
By Sang Heon Lee, Sung Hwan Kim, Kyung Bum Kim, Ho Sung Kim, and Young Koo Lee
Diabetic foot is defined as a foot affected by ulceration that is associated with neuropathy and/or peripheral arterial disease of the lower limb in a patient with diabetes. These authors focused on nutrition as a source of healing and examined the correlation between various trace elements and wound healing in patients with diabetic foot ulcers.

Diabetic foot ulcers based on Brodsky’s classification. Grade 0 has no sign of ulceration, but persistent pain is present. Grade 1 is a superficial ulcer. Grade 2 indicates deep ulceration toward the bone. Grade 3 means exposure to severe infection (osteomyelitis). Grade A has no ischemia. Grade B indicates ischemia but no gangrene. Grades C and D are partial and complete gangrene infections with ischemia, respectively. Reprinted from Appl. Sci. 2022;12:11777. https://doi.org/10.3390/app12221177 7.
Diabetic foot stands out as one of the most consequential and devastating complications of diabetes. Many factors, including VIPS (Vascular management, Infection management, Pressure relief, and Source of healing), influence the prognosis and treatment of diabetic foot patients. There are many studies on VIPS, but relatively few studies on “sources of healing.” Nutrients that affect wound healing are known, but objective data in diabetic foot patients are insufficient. We hypothesized that “sources of healing” would have many effects on wound healing. The purpose of this study is to know the affecting factors related to the source of healing for diabetic foot patients.
Methods
A retrospective review identified 46 consecutive patients who were admitted for diabetic foot management from July 2019 to April 2021 at our department. The wound size was measured manually using a ruler in operation rooms. Several laboratory tests were performed for influencing factor evaluation. We checked serum levels of total protein, albumin, vitamin B, iron, zinc, magnesium (Mg), copper (Cu), hemoglobin (Hb), HbA1c, high-density lipoprotein (HDL) cholesterol, and low-density lipoprotein (LDL) cholesterol. These values of diabetic foot patients were compared with normal values. Patients were divided into 2 groups based on wound healing rate, age, length of hospital stay, and sex, and the test values between the groups were compared.
Results & Discussion
The wound healing rate was measured using the initial wound size and the change of the wound size after 1 week of treatment. Wound healing rate (%) = [(Initial wound size − wound size after 1 week)/Initial wound size] × 100. The wound healing rate was divided into 2 groups based on a 20% threshold and the differences were compared in 2 groups. There were no differences in demographic characteristics based on wound-healing rate. There was no significant difference in age, American Orthopedic Foot and Ankle Society score, visual analog scale (VAS) score, or length of stay between the 2 groups.
The facts learned from this study are that levels of albumin (37%) and Hb (89%) were low in the diabetic foot patients; as for trace elements, levels of iron (97%) and zinc (95%) were low in these patients, but levels of magnesium and copper were usually normal or high. However, when compared to normal adult values, diabetic foot patients in our data exhibited significantly lower levels of Hb, total protein, albumin, iron, zinc, Cu, and HDL cholesterol. When compared based on age and length of hospital stay, hemoglobin levels were significantly lower in both the older age group and the group with longer hospital stays. Glycemic control, as indicated by the mean HbA1c of 7.90 (7.46, 8.35), was generally poor, which is not unexpected. The Table details average values of diabetic foot ulcer patients and comparison with normal values.
