 Using muscle function symmetry as an indicator of patient progress after anterior cruciate ligament (ACL) reconstruction can provide insight about potential targets for intervention to improve movement quality, functional performance, and patient outcomes.
Using muscle function symmetry as an indicator of patient progress after anterior cruciate ligament (ACL) reconstruction can provide insight about potential targets for intervention to improve movement quality, functional performance, and patient outcomes.
By Christopher Kuenze, PhD, ATC; and Adam Kelly, MS, ATC
The goal of anterior cruciate ligament reconstruction (ACLR) is to improve knee joint stability following ACL injury to facilitate a return to preinjury levels of physical activity or sports performance.1 Unfortunately, this clinical approach often comes with potential costs in the form of persistent neuromuscular and movement dysfunction that can be difficult to evaluate and treat in the clinical setting.2 Although comprehensive rehabilitation following surgery is meant to address these potential issues, it’s often difficult for clinicians to effectively monitor patient progress because they lack information about the patient’s preinjury functional status and level of performance. This can pose a significant challenge in setting clinical goals for the patient, as well as for making informed decisions regarding rehabilitation progression for a safe return to physical activity or sports.
In the absence of preinjury physical assessment data clinicians often use the uninjured or contralateral limb as a stable reference for comparison.3 In the literature, limb symmetry assessments have been reported for measures of muscle function, biomechanics, and functional performance following ACLR.4 The ideal approach to prospective assessment of physical function following ACLR would include comparison with preinjury data or normative data for a matched population, but this is largely unrealistic for most measurements or assessments used in the clinical setting. The use of limb symmetry as an indicator of patient progress has been supported in the literature and, despite some limitations, has provided insight into potential targets for intervention that can positively impact movement quality, functional performance, and patient outcomes.
Quantification of limb symmetry
There are several common approaches to assessing limb symmetry, all of which have strengths and weaknesses that depend on the goal of the assessor. Subtracting a measurement of the injured limb from the corresponding measurement of the healthy contralateral limb is a simple and commonly used estimation of asymmetry or between-limb differences. Despite its ease of use, it does not adequately account for the scale of the measure being taken.
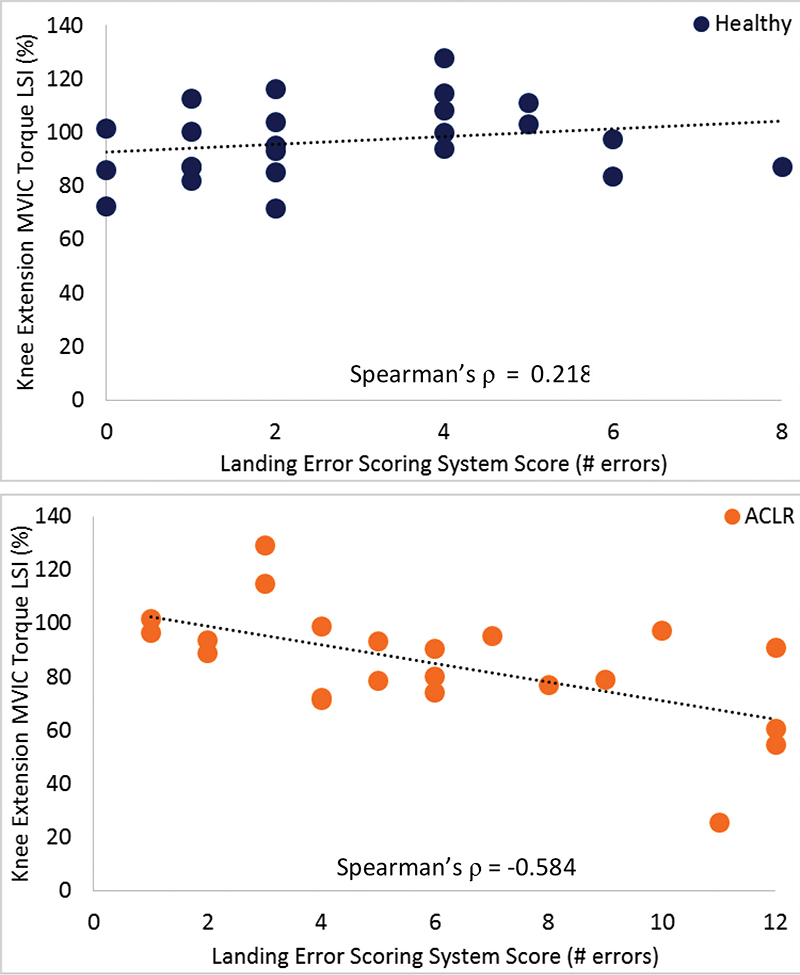
Figure 1. The relationship between knee extension MVIC torque symmetry and Landing Error Scoring System score. There is a significant moderate relationship (ρ= -.584) between less knee extension MVIC torque asymmetry and more landing errors among those with a history of ACLR, while no relationship exists among healthy participants.
