

Figure 1: A- Implanted plates in shoes; B- Arch support splints
By Pradhyum D. Kolhe , H V Sharath , Siddhi G. Rathi , Deepali S. Patil
Pes planus is also known as flatfoot. It comes from Latin words that mean pes as foot and planus as flat or ground level. Here, the medial longitudinal arch of the foot descends, resulting in a lack of spring action and increased stress on the entire foot with each step. It serves as an adaptive support base for the entire body, functions to dissipate the forces of weight bearing and acts to store energy during the gait cycle. The dysfunction of the arch complex typically does not present with symptoms; however, it can impact the biomechanics of the lower limbs and lumbar spine, leading to a higher likelihood of pain and injury. Occurrence of pes planus among children exceeds 70% during the initial 4 to 6 years of life, yet it has been documented to decline to approximately 9% post the age of 6.
Flatfoot is defined by the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes. Flat feet are commonly seen in orthopedic clinics and are usually functional and painless. The etiology of flatfoot remains elusive at present. Numerous studies propose a correlation between the debilitation of the intrinsic muscles of the foot and the diverse abnormalities that impact the foot arch, including both pes planus and pes cavus.
Case Presentation
A 20-year-old female arrived at the musculoskeletal department of physiotherapy with concerns about her walking difficulties. These difficulties were attributed to her developmental flatfeet and an underdeveloped heel on one foot, which she has had since birth. Despite these structural issues, her general examination showed no abnormalities, and she was able to maintain normal activity levels. Upon clinical examination, it was confirmed that she had bilateral flatfeet with decreased arches and an underdeveloped heel on 1 foot.
She was utilizing orthotic interventions such as arch support splints for both feet (Figure 1A) and implanted plates in her shoes (Figure 1B) to assist with balance while walking. Flatfoot was confirmed through the Fiess line test, as illustrated in Figure 2. On examination, manual muscle testing (MMT) (Table 1) was conducted on the patient with flatfoot before rehabilitation was given. It was observed that there was reduced strength in dorsiflexion and inversion movements compared to plantarflexion and eversion, indicative of possible muscle imbalances associated with the condition. The patient also complained of pain during strenuous activity. X-sens gait analysis was employed to examine and analyze gait patterns. However, apart from these foot deformities, no other significant abnormalities are noted. Neurologically, she displays normal muscle tone and strength in both lower extremities. Gait analysis indicated compensatory movements to adjust to the altered foot structure. With ongoing orthotic management and monitoring, her prognosis for maintaining functional independence remains positive.
Physiotherapy Management Intervention
Physiotherapy plays a pivotal role in the comprehensive management of patients with flatfoot, a condition characterized by the collapse or flattening of the arches of the feet. Through a tailored regimen of exercises and interventions, physiotherapists aim to alleviate symptoms, enhance foot strength, and improve overall biomechanics. The treatment protocol is typically designed for 2 months of duration with 5 days per week. It involves a combination of targeted exercises such as towel gathering, heel cord stretching, toe spreading, and posterior tibialis exercises. These exercises not only help in strengthening the intrinsic foot muscles but also promote flexibility

Figure 2: Fiess-line test
and alignment of the foot structures. Additionally, incorporating barefoot walking or engaging in activities without supportive footwear allows for natural movement patterns, facilitating proprioceptive feedback and muscle activation. Table 2 displays a well-designed exercise protocol for foot rehabilitation. Under the guidance of a physiotherapist, patients embark on a journey of rehabilitation, gradually restoring function and stability to their feet. Through consistent dedication to the prescribed program, individuals with flatfoot can experience significant improvements in pain management, mobility, and overall quality of life, thereby highlighting the invaluable role of physiotherapy in the holistic management of this condition.
Outcome measures for this intervention included a visual analog scale to assess pain levels during strenuous activities of the patient, along with foot assessment scales such as Foot Function Index (FFI), Foot and Ankle Ability Measures (FAAM), and Foot Posture Index (FPI), as mentioned in Table 3.
Post-intervention, orthotic management and ongoing monitoring have been initiated to facilitate functional independence.
