
Figure 1. In the neutral foot, the area of skin immediately superficial to the talo-navicular joint becomes more prominent if the head of the talus is adducted in rearfoot pronation. Bulging in the area of the talo-navicular joint is thus associated with a pronating foot. In the supinated foot, this area might be indented. Image from Olesky L et al. Intrarater reliability of the Foot Posture Index (FPI-6) applied as a tool in foot assessment in children and adolescents. Med Rehab. 2010;14(4:10-20). Use is per Creative Commons license CC BY-SA 4.0. Available at https://rehmed.pl/resources/html/article/details?id=136198.
Recent analysis of the podiatric literature concludes that custom foot orthoses aren’t superior to prefab inserts—an account one expert rejects. It’s a matter of who does the custom work, he says.
By STANLEY BEEKMAN, DPM
This article is adapted, by Dr. Beekman and the Editors of LER, from his podium presentation at the Richard O. Schuster, DPM, Memorial Biomechanics Seminar, sponsored by the New York College of Podiatric Medicine, in New York City, November 2018. At that presentation, Dr. Beekman reviewed and critically reconsidered the findings of studies of the efficacy of custom foot orthoses in managing mechanically induced plantar heel pain.
—The Editors
In March 2018, the British Journal of Sports Medicine published Nadine Rasenberg, PhD,a and her coauthors’ systematic review and meta-analysis of the literature on the efficacy of foot orthoses for plantar heel pain1 (I’ll refer to the paper simply as “Rasenberg’s”). The next day, on March 19, a United Press International headline read: “Pricey insoles aren’t worth the cost.” On March 21, Reuters’s coverage began with “Shoe inserts may not help plantar heel pain.”
I soon came to the realization that there are concerns about the reliability and validity of the Rasenberg paper. Why? In part because of our collective experience: At the Schuster Memorial Biomechanics Seminar later that year, when speaking about Rasenberg’s work, I asked the audience if anyone had ever had a patient present with a prefabricated device that didn’t work and, by making a functional orthosis for that patient, their condition had improved.
Every participant raised their hand—in the affirmative.
My aim in this article, as it was in my Schuster presentation, is to provide a critical examination of Rasenberg’s work and of the studies included in her meta-analysis. Are “pricey insoles” worth the cost?
What Rasenberg Said
In the British Journal of Sports Medicine paper, Rasenberg stated:
Five studies compared prefabricated orthoses with custom-made orthoses. All studies provided data that could be used for pooling. No difference was found on short-term pain… between prefabricated and custom-made orthoses. […] One study reported self-reported recovery at short term and found a significant effect… in favour of prefabricated orthoses. […] In summary, foot orthoses are not superior for improving pain and function compared with sham or other orthoses.1
Background: What, Exactly, is a Custom Foot Orthosis?
Rasenberg did not define “custom foot orthosis” (CFO) in her paper. An Internet search reveals that most definitions are provided by orthotics laboratories, which might be biased in defining a CFO. The definition offered by the Canadian Life and Health Insurance Association, Inc., seems appropriate:
Custom made foot orthotics are functional devices made from a directly-molded impression of the patient’s full contours of the foot using plaster, slipper cast made of resin, foam impression, wax or 3D scan. The foot orthotic is constructed from raw materials and manufactured to each patient’s individual prescription. The foot orthotic is removable from the patient’s footwear. […] Generally, in order to be eligible for coverage under a group benefit plan the orthotics must be prescribed by the appropriate medical professional before the purchase is made.2
There are 4 main criteria necessary to meet that definition, according to the Association’s description. The device must be:
- functional
- prescribed for the individual patient
- made to a negative mold
- prescribed by an appropriate medical professional.
Criterion #1: Functional—Dr. Schuster (to whom the Memorial Biomechanics Seminar is a tribute) told me: “Foot orthoses change the surface we walk on from one that is flat and level that requires the body to adapt to, to one that does not require these adaptations” (Schuster R, personal communication, 1974). The 4 changes produced by a foot orthosis are:
- frontal-plane corrections for varus or valgus deviation
- heel height for equinus
- heel lift, with or without a sole lift (applied to a shoe), for leg-length differences
- possibly, correction to allow the first ray to plantarflex at propulsion.
