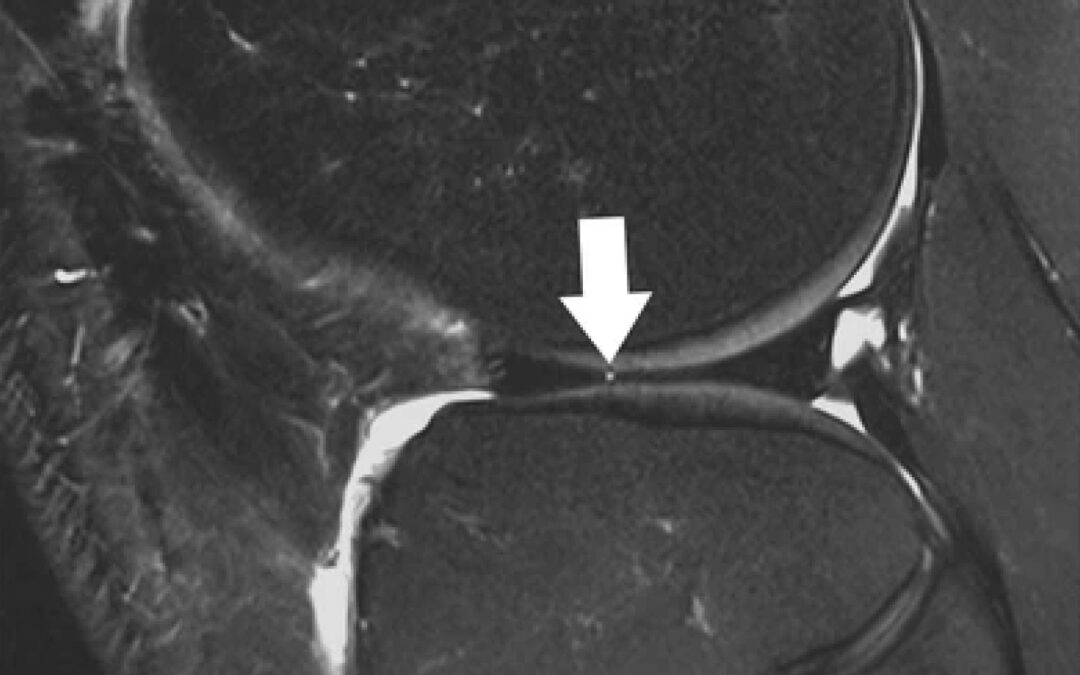
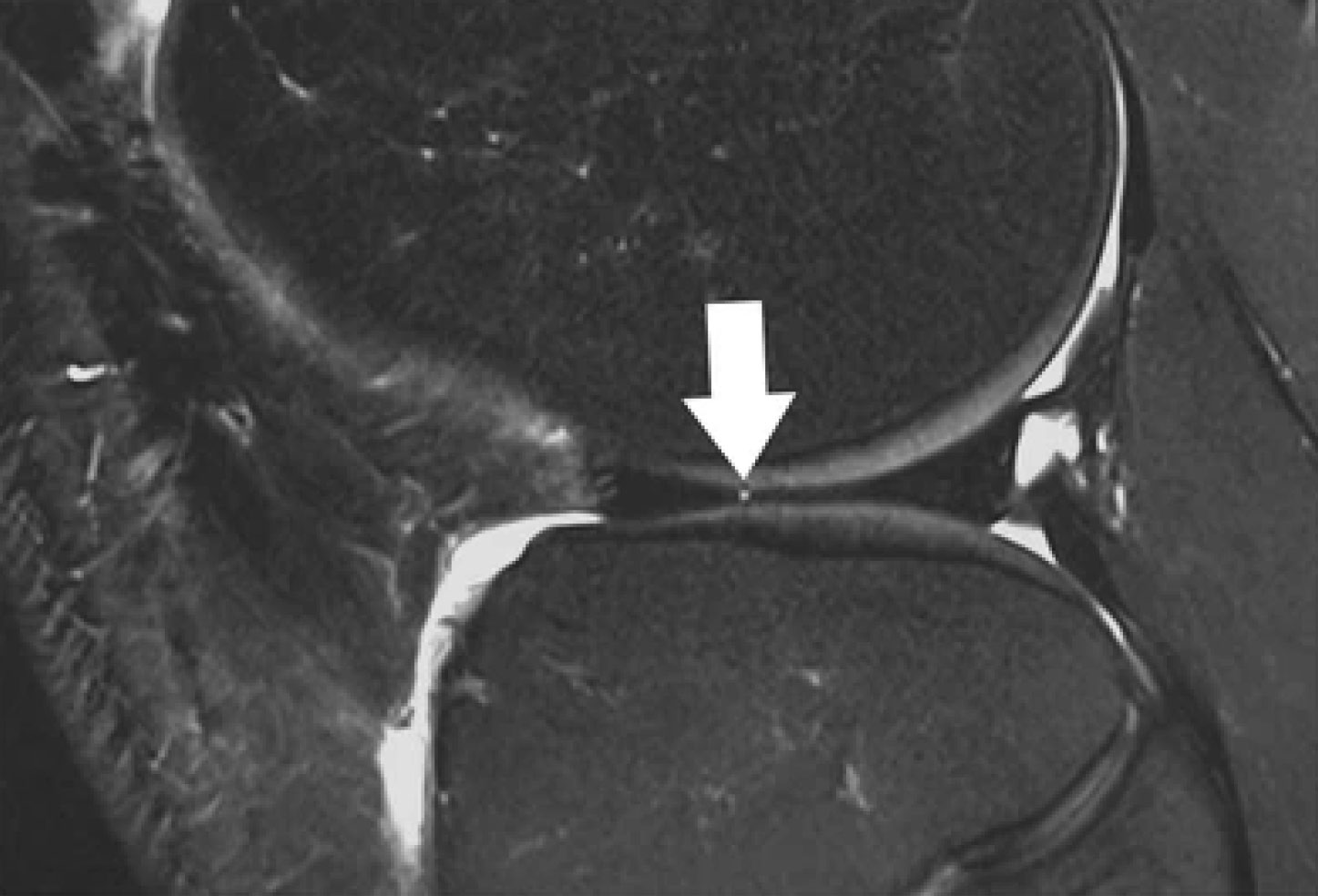
Sagittal T2-weighted, fat-suppressed fast spin echo image of the right knee in a 39-year-old male patient acquired at 3 Tesla (Siemens Healthcare, Erlangen, Germany) using a dedicated 28 channel transmit-receive knee coil shows a small radial tear of the lateral meniscus (arrow). Reprinted from Bolog NV, Andreisek G. Reporting knee meniscal tears: technical aspects, typical pitfalls and how to avoid them. Insights Imaging 2016;7:385–398. https://doi.org/10.1007/s13244-016-0472-y. Use is per Creative Commons Attribution 4.0 International License.