Discussion
Pes planus is a prevalent condition marked by the collapse of the medial arch, abduction of the forefoot, internal rotation, plantar flexion of the talus, and eversion of the calcaneus. Subotnick reported that pes planus is observed in 20% of the overall population. Khamis and Yizhar et al concluded that changes in foot structure can have an impact on adjacent body segments due to the interconnected nature of the body’s structures, which can be likened to a chain reaction manner. Indeed, according to Precilla et al, the kinematic chain exercise has demonstrated a significant impact in reducing pain from flatfeet, resulting in noticeable improvements in foot function and balance as well.

Figure 3: A- Achilles tendon stretching and B- Strengthening of Posterior Tibialis
The present case has difficulty in walking due to flatfeet and an underdeveloped heel highlights the importance of physiotherapy in treating such conditions. Physiotherapists play a vital role in dealing with the issues caused by flatfeet by using specific exercises and treatments to reduce symptoms and enhance foot mechanics. The recommended 2-month treatment plan, which includes exercises such as towel scrunches, heel stretches, toe spreads, and posterior tibialis exercises done 5 times a week, shows potential in strengthening the muscles in the feet and improving their flexibility and alignment. Encouraging activities without shoes also helps promote natural movements, which aids in providing feedback to the muscles and activating them.
The exercise plan provided in Table 2 offers a comprehensive approach to foot rehabilitation, highlighting the diverse aspects of physiotherapy in addressing concerns related to flatfeet. Towel-gathering exercises, for instance, help strengthen the intrinsic foot muscles. Meanwhile, heel cord stretching promotes flexibility in the Achilles tendon and calf muscles, essential for achieving proper foot alignment during gait. Furthermore, incorporating exercises that target toe spreading and activate the posterior tibialis muscle aids in stabilizing and providing support to the arches of the foot. Strengthening the posterior tibialis muscle, in particular, is pivotal in preventing excessive pronation and supporting the medial longitudinal arch.
FFI is a self-administered survey utilized for evaluating how foot problems or injuries affect a person’s capacity to carry out everyday tasks. Visual analogue scale is used to check pre- and post-rehabilitation pain level. FAAM is a questionnaire that individuals complete to assess their functional limitations and disabilities associated with foot and ankle conditions. FPI is a clinical tool used to assess the static alignment of the foot and ankle complex.
A cross-sectional investigation was carried out to assess and contrast the reliability and diagnostic precision of the FPI-6 and Clarke’s angle (CA) in identifying flexible flatfoot in adolescents age 12 to 18 years, taking into account radiographic examination as the benchmark measure. In their systematic review, Hara et al analyzed the impacts of short-foot exercise (SFE) in contrast to foot orthosis or alternative forms of interventions. Physiotherapy interventions focus on these particular muscle groups to address biomechanical abnormalities linked to flatfoot, ultimately relieving symptoms and enhancing functional outcomes.
Conclusions

Figure 4: Golf ball rolling exercise
In this case study, the efficacy of foot rehabilitation exercises in managing painful flatfoot in a 20-year-old female was investigated. The patient’s presentation with foot pain and discomfort due to flatfeet significantly impacted her daily functioning and quality of life. Through a structured rehabilitation program comprising targeted exercises, stretching, and orthotic intervention, notable improvements were observed in pain reduction, functional mobility, and foot posture. The implementation of a personalized exercise regimen focusing on intrinsic foot muscle strengthening, arch support enhancement, and proprioception improvement played a pivotal role in addressing the underlying biomechanical issues contributing to painful flatfoot. Moreover, incorporating stretching exercises helped alleviate muscle tightness and enhance flexibility, augmenting the effectiveness of the rehabilitation program. This case study underscores the importance of tailored rehabilitation protocols to meet individual needs in patients with painful flatfoot. By targeting biomechanical abnormalities, strengthening intrinsic foot muscles, and optimizing foot posture, clinicians can effectively alleviate symptoms, enhance functional outcomes, and improve overall quality of life for individuals with this condition. Further research and larger-scale studies are warranted to validate these findings and elucidate the long-term efficacy of foot rehabilitation interventions for painful flatfoot. Ultimately, continuous studies on foot rehabilitation not only improve clinical procedures but also play a fundamental role in fostering overall wellness and reinstating functional autonomy for individuals.