For a device to be functional, it has to be made appropriately. That requires recognition (through biomechanical examination) of why excessive pronatory compensation is taking place, an ability to find the neutral position, and appropriate posting to attempt to maintain that position.
Criterion #2: Prescribed individually—An individual prescription should address the 4 imbalances listed above. This can be done by static or computerized gait examination, or both. One evaluation used outside the United States is the Foot Posture Index,3 developed by a collaboration of esteemed podiatrists at notable universities in Great Britain and Australia. The index uses several parameters, including bulging of the talo-navicular joint (Figure 1b).
Criterion #3: Uses a negative mold—It is impossible to make a custom orthosis without a negative mold. A negative mold can be obtained via plaster casting, foam impressions, or digital scanning. Factors that are captured by a negative mold include the width of the heel; width of the forefoot; metadductus angle; the metatarsal length (the angle a line drawn connecting the first and fifth metatarsal makes with the long axis of the foot); the height of the medial arch; the height of the lateral arch; and if needed, the exact areas to place metatarsal pads, toe crests, cuboid pads, and the ends of heel raises.
Criterion #4: Prescribed by an appropriate medical professional—Asking who is an “appropriate” medical professional raises more questions than it provides answers, in regard to education and to experience in prescribing, fabrication, dispensing, and follow-up. Should education be equivalent to that of a US podiatrist—ie, the doctorate level? Even the American Board for Certification in Orthotics, Prosthetics, and Pedorthics requires a minimum of 500 hours of orthotic fitting prior to certification.4

Figure 2. A sampling of uncharacteristic feet. Casting by the author.
Instead, a simpler method to determine who is an “appropriate” medical professional would be results-based: How difficult would it be for someone to make a foot orthosis that outperforms a prefabricated device—especially because there are a number of feet of uncharacteristic shapes, including metatarsus adductus, forefoot splay, accessory navicular, and prominent styloid process (Figure 2)? Imagine an optometrist who isn’t able to prescribe a pair of glasses that outperforms an off-the-shelf pair; would you say, based on this optometrist’s ability, that off-the-shelf glasses perform better? Or that the optometrist isn’t adequately trained?

With that notion in mind, the focus of this article is to determine whether the orthoses used in the studies that were the basis of Rasenberg’s paper were properly made and whether they were truly “custom.” And because meta-analyses focus on the possibility of hidden bias, I’ll also raise the question of bias in areas not addressed by Rasenberg.
Rasenberg’s Review and Meta-analysis
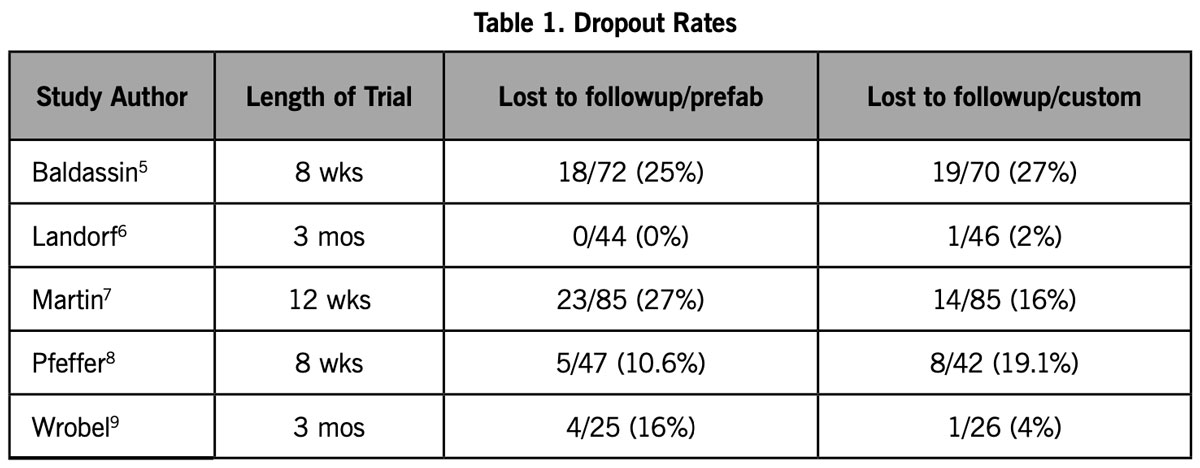
Rasenberg reviewed 895 studies, 38 of which were utilized for her paper. The section dealing with a comparison of CFOs to prefabricated arch supports used 5 studies: those of Baldassin,5 Landorf,6 Martin,7 Pfeffer,8 and Wrobel.9
To ensure no hidden bias, Rasenberg evaluated 12 parameters to determine which studies were unbiased. The higher the number of those parameters, the less the bias. The selection of articles and the minimization of the risk of bias assume that there is no bias on the part of the studies’ author(s).