The use of limb symmetry indices (LSI, Equation 1) has become commonplace in practitioner attempts to better understand the magnitude of symmetry between limbs relative to the scale of the assessment of interest.3,5,6 In this case, the between-limb difference is now represented as a percentage of the healthy limb measurement, which enables the clinician to compare symmetry directly between different assessments regardless of the scale of the units of measure. For example, a clinician would be able to directly compare symmetry estimates for range of motion and strength for an individual, since LSI in each case would be expressed as a percentage, despite the fact that one is measured in degrees while the other is measured in newtons or foot-pounds.
![]()
Our corticomotor research
Unilateral and bilateral deficits in quadriceps strength and activation have been widely reported in the months and years following ACLR.7,8 The exact source of this dysfunction has been elusive, but neural inhibition at the cortical and spinal levels and muscle atrophy have been implicated as primary contributors.2,8,9 Previous research investigating the importance of symmetry in quadriceps strength and activation following ACLR has established a number of thresholds for adequate or ideal quadriceps functional symmetry. Most often studies report that 85%4 or 90% symmetry10,11 is indicative of good bilateral quadriceps function and functional performance. These scores are predictive of strong patient-reported knee-related function, as well as symmetry in performance on functional testing such as single-leg hopping.12-14 Unfortunately, the source of asymmetry and the potential targets for clinical intervention in patients with persistent quadriceps dysfunction is still unclear.
Our recent work has focused on the symmetry of neuromuscular and corticomotor measures of quadriceps function among patients with a history of unilateral ACLR, as well as healthy controls.8 The primary goals of this research were to confirm that neuromuscular and corticomotor symmetry in quadriceps function is present in healthy individuals and to quantify the level of asymmetry in clinical and laboratory-based measures of quadriceps function among physically active patients with a history of ACLR.
To better understand the potential sources of symmetry in isometric knee extension strength following ACLR, we chose to investigate symmetry in cortical excitability via transcranial magnetic stimulation (TMS), spinal reflex excitability via the quadriceps Hoffmann reflex (H-reflex), and a global measure of quadriceps activation via the quadriceps central activation ratio (CAR). We found that patients with a history of ACLR (time since surgery = 31.5 ± 23.5 months) who had returned to physical activity persistently experienced greater asymmetry in quadriceps strength, quadriceps activation, and cortical excitability, but not in spinal reflex excitability, compared with a similar group of healthy participants.
Our findings related to quadriceps strength and activation were consistent with those of previous investigations;7,11 however, this was the first time that asymmetry of quadriceps function was linked to cortical sources of asymmetry in those with a history of ACLR. While not included in the published study, subsequent reanalysis of this dataset revealed a moderate relationship between symmetry of cortical excitability and symmetry of both quadriceps strength (ρ = .417) and activation (ρ = .564). Although not causal, this relationship may highlight the importance of cortically directed treatment options, such as visual or auditory feedback during strength and movement training, when attempting to restore functional symmetry during the terminal phases of rehabilitation after ACLR.
Functional implications of symmetry
Return to optimal and symmetrical muscle function is a common clinical goal that is important for restoration of lower extremity movement quality, functional performance, and improvement in patient outcomes, as well as for reduction of reinjury risk after ACLR.11,15-18 Our current work focuses on the relationship between asymmetry in muscle function and movement quality and between asymmetry in muscle function and patient-reported function after return to physical activity in patients with a history of unilateral ACLR. This approach lets us investigate the source of potential dysfunction while better understanding its clinical manifestations to provide clinicians with guidance regarding the most effective evaluative and treatment techniques for patients experiencing asymmetry in quadriceps function following ACLR.
Symmetry and movement quality
Recently, we assessed the relationship between Landing Error Scoring System (LESS) score,19 a validated assessment tool for identifying patients at high risk for ACL injury, and symmetry of quadriceps function in individuals with a history of ACLR.16 Although our publication focused on the relationship between bilateral knee extension MVIC (maximum voluntary isometric contraction) torque and LESS score, a subsequent reanalysis that focused on symmetry of knee extension MVIC torque revealed some findings that of interest to clinicians.
In those with a history of ACLR, we found a moderate and negative relationship (ρ = -.584) between knee extension MVIC torque and LESS score, indicating that those with better symmetry in quadriceps function also displayed fewer landing errors, which in turn suggests a lower risk of ACL injury (Figure 1). In addition, symmetry of quadriceps strength predicted 30.4% of the variance in LESS score, which establishes a relatively strong causal relationship between these variables. A number of other variables (eg, proprioception, dynamic balance, and fear of movement) undoubtedly contribute to landing errors or, more importantly, risk of ACL injury, but reestablishing symmetry in knee extension strength may be an important first step in improving patient’s movement profiles.
