 By Thorlene Egerton, Joanne Bolton, Camille E. Short, and Kim L. Bennell
By Thorlene Egerton, Joanne Bolton, Camille E. Short, and Kim L. Bennell
Patient education is the most commonly used intervention for chronic disease management. Education interventions have variably been shown to have benefits for chronic disease management in general and musculoskeletal pain disorders more specifically. Although impacts are modest, education interventions are accepted as an important part of multi-component behavior change interventions. Knee osteoarthritis (OA) is a highly prevalent, chronic painful condition with no cure, and recommended care focusses on education and self-management behaviors. Education is recommended as a core component of knee OA management, yet not all education is beneficial – it can do harm via the nocebo effect whereby expectation of symptom worsening is unintentionally promoted. People who are fearful of activity because of their understanding of their joint damage are less likely to engage in the very treatment that can alleviate symptoms and preserve joint functioning. Education for people with knee OA has received little research attention and little is known about the comparative impacts of different types of education.
The potential benefits of education interventions for knee OA include improvements in psychosocial outcomes, pain, function, and markers of disease. To achieve these benefits, education should not just share information about the disease process but develop a patient mindset and level of understanding that facilitates ongoing physical activity, participation and well-being. Education should aim to activate the person to self-manage through changes in behavioral determinants such as expectations, motivation and self-efficacy. Traditional patient education for people with knee OA focuses on structural damage (eg, cartilage degeneration or ‘wear and tear’) and an expectation of disease progression (eg, symptoms will progress and surgery is inevitable). This type of information is typical of education currently delivered by healthcare professionals as well as via written and online resources. This information has been shown to foster negative outcome expectation, fatalism, and activity avoidance in people with knee OA. Previous research suggests that patient education for people with musculoskeletal pain delivered with a biopsychosocial approach and messages of empowerment and positive expectation of benefit from conservative options, may be more beneficial than traditional disease information approaches. Our own qualitative study1 exploring the reactions of people with painful knee OA to a brief educational video with novel empowerment content including psychosocial components of the condition, found most participants responded favorably. Many declared an intention to add at least one effective self-management behavior. However, there was a range of responses and a small proportion reported less favorable reactions to the video. These included frustration (eg, because the information was not what they wanted to hear) and some resistance either because the information was at odds with their beliefs or advice from their doctor, or because they perceived the recommendations did not apply to their personal situation. This variability in responses warrants further exploration in order to optimize utilization of low-cost, scalable education and target enhanced education approaches.
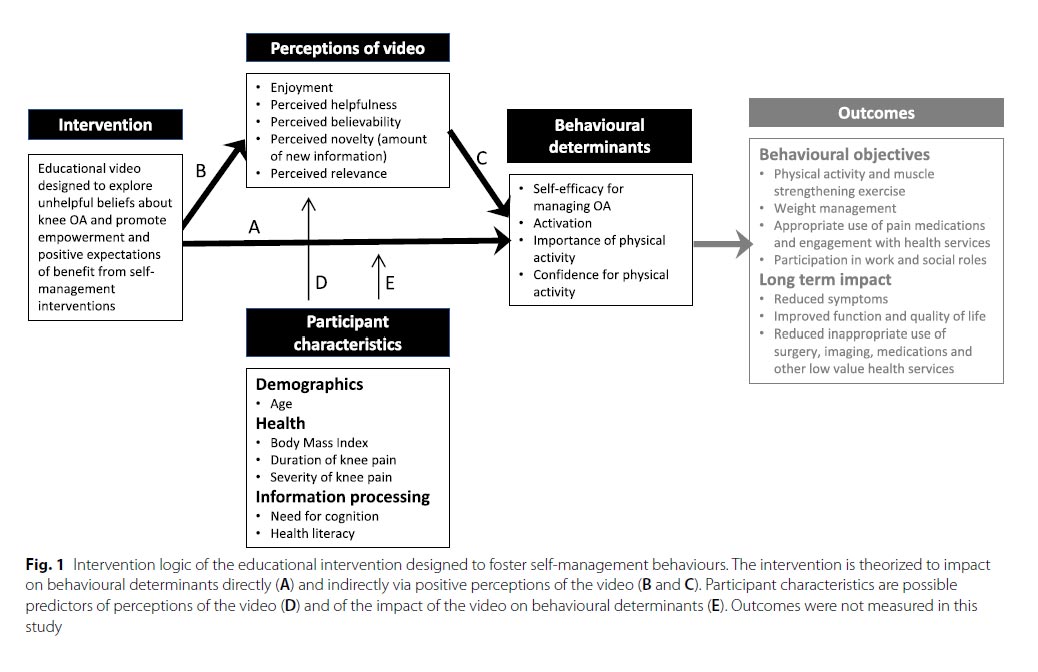 This quantitative study aimed to further explore responses to this educational video. The video utilizes presentation features and content that moves away from the more common biomedically based-education and pathoanatomical approaches to explaining and managing the disease. It avoids pictures of structural damage and does not describe severity in terms of imaging results. It was designed to communicate positive expectations about the effects of self-management behaviors with optimism for one’s future prognosis. Our rationale for how the educational video would achieve benefits for people with knee OA is depicted in the proposed intervention logic (Figure 1).