Earlier statements are revelatory—On closer look, however, this might not be the case. In 2015, Rasenberg published an article on the so-called STAP (Soles as Treatment Against Pain) study, a randomized controlled trial that examined the cost-effectiveness of CFOs for plantar fasciopathy in general practice and sports medicine.10 In that paper, she stated: “The secondary objective of our study is to examine the cost-effectiveness of custom made insoles by a podiatrist, compared to usual care in patients with plantar fasciopathy.”
Rasenberg also stated, in her 2015 paper, that “the standardized intake at the podiatrist will consist of an examination of the posture of the foot using the standardized Foot Posture Index,[27] the Hubscher test,[28] the navicular drop test[29] and the range of motion in the tarsometatarsal joint and the first metatarsophalangeal joint (MTP-I) as measured with a goniometer.” Earlier, I mentioned the Foot Posture Index, but there are no standardized podiatric tests to show the 4 imbalances previously discussed: functional hallux limitus, frontal plane deviations, asymmetry, and equinus.
Furthermore, the 2015 study mistakenly lumps podiatrists into the same category worldwide. In the Netherlands, podiatry is a 4-year, accredited, full-time Bachelor of Science course11; in the United States, it is a postgraduate doctoral course.
Rasenberg goes on to say in the 2015 paper that “the podiatrists will report for each patient, whether they agree with the indication for orthotic insoles as established by the GP or sports physician.” In the United States, the podiatrist determines the indication for a foot orthosis.
Further down, Rasenberg states that “orthotic devices seem to be a frequently applied treatment option, despite a lack of evidence on the effectiveness.” She references Thomas12 and Covey.13
Interestingly, Thomas states, “The second tier of the treatment ladder includes continuation of the initial (Tier 1) treatment options with considerations for additional therapies: orthotic devices [75 to 78]….”12 References 75 through 78 in the cited Thomas paper in fact support the use of orthoses:
- “The present study demonstrates a significant difference after using the functional orthosis for 8 weeks in foot pain and foot function (FHSQ [Foot Health Status Questionnaire] and overall health status (EQ-5D [questionnaire])”14 (original reference 75)
- “The meta-analysis results showed significant reductions in pain after orthotic intervention”15 (original reference 76)
- “Mechanical control of the foot is a successful method of treating plantar fasciitis. Custom-made orthoses, over-the-counter arch supports, and tension night splints are all effective as initial treatments for plantar fasciitis. Patients in the present study demonstrated the best compliance with the use of custom-made orthoses, which may indicate that orthoses provide the best long-term results”7 (original reference 77 [this paper was also used in the 2018 Rasenberg paper1]).
- “23 patients have been fitted with the University of California Biomechanics Laboratory (UCBL) Shoe Insert for plantar fasciitis. In the last 15 months a total of 10 patients have been fitted with the insert at the UCLA Rehabilitation Center in Los Angeles. Most of these patients had been treated previously with arch supports, heel cushions, steroids, and phenylbutazone, without success. In all but 2 cases the relief from discomfort with the shoe insert was almost instantaneous”16 (original reference 78).