Our findings are consistent with several other studies that have established a link between symmetry in quadriceps function and functional performance, which most commonly has been assessed using single-leg hopping distance.12-14,20 Over the course of several studies, it has been shown that symmetry in knee extension strength is a significant predictor of functional performance and advantageous knee biomechanics during a hopping task.14,20 In addition, improvement in quadriceps function symmetry over the course of recuperation from ACLR is associated with improvement in hop performance.3,21 Although this is a rapidly expanding area of research, these findings are consistent with the approach of many clinicians, specifically the focus on improving a patient’s lower extremity strength before attempting to retrain movement patterns during rehabilitation after ACLR.
Symmetry and patient-reported outcomes
The importance of reestablishing quadriceps function and movement quality following ACLR is clear; however, patient-reported improvement in activities of daily living, knee-related function, and physical activity are more patient-centric outcome measures. In a recent study investigating whether symmetry of knee extension MVIC torque or quadriceps central activation ratio could predict patient-reported knee-related function, we found that near-full symmetry for either measure of quadriceps function was an adequate indicator of patient-reported knee-related function in those with a history of ACLR.15 These findings were consistent with a limited number of previous studies that have investigated this topic in individuals with a history of ACLR.3,21,22 Continued research on the impact of quadriceps function symmetry and lower extremity movement patterns on patient-reported function, as well as physical activity level, represents a natural next step in this field that has the potential to greatly impact the current approach to rehabilitation after ACLR.
Limitations of symmetry as a tool
As with other clinical tools for physical assessment, there are limitations to the use of neuromuscular, biomechanical, or functional symmetry as standalone measures of lower extremity function following ACLR. The major assumption when using complete or near-complete symmetry as an indicator of optimal lower extremity function or patient readiness for a return to physical activity following ACLR is that the contralateral limb or healthy limb is indicative of ideal muscle function, movement quality, or functional performance.
Although it is possible that the contralateral limb is the model of optimal comprehensive lower extremity function, ACLR has been shown to be associated with reduced contralateral quadriceps strength and activation7,8,23 as well as altered knee biomechanics during landing in the contralateral limb, despite no injury to the joint or surrounding muscle tissue.11 This “crossover” effect has been shown in a number of clinical populations with a unilateral injury or disease process.24-26
In addition, up to 15% of patients with an ACL injury may have experienced an ACL injury or injury to another structure within the contralateral limb that required surgical intervention.27 This may not immediately invalidate a measure of symmetry; however, additional consideration and concern should be taken when attempting to make comparisons between limbs. In this subgroup, it may be more valuable to focus on maintaining symmetry while facilitating bilateral functional improvements instead of focusing exclusively on reestablishing between-limb symmetry.

Clinical take-home messages
Quantification and prospective tracking of symmetry and asymmetry of quadriceps muscle function following ACLR can provide clinicians and patients with important information regarding the effectiveness of treatment throughout rehabilitation. Using limb symmetry indices may enable clinicians to better quantify and compare persistent alterations in muscle function, movement patterns, and functional performance following ACLR. In addition, recent evidence supports a relationship between neuromuscular symmetry and both biomechanical and functional symmetry, which may help guide clinicians toward targets for early clinical intervention during the rehabilitation process.
The link between symmetry in quadriceps muscle function and movement quality, as well as the link between quadriceps muscle function symmetry and patient-reported function, have been established throughout the literature and should be considered when designing and implementing rehabilitation protocols and return-to-play guidelines. Despite the consistency of these findings, it’s important to account for limitations associated with assessments of asymmetry, including the impact of ACLR on the uninvolved limb, when integrating these estimates into the clinical decision-making process.
Christopher Kuenze, PhD, ATC, is assistant professor in the Department of Kinesiology at Michigan State University in East Lansing, and the director of its Sports Injury Research Laboratory. Adam Kelly, MS, ATC, is a doctoral student in the Department of Kinesiology at Michigan State University and a research assistant in the Sports Injury Research Laboratory.
- Ardern CL, Webster KE, Taylor NF, Feller JA. Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and meta-analysis of the state of play. Br J Sports Med 2011;45(7):596-606.
- Ingersoll CD, Grindstaff TL, Pietrosimone BG, Hart JM. Neuromuscular consequences of anterior cruciate ligament injury. Clin Sports Med 2008;27(3):383-404.
- Logerstedt D, Grindem H, Lynch A, et al. Single-legged hop tests as predictors of self-reported knee function after anterior cruciate ligament reconstruction: the Delaware-Oslo ACL cohort study. Am J Sports Med 2012;40(10):2348-2356.