Authors Pradhyum D. Kolhe, H.V. Sharath, and Siddhi G. Rathi, are with the Department of Paediatric Physiotherapy at Ravi Nair Physiotherapy College, Datta Meghe Institute of Higher Education and Research (DU) Sawangi Meghe, in Wardha, India.
Author Deepali S. Patil is with the Department of Musculoskeletal Physiotherapy at Ravi Nair Physiotherapy College, Datta Meghe Institute of Higher Education and Research (DU) Sawangi Meghe, in Wardha, India.
This article has been excerpted from “Effect of Foot Rehabilitation Exercises for Painful Flat Foot in a 20-Year-Old Female: A Case Study Analysis,” by the same authors, which was originally published in Cureus 2024;16(4): e59377. DOI 10.7759/cureus.59377. Editing has occurred, including the removal of references for brevity. Use is per CC Attribution 4.0 International License.

Table 1: Pre- and Post-rehabilitation Manual Muscle Testing (MMT)
MMT- 0: No evidence of muscle contraction; 1: Trace contraction, but no movement; 2: Movement with gravity eliminated (passive range of motion); 3: Movement against gravity, but without resistance; 4: Movement against gravity and some resistance; 5: Normal strength, movement against full resistance
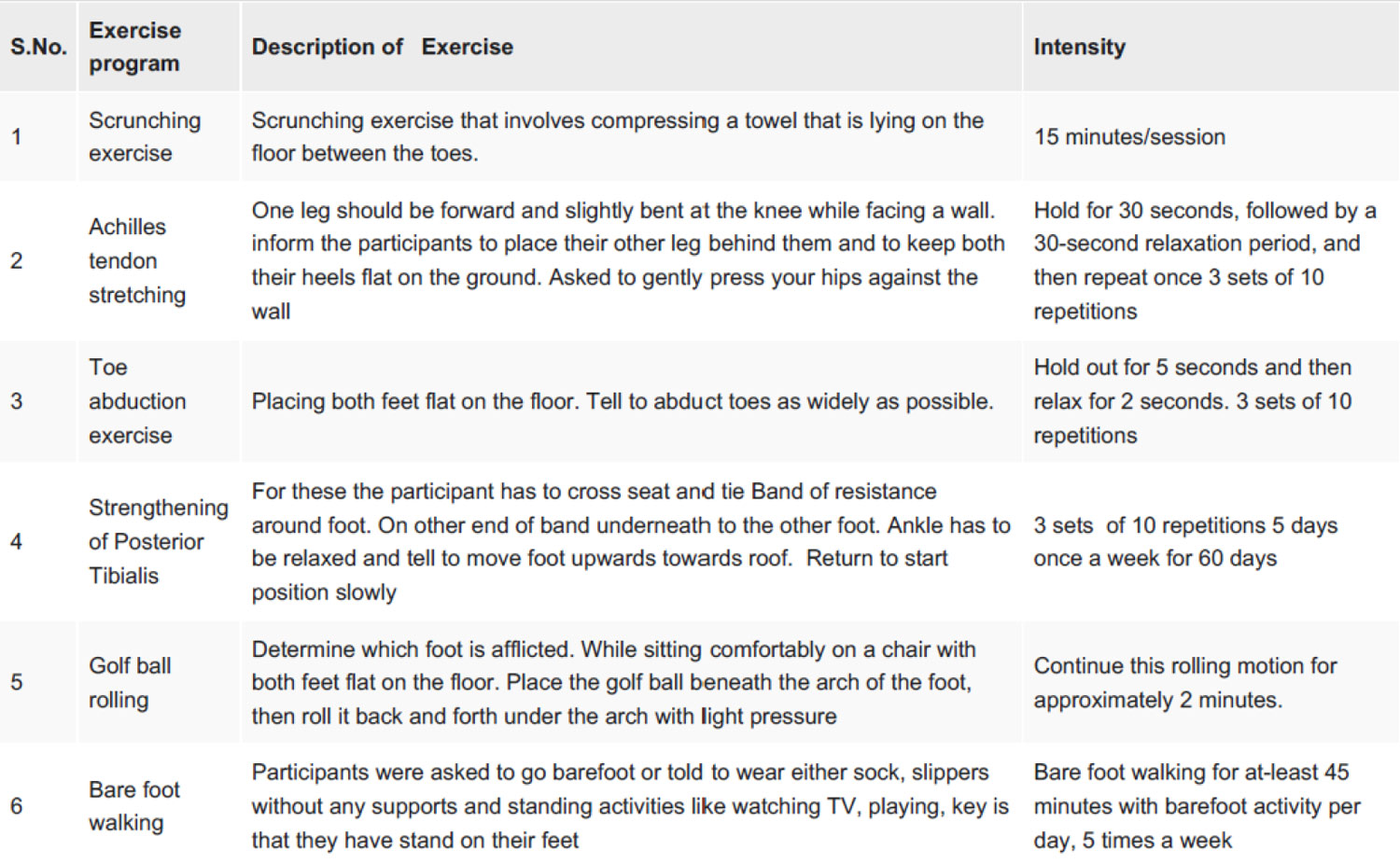
Table 2: Optimized exercise protocol for flatfoot rehabilitation
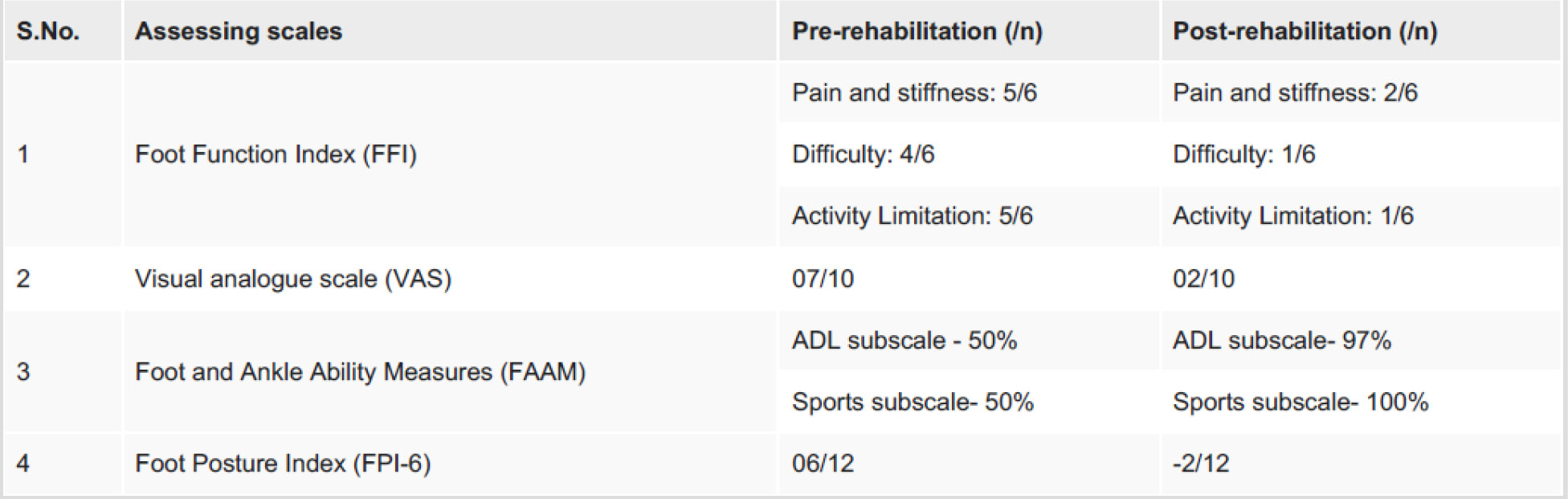
Table 3: Pre- and Post-rehabilitation Assessments for flatfoot
FFI: Pain: 1: No pain; 2: Mild pain; 3: Moderate pain; 4: Severe pain; 5: Very severe pain; 6: Worst pain imaginable; Difficulty: 1: No difficulty; 2: Mild difficulty; 3: Moderate difficulty; 4: Severe difficulty; 5: Very severe difficulty; 6: So difficult unable; Activity limitation 1: None of the time; 2: A little of the time; 3: Some of the time; 4: Much of the time; 5: Most of the time; 6: All of the time
VAS: 0: No pain; 10: Worst pain
FAAM: Higher (100%) the score lesser the disability
FFPI-6: Normal: 0 to +5; Pronated: +6 to +9, Highly Pronated +10: Supinated: -1 to -4, Highly supinated -5 to -12