In defense of Rasenberg, Covey’s article13 cited a Cochrane review17 that found no difference in pain reduction between CFOs and prefabricated foot orthoses. This assertion came from a paper by Hawke,17 which, in turn, was based on papers by Landorf,6 Martin,7 and Pfeffer.8 Those 3 papers are among the 5 analyzed in Rasenberg’s 2018 systematic review and meta-analysis.
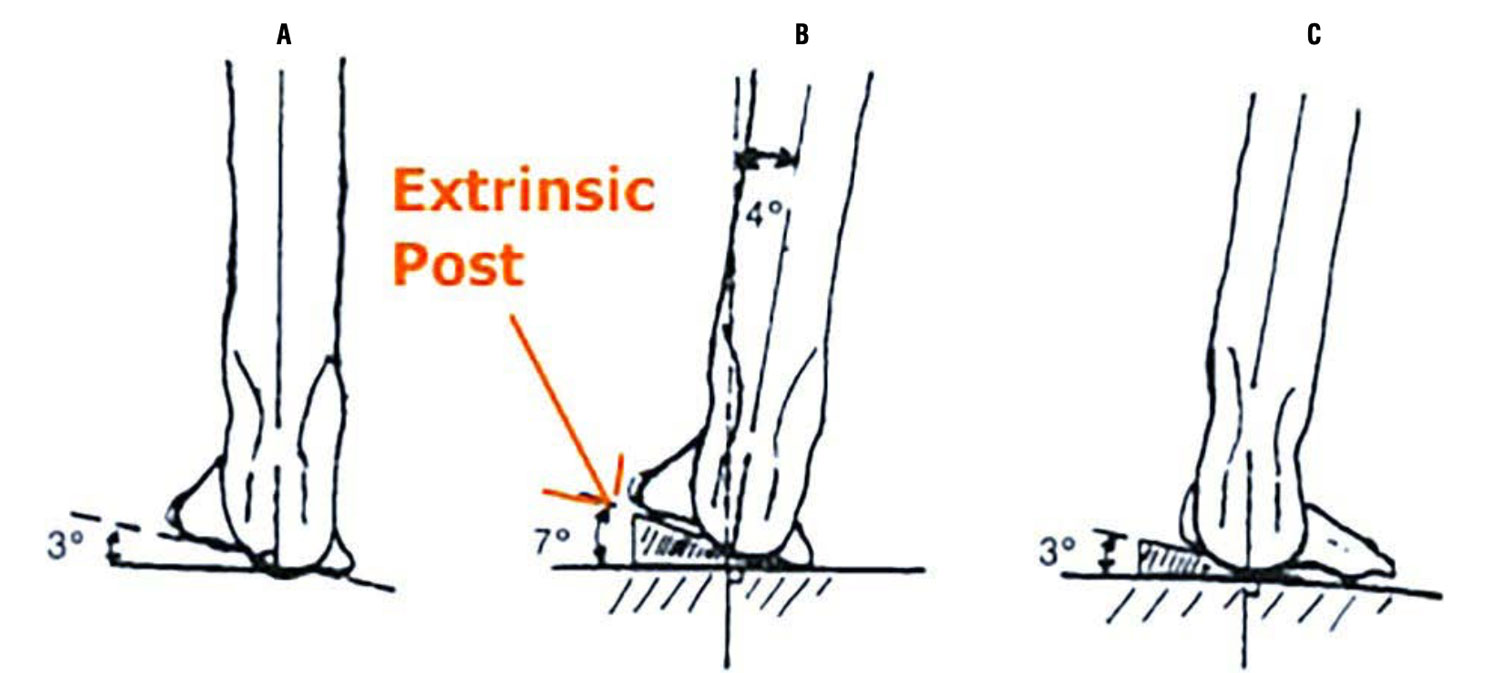
Figure 3. A: Casted position. Subtalar join is neutral; forefoot varus = 3°. B: Rearfoot varus, 4°; forefoot varus, 3°. High oblique midtarsal joint axis. C: The orthosis is forefoot-posted in 3° varus, placing the heel vertical in stance. The subtalar joint is pronated 4° from neutral. The forefoot pronates off the orthosis. Reprinted from Hice GA. Orthotic treatment of feet having a high oblique midtarsal joint axis. J Am Podiatry Assoc. 1984;74(11):577-582. Used with permission of the American Podiatric Medical Association, all rights reserved.