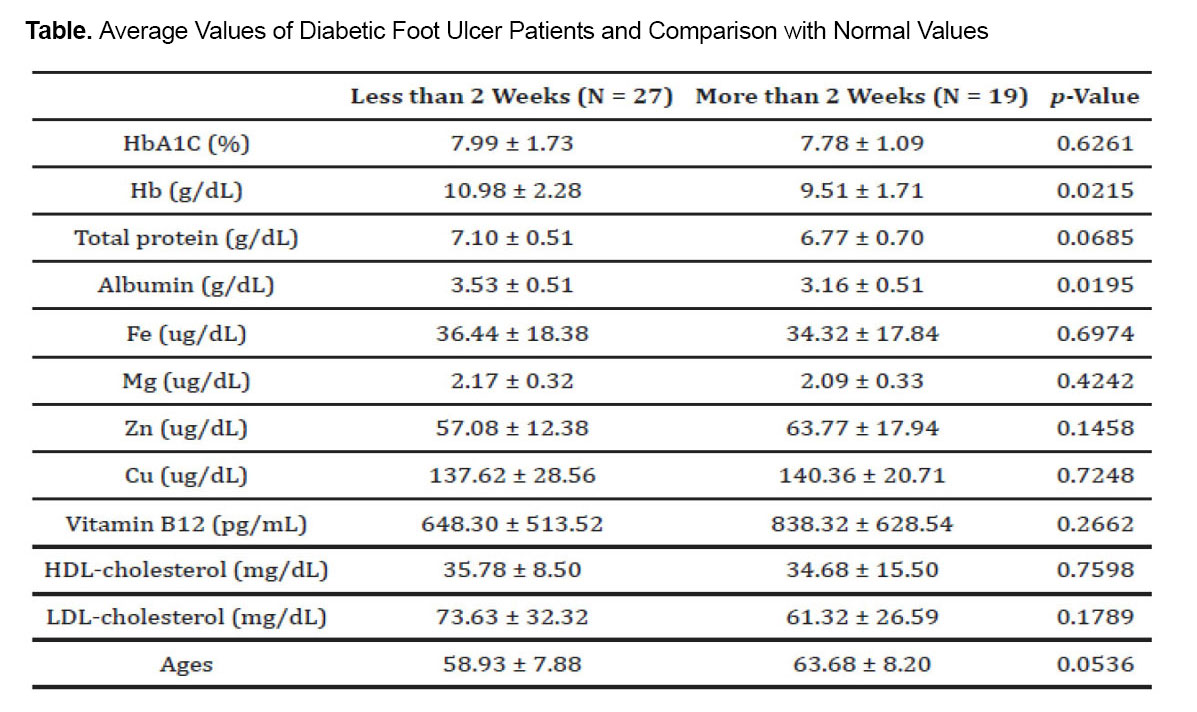
Less than 2 Weeks = Wound healing rate ≤20% (normal); More than 2 Weeks = Wound healing rate >20%.
While hypoglycemia has been linked to vascular complications in diabetes, the majority of the literature, including this section, concentrates on the adverse impacts of hyperglycemia in relation to the onset and advancement of diabetic foot ulcers. Hyperglycemia plays a role in the development of atherosclerosis, which in turn impedes the delivery of essential nutrients to wounds, thereby hindering the healing process. Additionally, in individuals with diabetes, hyperglycemia has been identified as a potential factor leading to dysfunction of endothelial cells, which are essential for the healing of diabetic foot ulcers through pressure-induced vasodilation, a response that typically serves as a protective mechanism for the skin. In addition to endothelial cells, hyperglycemia disturbs essential mechanisms crucial for re-epithelialization, such as the synthesis of proteins, migration, and proliferation of keratinocytes and fibroblasts. Another way in which hyperglycemia hampers wound healing is through the generation of free radicals due to decreased activity of antioxidant enzymes such as glutathione peroxidase and superoxide dismutase. This could partly elucidate why other research has indicated that prolonged uncontrolled hyperglycemia correlates with elevated levels of markers related to the skin-aging process, specifically advanced glycation end products (AGEs) and their receptors. Hyperglycemia can also induce the production of reactive oxygen species (ROS) through pathways including polyol, hexosamine, protein kinase C, and advanced glycation end products (AGEs). While reactive oxygen species are necessary for the initial phases of wound healing, an imbalance in their production has been demonstrated to be detrimental to the later stages of the healing process. In particular, heightened levels of reactive oxygen species can inflict damage on the blood supply, metabolism, and structure of peripheral nerves. This damage to nerves can result in sensory, motor, and/or autonomic dysfunction, with each impairment independently elevating the risk of developing a diabetic foot ulcer. Collectively, these alterations induced by uncontrolled hyperglycemia render the skin more vulnerable to injury and infection, thereby impairing the process of wound healing.
Anemia has been reported as a complication of DM and is associated with poor wound healing, amputation, and increased mortality. Recent studies have shown that anemia is prevalent among patients with DM, particularly in those with diabetic foot ulcers. A meta-analysis revealed that the severity of anemia was positively correlated with the severity of diabetic foot ulcers and could potentially serve as a predictor of amputation and mortality. Retrospective cohort studies, including research on 654 and 353 patients with diabetic foot ulcers, have identified anemia as significantly associated with larger, deeper ulcers, more severe infections, higher risk of amputation, and increased mortality rates, In the present study, hemoglobin (Hb) levels were significantly lower in diabetic foot patients compared to healthy individuals, particularly among those over 60 years of age and those hospitalized for 2 weeks or more. Addressing anemia will be crucial for promoting wound healing in diabetic foot patients. In this study, iron levels were significantly lowered in DM foot patients compared to healthy people. Iron supply will be important for the treatment of iron deficiency anemia, the main cause of anemia.