This quantitative study aimed to further explore responses to this educational video. The video utilizes presentation features and content that moves away from the more common biomedically based-education and pathoanatomical approaches to explaining and managing the disease. It avoids pictures of structural damage and does not describe severity in terms of imaging results. It was designed to communicate positive expectations about the effects of self-management behaviors with optimism for one’s future prognosis. Our rationale for how the educational video would achieve benefits for people with knee OA is depicted in the proposed intervention logic (Figure 1).
The study had three objectives. Firstly, to investigate whether the behavioral determinants targeted by the intervention (self-efficacy for managing OA, ‘activation’ i.e. attitude toward self-management, importance of physical activity, and confidence to be sufficiently physically active) changed immediately after watching the video (analysis A). The second objective was to describe viewer perceptions of the video (enjoyment, helpfulness, believability, novelty and relevance) (analysis B), and then explore whether viewer perceptions were associated with changes in behavioral determinants (analysis C). The third objective was to identify participant characteristics (age, health status and information usage attributes, i.e. health literacy and need for cognition) that were associated with viewer perceptions (analyses D) and/or changes in behavioral determinants (analysis E).
Significance
Successful adult patient education is a planned intervention, grounded in adult learning theory, with multiple components that need careful consideration. Exploring potential causal pathways explaining the effect of this novel educational intervention may help to identify characteristics that are important for educational interventions for this patient population. Since people function in complex social and physical environments and bring a range of personal attributes and health beliefs to their self-management of any health condition, understanding the participant characteristics that may indicate who will/will not benefit from this low cost, scalable education intervention may help with planning more tailored implementation strategies and optimize utilization.
Methods: Seventy-eight participants with knee OA (77% female, mean age 63.0 ± 8.7) watched the 9-min video that included evidence-based content and was designed to foster empowerment to self-manage effectively. Data were collected by online questionnaire at baseline and immediately after watching the video. Associations were tested between baseline health and information processing characteristics (health literacy, need for cognition*), perceptions of the video (enjoyment, helpfulness, believability, novelty and relevance) and pre-post changes in behavioral determinants (self-efficacy for managing arthritis, attitude to self-management or ‘activation’, and importance/confidence for physical activity). (*Need for cognition: higher score signifies greater need for cognition [which is indicative of a tendency to enjoy effortful cognitive activities].)
Results: All behavioral determinants improved immediately after watching the video (Table). Positive perceptions were associated with greater improvements in self-efficacy for arthritis (Spearman’s rho, ρ = 0.26–0.47). Greater perceived relevance was associated with increased self-rated importance of being physically active (ρ = 0.43). There were small positive associations between health literacy domains related to health information and positive viewer perceptions of the video. People with higher need for cognition may achieve greater improvement in confidence to be physically active (ρ = 0.27).
Conclusion
This study adds further support that positively framed video information about knee OA with an emphasis on empowerment for self-managing with physical activity and exercise may be beneficial. Findings are suggestive, though not conclusive, that short term benefits may include improvements in self-efficacy, activation, and motivation/confidence to be physically active. The video investigated in this study appears to be slightly better received by people with higher health literacy and higher need for cognition, as these characteristics were associated with more positive perceptions of the video and greater increase in confidence for physical activity respectively. Further research is needed to confirm these findings, but it is recommended that designers of empowerment education for people with knee OA strive to engage those with lower health literacy and lower need for cognition. Our findings also suggest that education interventions that are enjoyable and perceived to be helpful, and relevant to the individual may have greater effect. Thus, efforts by health professionals to help people with knee OA to perceive the information is being relevant to them personally may optimize the potential for the video to increase motivation and confidence to be physically active.
Reference
- Egerton T, McLachlan L, Graham B, Bolton J, Setchell J, Short CE, et al. How do people with knee pain from osteoarthritis respond to a brief video delivering empowering education about the condition and its management? Patient Educ Couns. 2021;104(8):2018–27.
This article has been excerpted from “Exploring changes, and factors associated with changes, in behavioural determinants from a low-cost, scalable education intervention bout knee osteoarthritis: An observational cohort study,” by the authors listed above. BMC Musculoskeletal Disorders. 2021;22:862. https://doi.org/10.1186/s12891-021-04751-2. Tables have been renumbered and references have been removed for brevity. Use is per Creative Commons License CC BY 4.0.