The 5 Papers Examined
Because Rasenberg did not define “custom orthosis,” my review of the 5 papers she analyzed in her 2018 study1 largely focuses on whether or not (1) the orthoses used in the papers fit the definition of a CFO and (2) there was possible bias not found by Rasenberg.
Martin: Prospective study—This paper7 is important not only because it was used in Rasenberg’s 2015 paper but also in Covey’s paper13 that was the basis for Rasenberg stating that “orthotic devices seem to be a frequently applied treatment option, despite a lack of evidence on the effectiveness ….” Martin, a podiatrist from the United States, performed a biomechanical examination on the subjects in his study, which included checking for equinus and frontal plane deviations.
The impression for the CFO was made using laser scanning. The orthoses were 5mm Polydur (Bergmann Orthotic Laboratory, Northfield, IL), with a 4° rearfoot post, with intrinsic posting allowing 4° pronation. The prefabricated device was Foot Soldiers (Foot Soldiers, Professional Footcare International, Inc., Valencia, CA). Both groups were taped for 2 weeks prior to receiving the CFO or prefabricated orthosis.
Martin made the CFO according to the previously noted 4-criteria definition. He concluded that “the group using custom-made orthoses showed the greatest improvement over time.”17
Landorf: Review of trials—This paper6 is especially important because it appears to be well-researched and was one of the 3 papers in the Cochrane review17 quoted by Covey,13 on which Rasenberg based her question about the efficacy of orthoses. Landorf, a podiatrist from Australia (ie, he has a baccalaureate in podiatry), stated:
Each participant was assessed using a standardized assessment by the investigator, an experienced podiatrist (K.B.L.). Neutral position plaster casts were taken by the investigator; […] The customized foot orthosis was fabricated at a commercial orthotic laboratory (The Orthotic Laboratory, Melbourne, Australia) using principles described by Hice.[18] A plaster cast was posted to the neutral calcaneal stance position, and a hard plastic shell was vacuum molded over the cast. [… A] firm foam heel post was applied inferior to the heel.
The prefabricated device used was not named; however, at the end of the article, the statement of funding and support says: “The Orthotic Laboratory, Foot Science International, and Allied Health Industries donated orthoses and orthotic materials.” Note that Foot Science International makes a prefabricated support called Formthotics.
Although Landorf states that he used principles described by Hice,18 this does not appear to be the case. Hice was concerned about the forefoot abducting, relative to the rearfoot, therefore sliding laterally off the orthosis. He attributed this to inadequate posting of a foot with a high oblique midtarsal joint axis. Hice makes this clear by stating that:
Casting a foot with the subtalar joint in neutral and the midtarsal joint stable in the direction of pronation captures a specific forefoot-to-rearfoot relationship. An orthotic shell made from this cast has a forefoot-to-rearfoot relationship that is unaltered by either a forefoot post or rearfoot post.18
In his illustrations, Hice shows an extrinsic forefoot post; in another place, he states:
The orthosis will be generally comfortable. If the orthotic front edge irritation occurs because of forefoot posting height, a Morton’s extension made of flexible material (Korex) may be incorporated into the device. [Figure 3]18
However, Landorf clearly uses intrinsic posting as he describes the methodology: “A plaster cast was posted to the neutral calcaneal stance position, and a hard plastic shell was vacuum molded over the cast.”
