

Midfoot relast for Charcot foot deformity, shown with foot cast and custom foot orthosis.
By Erick J. Janisse, CO, CPed
Much has been written about the problem of less-than-ideal patient adherence to use of therapeutic and custom footwear for management and prevention of diabetic foot complications. Over the last few decades, there have been numerous research projects, surveys, and studies designed to parse out the exact reasons for low adherence and to create real world, implementable solutions.
Some researchers conclude that the lack of perceived value or benefit of specialized footwear from the patient’s perspective is to blame.1,2 This is most certainly true, and a real challenge for not only pedorthists, orthotists, and shoe fitters, but for physicians, as well. Other studies, though, point to the culpability of the shoes’ poor aesthetics.3,4 And some suggest that if the patient had a wider and/or more consistent selection of footwear, adherence would likely improve.3,5
There’s more to this, however. A 2018 article by Nicholls et al in Journal of Foot and Ankle Research hit the nail on the head.6 The goal of their narrative review was to explore the sociology of footwear and discover ways to apply previous sociological findings about people and their shoes to improve patient adherence to therapeutic footwear – and not solely in patients with diabetes. The authors pointed out that shoes are not merely “neutral” objects, but rather, in many cases, shoes are the most expensive part of a person’s outfit. They refer to previous sociological research that demonstrates just how important the role of footwear is presentation and management of oneself, body, and identity. One study referred to in the article is a 2018 study by Williams et al published in BMC Musculoskeletal Disorders and examined the therapeutic footwear experiences of patients with rheumatoid arthritis.7 One of their conclusions was that, “[u]nlike any other intervention specialist therapeutic footwear replaces something that is normally worn and is part of an individual’s body image. It has much more of a negative impact on the female patients’ emotions and activities than previously acknowledged and this influences their behaviour with it.” They also pointed out that, “[f]or several participants, orthopaedic or specialist footwear also compounded an existing negative self-image and could be linked with feelings of shame, anger, and humiliation. Those who did wear their prescribed footwear frequently suggested that it could limit their engagement with social activities.” These are very real considerations that are frequently overlooked, undervalued, or misunderstood by referring physicians and orthotics, prosthetics, and pedorthic (OP&P) providers.
Even though there are many fine, reputable, and talented custom shoemakers and respected custom shoe companies in existence today, many within our profession and related professions would not consider most therapeutic custom footwear to be “normal looking”. Herein lies the problem. In a therapeutic context, the only instances where a pedorthist resorts to provision of custom shoes are when the patients’ deformities are so severe in nature that they simply cannot be accommodated by any so-called off-the-shelf shoes. Despite the custom shoemaker’s best attempts, the shoes inevitably look quite a bit like the patient’s deformed feet. There is no escaping the self-consciousness brought on by–and the stigma attached to–having to wear such shoes.
 Admittedly, there are, and always will be, situations where custom shoes truly are the only practical option for a given patient. In many cases, though, there are alternatives. Many therapeutic or orthopedic footwear manufacturers offer in-depth shoes, double-depth shoes, and the availability of mismating sizes and widths left-to-right in order to accommodate unusually shaped feet as best as possible. There are even triple-depth shoes available in extreme sizes and widths from companies like Apis that can accommodate a great many of the feet with which this article is concerned.
Admittedly, there are, and always will be, situations where custom shoes truly are the only practical option for a given patient. In many cases, though, there are alternatives. Many therapeutic or orthopedic footwear manufacturers offer in-depth shoes, double-depth shoes, and the availability of mismating sizes and widths left-to-right in order to accommodate unusually shaped feet as best as possible. There are even triple-depth shoes available in extreme sizes and widths from companies like Apis that can accommodate a great many of the feet with which this article is concerned.
There is one last, more aesthetically pleasing, alternative to custom shoes. Relasting. That is, using a relatively normal looking shoe – sometimes even a shoe that the patient already had in their closet – and customizing it by widening the sole to accommodate their foot deformities or painful prominences. Relasting frees up the patient and pedorthist to select from a wider variety of socially acceptable and cosmetically satisfactory footwear. When the patient looks down at their shoes, they see normal shoes that won’t garner unwanted attention…and they themselves, in turn, feel more normal (and more likely to wear the shoes as prescribed).
