonographic findings in correlation with clinical symptoms. Eur Radiol. 2008;18(8):1703-1709.
- Ophir J, Céspedes I, Ponnekanti H, et al. Elastography: a quantitative method for imaging the elasticity of biological tissues. Ultrason Imaging. 1991;13(2):111-134.
- Prado-Costa R, Rebelo J, Monteiro-Barroso J, Preto AS. Ultrasound elastography: compression elastography and shear-wave elastography in the assessment of tendon injury. Insights Imaging. 2018;9(5):791-814.
- Drakonaki EE, Allen GM, Wilson DJ. Ultrasound elastography for musculoskeletal applications. Br J Radiol. 2012;85(1019):1435-1445.
- Taljanovic MS, Gimber LH, Becker GW, et al. Shear-wave elastography: basic physics and musculoskeletal applications. Radiographics. 2017;37(3):855-870.
- Rist HJ, Mauch M. Quantifizierte TDI-Elastosonografie der Patellarsehne bei Sportlern [Quantified TDI elastography of the patellar tendon in athletes]. Sportverletz Sportschaden. 2012;26(01):27-32.
- Ooi CC, Richards PJ, Maffulli N, et al. A soft patellar tendon on ultrasound elastography is associated with pain and functional deficit in volleyball players. J Sci Med Sport. 2016;19(5):373-378.
- Porta F, Damjanov N, Galluccio F, et al. Ultrasound elastography is a reproducible and feasible tool for the evaluation of the patellar tendon in healthy subjects. Int J of Rheum Dis. 2014;17(7):762-766.
- Coombes BK, Tucker K, Vicenzino B, et al. Achilles and patellar tendinopathy display opposite changes in elastic properties: a shear wave elastography study. Scand Med Sci Sports. 2018;28(3):1201-1208.
- Dirrichs T, Quack V, Gatz M, et al. Shear wave elastography (SWE) for the evaluation of patients with tendinopathies. Acad Radiol. 2016;23(10):1204-1213.
- Zhang ZJ, Ng GY fat, Lee WC, Fu SN. Changes in morphological and elastic properties of patellar tendon in athletes with unilateral patellar tendinopathy and their relationships with pain and functional disability. PLoS ONE. 2014;9(10):e108337.
- Breda SJ, Van Der Vlist A, De Vos RJ, et al. The association between patellar tendon stiffness measured with shear-wave elastography and patellar tendinopathy—a case-control study. Eur Radiol. 2020;30(11):5942-5951.
- Hsiao MY, Chen YC, Lin CY, et al. Reduced patellar tendon elasticity with aging: in vivo assessment by shear wave elastography. Ultrasound Med Biol. 2015;41(11):2899-2905.
- Taş S, Onur MR, Yılmaz S, et al. Shear wave elastography is a reliable and repeatable method for measuring the elastic modulus of the rectus femoris muscle and patellar tendon. J of Ultrasound Med. 2017;36(3):565-570.
- Peltz CD, Haladik JA, Divine G, et al. Shearwave elastography: repeatability for measurement of tendon stiffness. Skeletal Radiol. 2013;42(8):1151-1156.
- Crawford SK, Rudolph A, Engel AJ, et al. Longitudinal quantitative ultrasonic analysis of patellar tendon in a collegiate athlete after bilateral debridement: a case report. J Athl Train. 2021;56(12):1349-1354.
- Crawford SK, Wille CM, Stiffler-Joachim MR, et al. Spatial frequency analysis detects altered tissue organization following hamstring strain injury at time of injury but not return to sport. BMC Med Imaging. 2021;21(1):190.
- Crawford SK, Kliethermes SA, Heiderscheit BC, Bashford GR. Influence of ultrasound machine settings on quantitative measures derived from spatial frequency analysis of muscle tissue. BMC Musculoskelet Disord. 2023;24(1):664.
- Crawford SK, Lee KS, Bashford GR, Heiderscheit BC. Intra-session and inter-rater reliability of spatial frequency analysis methods in skeletal muscle. PLoS ONE. 2020;15(7):e0235924.
- Pearson SJ, Engel AJ, Bashford GR. Changes in tendon spatial frequency parameters with loading. J Biomech. 2017;57:136-140.
- Bashford GR, Tomsen N, Arya S, et al. Tendinopathy discrimination by use of spatial frequency parameters in ultrasound B-Mode images. IEEE Trans Med Imaging. 2008;27(5):608-615.
- Kulig K, Chang YJ, Winiarski S, Bashford GR. Ultrasound-based tendon micromorphology predicts mechanical characteristics of degenerated tendons. Ultrasound Med Biol. 2016;42(3):664-673.
- Kulig K, Landel R, Chang Y -J., et al. Patellar tendon morphology in volleyball athletes with and without patellar tendinopathy. Scand Med Sci Sports. 2013;23(2).