- Noyes FR, Barber SD, Mangine RE. Abnormal lower limb symmetry determined by function hop tests after anterior cruciate ligament rupture. Am J Sports Med 1991;19(5):513-518.
- Shelbourne KD, Klotz C. What I have learned about the ACL: utilizing a progressive rehabilitation scheme to achieve total knee symmetry after anterior cruciate ligament reconstruction. J Orthop Sci 2006;11(3):318-325.
- Logerstedt D, Lynch A, Axe MJ, Snyder-Mackler L. Symmetry restoration and functional recovery before and after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 2013;21(4):859-868.
- Hart JM, Pietrosimone B, Hertel J, Ingersoll CD. Quadriceps activation following knee injuries: a systematic review. J Athl Train 2010;45(1):87-97.
- Kuenze CM, Hertel J, Weltman A, et al. Persistent neuromuscular and corticomotor quadriceps asymmetry after anterior cruciate ligament reconstruction. J Athl Train 2015;50(3):303-312.
- Snyder-Mackler L, De Luca PF, Williams PR, et al. Reflex inhibition of the quadriceps femoris muscle after injury or reconstruction of the anterior cruciate ligament. J Bone Joint Surg Am 1994;76(4):555-560.
- Reid A, Birmingham TB, Stratford PW, et al. Hop testing provides a reliable and valid outcome measure during rehabilitation after anterior cruciate ligament reconstruction. Phys Ther 2007;87(3):337-349.
- Schmitt LC, Paterno MV, Ford KR, et al. Strength asymmetry and landing mechanics at return to sport after ACL reconstruction. Med Sci Sports Exerc 2015;47(7):1426-1434.
- Petschnig R, Baron R, Albrecht M. The relationship between isokinetic quadriceps strength test and hop tests for distance and one-legged vertical jump test following anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther 1998;28(1):23-31.
- Rudolph KS, Axe MJ, Snyder-Mackler L. Dynamic stability after ACL injury: who can hop? Knee Surg Sports Traumatol Arthrosc 2000;8(5):262-269.
- Augustsson J, Thomee R, Karlsson J. Ability of a new hop test to determine functional deficits after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 2004;12(5):350-356.
- Kuenze C, Hertel J, Saliba S, et al. Clinical thresholds for quadriceps assessment after anterior cruciate ligament reconstruction. J Sport Rehabil 2015;24(1):36-46.
- Kuenze C, Foot N, Saliba S, Hart J. Drop landing performance and knee extension strength after anterior cruciate ligament reconstruction. J Athl Train 2015;50(6):596-602.
- Jang SH, Kim JG, Ha JK, et al. Functional performance tests as indicators of returning to sports after anterior cruciate ligament reconstruction. Knee 2014;21(1):95-101
- Thomee R, Kaplan Y, Kvist J, et al. Muscle strength and hop performance criteria prior to return to sports after ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 2011;19(11):1798-1805.
- Padua DA, Marshall SW, Boling MC, et al. The Landing Error Scoring System (LESS) is a valid and reliable clinical assessment tool of jump-landing biomechanics: The JUMP-ACL study. Am J Sports Med 2009;37(10):1996-2002.
- Gustavsson A, Neeter C, Thomee P, et al. A test battery for evaluating hop performance in patients with an ACL injury and patients who have undergone ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 2006;14(8):778-788.
- Logerstedt D, Lynch A, Axe MJ, Snyder-Mackler L. Pre-operative quadriceps strength predicts IKDC2000 scores 6months after anterior cruciate ligament reconstruction. Knee 2013;20(3):208-212.
- Reinke EK, Spindler KP, Lorring D, et al. Hop tests correlate with IKDC and KOOS at minimum of 2 years after primary ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 2011;19(11):1806-1816.
- Chung KS, Ha JK, Yeom CH, et al. Are muscle strength and function of the uninjured lower limb weakened after anterior cruciate ligament injury? Two-year follow-up after reconstruction. Am J Sports Med 2015 Oct 12. [Epub ahead of print]
- Pietrosimone BG, Saliba SA, Hart JM, et al. Contralateral effects of disinhibitory tens on quadriceps function in people with knee osteoarthritis following unilateral treatment. N Am J Sports Phys Ther 2010;5(3):111-121.
- Lepley LK, Palmieri-Smith RM. Cross-education strength and activation after eccentric exercise. J Athl Train 2014;49(5):582-589.
- Palmieri-Smith RM, Thomas AC, Wojtys EM. Maximizing quadriceps strength after ACL reconstruction. Clin Sports Med 2008;27(3):405-424.
- Bourke HE, Salmon LJ, Waller A, et al. Survival of the anterior cruciate ligament graft and the contralateral ACL at a minimum of 15 years. Am J Sports Med 2012;40(9):1985-1992.