When looking at the data, a dropout rate of ≥ 25% is a factor in considering hidden bias. Landorf’s data aside, in the papers that Rasenberg reviewed, the dropout rate ranged from 10.6% to 27% in the prefabricated group and 4% to 27% in the CFO group. When looking at Landorf’s data alone, he had the lowest dropout rate: 0% in the prefabricated group and 2% in the CFO group (Table 1). This, by itself, would not seem that significant—except that, in an earlier (1998) article,19 of which Landorf is a coauthor, it is stated that:
With this in mind, the Australian Podiatry Council and state associations have, in recent years, identified a number of issues for consideration concerning podiatric orthoses…. These include community concerns in regard to efficacy, cost and clinical outcomes as well as increasing competition from alternative suppliers. In response to these concerns, and following widespread consultation, the Council adopted a number of strategies, which had, as a fundamental basis, the development of Australian clinical guidelines for podiatric prescription orthoses.19
The possibility of hidden bias should therefore have eliminated the Landorf article from the Rasenberg meta-analysis. His conclusions, not surprisingly, are: “At this stage, it is not possible to conclude that either prefabricated or customized orthoses are better, and it cannot be suggested that customized orthoses are better over time and therefore have a cost advantage.”6
Pfeffer: Prospective trial—This also is an important paper,8 not only because it was cited in Rasenberg’s 2015 paper, but because it was used in Covey’s paper that was the basis for Rasenberg stating that “orthotic devices seem to be a frequently applied treatment option, despite a lack of evidence on the effectiveness.”
Pfeffer is an orthopedic surgeon from the United States. All patients were examined by an orthopedic surgeon at each center who specialized in foot and ankle disorders. There was no biomechanical examination. The prefabricated devices used were a silicone heel pad (Bauerfeind, Atlanta, GA), a felt insert (Hapad, Bethel Park, PA), and a rubber heel cup (Tuli’s).
Pfeffer states:
Each center had reviewed a Prolab instructional video on casting technique. The orthoses were made from a negative cast of the patient’s foot while the subtalar joint was in a neutral position. Either ¼ inch or 3/16 inch polypropylene was used for each orthosis, with the thickness determined by the weight of the patient.8
 However, the video on the Prolab Web site runs 10 minutes and 25 seconds. The narrator says: “Neutral is by feeling for congruency of the STJ or lining the second metatarsal with the long axis of the leg. Do not pronate or supinate the foot but keep it in neutral.” Instruction on the neutral position lasts 17 seconds—inadequate, because this skill is an important one and requires instruction to perform properly.
However, the video on the Prolab Web site runs 10 minutes and 25 seconds. The narrator says: “Neutral is by feeling for congruency of the STJ or lining the second metatarsal with the long axis of the leg. Do not pronate or supinate the foot but keep it in neutral.” Instruction on the neutral position lasts 17 seconds—inadequate, because this skill is an important one and requires instruction to perform properly.
Furthermore, Pfeffer is a member of American Orthopedic Foot and Ankle Association. As for possible hidden bias, see “Clearing up the misconceptions of orthopedic surgeons over the VA Provider Equity Act” in a 2016 posting on the Podiatry Today Web site,20 regarding orthopedic surgeons vs. podiatrists.
Knowing the above, Pfeffer’s results aren’t surprising: All 5 treatment groups demonstrated improvement in both pain scales at 8-week follow-up. The Foot Function Index, when controlled for covariates (baseline pain, duration of pain, and history of similar heel pain), indicated that the greatest diminution in pain was in the rubber insert and silicone insert groups, followed by the felt insert, stretching-only, and CFO groups.8
Baldassin: Double-blind trial—The paper’s author is a physical therapist; his coauthors are a physician and a PhD. All are from Brazil. Baldassin states:
One hundred forty-two patients out of 248 evaluated were randomly allocated to receive a prefabricated or customized foot orthoses (both 95% EVA [ethylene vinyl acetate]) [….] The customized foot orthosis was made from a nonplaster casting technique. This implies that the molds from the patients’ feet were taken in the proper foam (EVA), and it was not necessary to make a negative cast.5
No mention is made of a biomechanical exam. Furthermore:
During this modeling process, the expert held the subtalar joint in a neutral position. The next step consisted of joining the 2 remaining plates of EVA under the single foam plate, already molded and cooled, in water to prevent any undesirable material deformity. Afterward, the expert cut and shaped the insole according to the participant’s footwear.5
No mention of wedging or posting was made. When a patient has forefoot varus or a hypermobile first ray, there is an inverted forefoot–rearfoot relationship. When the device is placed on the ground without posting (intrinsic or extrinsic), the calcaneus is in an everted position and has a pronatory effect on the rear foot.