In releasing its new clinical practice guideline (CPG) focused on acute isolated meniscal pathology, the American Academy of Orthopaedic Surgeons (AAOS) sought to help the medical community treat patients suspected of or diagnosed with an acute isolated meniscal tear.
Acute isolated meniscal tears often occur from a traumatic injury with rotation and flexion of the knee or direct impact. While it can happen to anyone, many acute isolated meniscal tears occur in a young active population, specifically high school and college athletes. Meniscal injuries can have a significant physical and emotional impact as patients need to take time off from work or school. For athletes, return to sport may take up to 4-7 months post-surgery.
“Treating acute meniscal tears is still an evolving area and compared to other guidelines that detail recommendations for the treatment of various musculoskeletal issues, the body of evidence surrounding this injury is relatively lacking,” said Robert Brophy, MD, FAAOS, co-chair of the guideline development group. “While acute meniscal tears are common, there is more heterogeneity in terms of the injury, the pattern associated with the injury, and treatments, making it a more difficult area to study. This new [guideline] is a first step toward establishing guidelines and laying the foundation for developing a higher level of evidence to inform future recommendations.”
New Diagnosis and Treatment Recommendations
The new guideline resulted in one strong and two moderate recommendations pertaining to the diagnosis and management of patients with acute meniscal injury. The guidance is not intended for patients with concurrent ligament issues like anterior cruciate ligament tears, nor is it appropriate for those suspected of chronic or degenerative meniscal tears. The CPG includes:
- A strong recommendation stating that magnetic resonance imaging (MRI) is the preferred imaging modality to diagnose acute meniscal tears because of its high accuracy, while computerized tomography (CT) arthrography or ultrasound can be used, particularly when MRI is not available or is contraindicated.
- A moderate recommendation that a physical examination, including joint line tenderness, the McMurray test and the Thessaly test, can effectively diagnose acute meniscal tears and may yield more accurate results when combined.
- A moderate recommendation that when indicated in the treatment of acute meniscal tear, surgery should preserve as much functional meniscal tissue as possible to mitigate patient risk for osteoarthritis, underscoring the importance of trying to preserve the meniscus to delay or prevent advancement of joint degeneration.
The guideline workgroup formulated 6 options for physicians and patients to consider. Options are used when there is little, conflicting, or no evidence. Highlights of the options include:
- A limited strength option states that patients with an acute meniscal tear who have failed conservative nonoperative treatment such as physical therapy may have better outcomes from surgical intervention within 6 months of injury.
- It is the consensus of the workgroup that patients with a displaced or displacing acute meniscal tear, particularly those restricting knee range of motion, can benefit from acute surgical intervention. The workgroup also advises that patients with a symptomatic acute meniscal tear who could benefit from a repair should be considered for early surgical intervention as it could optimize the likelihood for success.
- A limited strength option states that meniscus repair can improve patient outcomes compared to partial meniscectomy in acute isolated meniscal tears with healing potential.
- Biological enhancements, specifically bone marrow venting or platelet-rich plasma, received a limited strength option as a consideration to improve outcomes in patients undergoing surgical repair of acute isolated meniscal tears.
- Based on the workgroup’s clinical opinion, physical therapy/rehabilitation may be beneficial to patients who present with an acute non-displaced isolated meniscal tear not amenable to repair when implemented as a non-operative treatment option as well as for those recovering from meniscal surgery.
“There’s no doubt physical therapy is an integral part of the treatment algorithm for people with acute meniscal tears,” said Brophy. “Whether you’re trying to avoid surgery, planning on not doing surgery, or decide to do surgery, there will likely be a role for physical therapy as part of the treatment or recovery process.”
While the study of acute meniscal tears is complex, physicians and patients now have a starting point to weigh the pros and cons to make informed decisions.
“It is important to understand that this [clinical practice guideline] is a guide, not a prescription,” said Brophy. “However, this can help patients make an informed decision with their surgeon regarding optimal treatment for their injury.”
Development of this guideline was a collaborative effort between representatives from the American Academy of the Physical Medicine and Rehabilitation; the National Athletic Trainers’ Association; the American Orthopaedic Society for Sports Medicine, the American Physical Therapy Association; the Pediatric Orthopaedic Society of North America; and the American Medical Society for Sports Medicine.
To read the complete guideline, visit https://www.aaos.org/globalassets/quality-and-practice-resources/acute-meniscal-pathology/amp-cpg.pdf.
Source: American Academy of Orthopaedic Surgeons Management of Acute Meniscal Pathology Evidence-Based Clinical Practice Guideline. aaos.org/ampcpg. Published June 10, 2024.