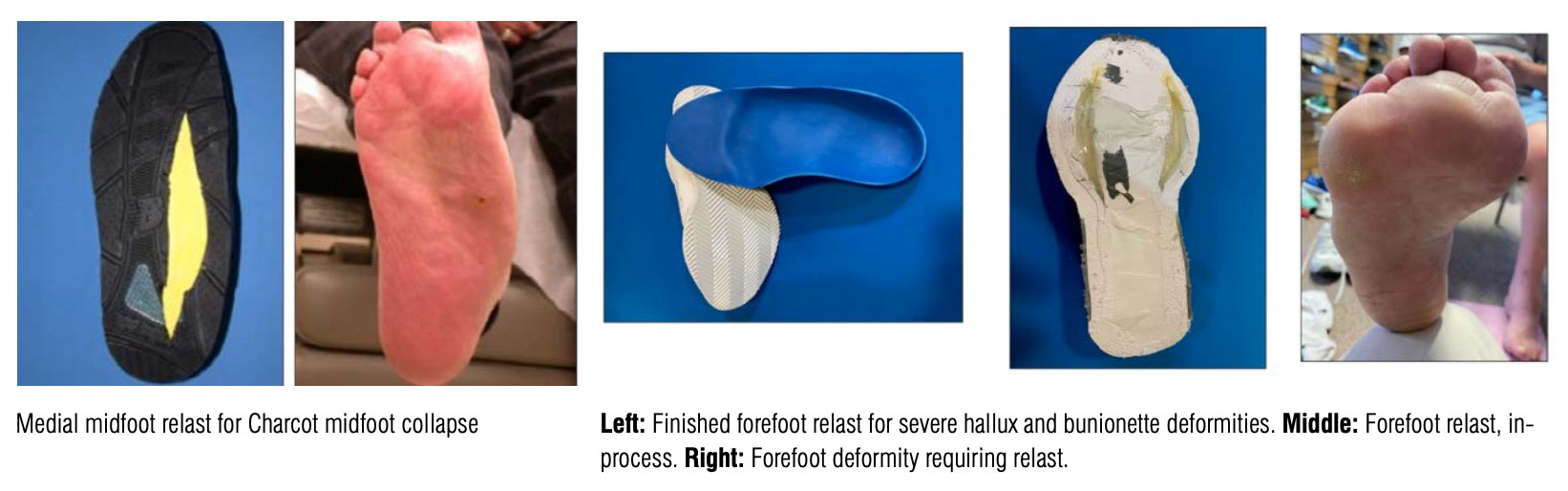
Relasts can be applied to great effect for patients with Charcot arthropathy, prominent bases of fifth metatarsals, severe bunion or bunionette deformities, wide transmetatarsal amputations and a host of other conditions and deformities.
For a relast to be a long-lasting and successful solution, there are some important factors to consider. The shoe must be appropriate to start with – for both the foot and the modification. That is, it must be as close to properly fitting before modification and the sole construct must have enough structural integrity to undergo the modification. Another important consideration is that, regardless of what is done to the sole, the upper will always only have the same fixed amount of material. This means that by widening the shoe, the depth is necessarily decreased, and, in the case of an extreme widening, the length of the shoe may be shortened slightly.
The modification, while requiring the necessary time and skill set to perform, is straightforward and simple. The outsole is carefully cut off the shoe. The shoe is cut longitudinally with a jigsaw (if the shoe is board-lasted or has a midsole; if it is slip-lasted, it can be cut with a sharp knife) and the cut is wedged open to fit a pattern created from a weightbearing tracing of the patient’s foot. Blocks of firm crepe or neoprene are placed into the cut to hold it open, and a cardboard dam is glued to the topside of the insole inside the shoe. The gaps are filled with a very firm viscoelastic polymer like PQ® Gel by Riecken’s or a rigid expanding foam. Once the filler is set, the surface is sanded smooth and level, and a new outsole is applied. The relasted shoe will need to be used in conjunction with a custom foot orthosis made to fit the shape of the modified shoe.
Relasts can be done in any part of the shoe. For obvious reasons, the midfoot is the easiest. The forefoot and hindfoot are more involved and challenging but can certainly be done. Relasts in the hindfoot may also necessitate modification of the counter itself.
Keep in mind, however, that the relasted shoe is a customized shoe and not a custom shoe. Therefore, it may not be billed as a custom shoe. The code L3254 may be used to bill for a relast if the modified shoe is an integral component of a lower extremity bracing system attached to the shoe. Outside of that, however, it will most likely be an out-of-pocket expense for the patient. Even so, once the patient tries the new shoe, be prepared for a happy patient and many more requests for additional shoes to be relasted.
Erick J. Janisse, CO, CPed, a certified orthotist and pedorthist, is Sales Training Manager at Enovis (formerly DJO) and Program Director for Midwest School of Modern Pedorthics in Mequon, Wisconsin.
- Macfarlane DJ, Jensen JL. Factors in diabetic footwear compliance. J Am Podiatr Med Assoc. 2003;93(6):485-91. doi: 10.7547/87507315-93-6-485.
- Arts ML, de Haart M, Bus SA, Bakker JP, Hacking HG, Nollet F. Perceived usability and use of custom-made footwear in diabetic patients at high risk for foot ulceration. J Rehabil Med. 2014;46(4):357-62. doi: 10.2340/16501977-1272.
- Knowles EA, Boulton AJ. Do people with diabetes wear their prescribed footwear? Diabet Med. 1996;13(12):1064-8. doi: 10.1002/(SICI)1096-9136(199612)13:12<1064::AID-DIA253>3.0.CO;2-#.
- Waaijman R, Keukenkamp R, de Haart M, Polomski WP, Nollet F, Bus SA. Adherence to wearing prescription custom-made footwear in patients with diabetes at high risk for plantar foot ulceration. Diabetes Care. 2013;36(6):1613-8. doi: 10.2337/dc12-1330.
- Jarl G, Tranberg R, Johansson U, et al. Predictors of adherence to wearing therapeutic footwear among people with diabetes. J Foot Ankle Res. 2020;13:45. https://doi.org/10.1186/s13047-020-00413-z.
- Nicholls E, Robinson V, Farndon L, Vernon W. ‘A good fit?’ Bringing the sociology of footwear to the clinical encounter in podiatry services: a narrative review. J Foot Ankle Res. 2018;11:9. doi: 10.1186/s13047-018-0253-6.
- Williams AE, Nester CJ, Ravey MI. Rheumatoid arthritis patients’ experiences of wearing therapeutic footwear – a qualitative investigation. BMC Musculoskelet Disord. 2007;8:104. doi:10.1186/1471-2474-8-104.