Because the molded orthoses had a pronatory effect, it can be predicted what results Baldassin would have: “… the prefabricated inserts appeared to be at least as effective in reducing the heel pain as a custom orthotic device….”
Wrobel: Double-blind trial—This podiatrist from the United States stated, in his paper:
The PFO (Orthaheel Workforce; Vionic Group LLC, San Rafael, California) contained a full foot–length, Shore C, 45-durometer, ethyl vinyl acetate, triplanar orthotic footbed with a 15-mm heel cup [.…] The device had an intrinsic 48 rearfoot medial post and was balanced through the forefoot. The manufacturer’s brushed nylon top cloth was covered by the study’s standard 3-mm neoprene top cover.9
Additionally:
A senior experienced biomechanics instructor (B.J.) with more than 20 years of teaching and practice experience performed all of the biomechanical examinations, neutral suspension castings, and CFO prescriptions. All of the patients in the CFO group received a standard prescription for functional CFOs posted with the forefoot balanced to the rearfoot deformity (neutral calcaneal stance position) with the following exceptions: 1) valgus rearfoot (neutral calcaneal stance position) received a flat rearfoot post and 2) rearfoot varus of greater than 6° was posted to a maximum of 6° varus. Medium arch fill was used for patients who could not dorsiflex past 0° and for those who were obese (30% over ideal body weight); minimum arch fill was used for all of the other patients.9
Additional accommodations were made to the prescription process, depending on body stature, foot type, first-ray function, and ankle function.
Wrobel concluded: “We found that the CFO group had a significant 125% greater improvement in spontaneous physical activity after 3 months of treatment for plantar fasciitis compared with the 22% improvement with PFOs and the 0.5% improvement with sham devices.”
Wrap-Up
In the Rasenberg meta-analysis,1 2 studies (Wrobel,7 Martin9)—each performed by first-author podiatrists from the United States—showed that a CFO provides better results than a prefabricated foot orthosis. The other 3 studies—Baldassin,5 Pfeffer,8 and Landorf6—were marked by significant insufficiencies:
- Baldassin5 did not perform a biomechanical examination, did not take a negative cast, and was not adequately trained.
- Pfeffer and associates8 were trained by watching a video for 10 minutes and 25 seconds, 17 seconds of which were devoted to the most critical part of making a proper custom orthosis (ie, a neutral position). Their inadequate training disqualifies them from making a CFO.
- Landorf6 has possible bias from an earlier paper; his study should therefore have been rejected for meta-analysis.
- My conclusion? In the United States, CFOs should be prescribed, and dispensed, only by a well-trained health professional, such as a podiatrist.
Stanley Beekman, DPM, is retired from private podiatric practice. He was Assistant Professor of Podopediatrics and, later, Assistant Professor of Sports Medicine, both in the Department of Clinical Services, Ohio College of Podiatric Medicine (now the Kent State University College of Podiatric Medicine), Kent OH. He was board certified in both podiatric orthopedics and podiatric surgery.
Disclosure: The author has had no financial ties to any podiatric laboratory for the past 36 years.
Acknowledgements: I would like to thank my mentor J. C. D’Amico and the editors of LER for helping me prepare this paper.
aOf the Department of General Practice, Erasmus Medical Center, Universitair Medisch Centrum, Rotterdam, The Netherlands.
bRegrettably, Figure 1 shows the talo-navicular joint overlying the muscle of the abductor hallucis, which brings into question the knowledge of those utilizing it.
- Rasenberg N, Riel H, Rathleff MS, Bierma-Zeinstra SMA, van Middelkoop M. Efficacy of foot orthoses for the treatment of plantar heel pain a systematic review and meta-analysis. Br J Sports Med. 2018;52(16):1040-1046.
- Weir J. Reference document: understanding claims for footwear and foot orthotics. Canadian Life and Health Insurance Association Inc Web site. January 2017. www.clhia.ca/web/CLHIA_LP4W_LND_webstation.nsf/page/7BC4EF1D20CCDFD085257A08004F6144/$file/Orthotics%20Reference%20Document%20ENG.pdf. Accessed April 9, 2020.
- Keenan A-M, Redmond AC, Horton M, Conaghan PG, Tennant A. The Foot Posture Index: Rasch analysis of a novel, foot-specific outcome measure. Arch Phys Med Rehabil. 2007;88(1):88-93.
- Orthotic fitter. American Board for Certification in Orthotics, Prosthetics & Pedorthics Web site. www.abcop.org/individual-certification/Pages/orthotic-fitter.aspx. Accessed April 7, 2020.
- Baldassin V, Gomes CR, Beraldo PS. Effectiveness of prefabricated and customized foot orthoses made from low-cost foam for noncomplicated plantar fasciitis: a randomized controlled trial. Arch Phys Med Rehabil 2009;90(4):701-706.
- Landorf KB, Keenan A-M, Herbert RD. Effectiveness of different foot orthoses to treat plantar fasciitis: a randomized trial. Arch Int Med. 2006;166:1305-1310. J Am Podiatr Med Assoc. 2004;94(6):542-549.
- Martin JE, Hosch JC, Goforth WP, Murff RT, Lynch DM, Odom RD. Mechanical treatment of plantar fasciitis. A prospective study. J Am Podiatr Med Assoc. 2001;91(2):55-62.
- Pfeffer G, Bacchetti P, Deland J, et al. Comparison of custom and prefabricated orthoses in the initial treatment of proximal plantar fasciitis. Foot Ankle Int. 1999;20(4):214-221.
- Wrobel JS, Fleischer AE, Crews RT, Jarrett B, Najafi B. A randomized controlled trial of custom foot orthoses for the treatment of plantar heel pain. J Am Podiatr Med Assoc. 2015;105:281-294.
- Rasenberg N, Fuit L, Poppe E, et al. The STAP-study: the (cost) effectiveness of custom made orthotic insoles in the treatment for plantar fasciopathy in general practice and sports medicine: design of a randomized controlled trial. BMC Musculoskelet Disord. 2016;17:31.
- Podiatry. National diploma supplement; national transcript. Study Direction Organisation of Podiatry (SROP) Web site. June 2013. www.podotherapie.nl/files/professional/opleidingen/national-transcript-podotherapie-2013-eng.pdf. Accessed April 9, 2020.
- Thomas JL, Christensen JC, Kravitz SR, et al. The diagnosis and treatment of heel pain: a clinical practice guideline—revision 2010. J Foot Ankle Surg. 2010;49(3 Suppl):S1-S19.
- Covey CJ, Mulder MD. Plantar fasciitis: how best to treat? J Fam Pract. 2013;62(9):466-471.
- Rome K, Gray J, Stewart F, Hannant SC, Callaghan D, Hubble J. Evaluating the clinical effectiveness and cost-effectiveness of foot orthoses in the treatment of plantar heel pain: a feasibility study. J Am Podiatr Med Assoc. 2004;94(3):229-238.
- Lee SY, McKeon P, Hertel J. Does the use of orthoses improve self-reported pain and function measures in patients with plantar fasciitis? A meta-analysis. Phys Ther Sport. 2009;10(1):12-18.
- Campbell JW, Inman VT. Treatment of plantar fasciitis and calcaneal spurs with the UC-BL shoe insert. Clin Orthop Relat Res. 1974;(103):57-62.
- Hawke F, Burns J, Radford JA, du Toit V. Custom-made foot orthoses for the treatment of foot pain. Cochrane Database Syst Rev. 2008;(3):CD006801.
- Hice GA. Orthotic treatment of feet having a high oblique midtarsal joint axis. J Am Podiatry Assoc. 1984;74(11):577-582.
- Petchell A, Keenan A-M, Landorf K. National clinical guidelines for podiatric foot orthoses Australasian Journal of Podiatric Medicine: AJPM.1998;32(3):97-103.
- Weil L, Jr. Clearing up the misconceptions of orthopedic surgeons over the VA Provider Equity Act. Podiatry Today. May 27, 2016. https://www.podiatrytoday.com/blogged/clearing-misconceptions-orthopedic-surgeons-over-va-provider-equity-act. Accessed April 12, 2020.