Albumin has the ability to maintain the function of endothelial cells. Albumin also improves microcirculatory blood flow and reduces inflammation and oxidative damage. Hypoalbuminemia is a risk factor for wound healing in diabetic foot ulcers. Recent studies of patients with a diabetic foot ulcer showed that serum albumin levels were significantly lower than that in diabetic patients without a diabetic foot ulcer and that low albumin level was an independent predictor for delayed wound healing. Similarly, in this study, albumin levels were significantly lowered in DM foot patients compared to healthy people. Also, the albumin level was measured to be low in patients who were hospitalized for more than 2 weeks. For wound healing, it is thought that albumin level correction and nutrition supply are important.
Magnesium plays an important role in carbohydrate metabolism as a cofactor of enzymes needed for the phosphorylation of glucose and is also required for glucose transport. Low intracellular levels negatively affect tyrosine kinase activity, glucose transport in cells, and post-receptor insulin action, which, in turn, accentuates hyperglycemia. Reza Razzaghi et al, in their randomized, double-blind, placebo-controlled trial, observed significant benefits in the reduction of ulcer length, width, and depth with Mg supplements for a period of 12 weeks in diabetic foot ulcer patients. A study by Martha Rodríguez-Morán et al showed a strong relationship between hypomagnesemia and foot ulcers in subjects with type 2 diabetes. Magnesium, which was thought to affect wound healing in previous studies, did not differ between the DM foot patients and healthy people in this study.
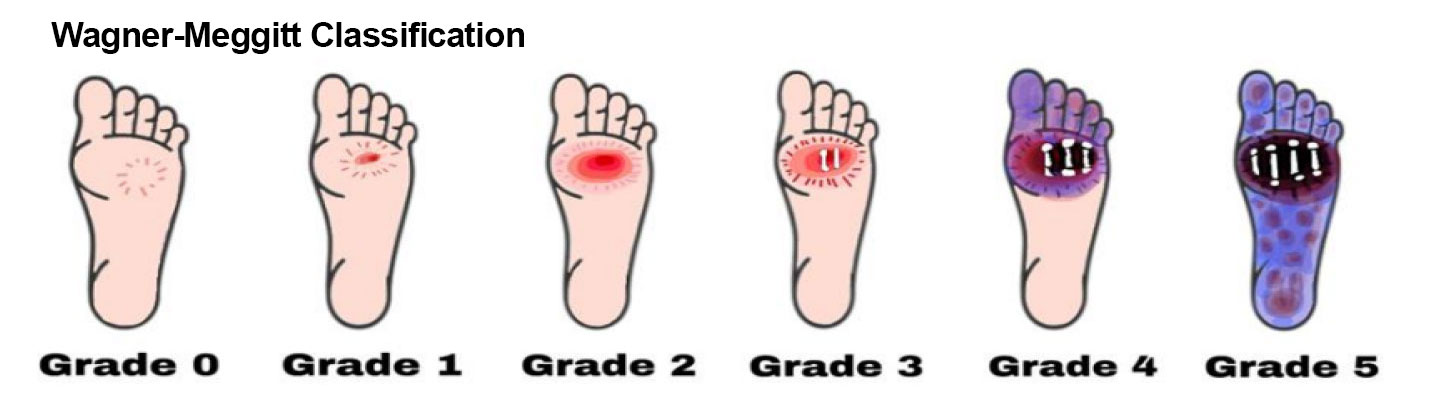
Diabetic foot ulcers are categorized using the Wagner–Meggitt classification. Grade 0 means no break in the skin. Grade 1 indicates a superficial ulcer. Grade 2 indicates a deep ulcer. Grade 3 shows the presence of osteomyelitis. Grade 4 is identified as forefoot gangrene. Grade 5 is recognized as complete foot exposure to gangrene. Reprinted from Ansari et al. Appl. Sci. 2022;12:11777. https://doi.org/10.3390/app12221177 7.
Zinc (Zn) is involved in insulin secretion, transport and receptor sensitivity, protection against free radicals, and as a cofactor for enzymes of wound healing. Zinc is the second most abundant trace element in the human body after iron, and its primary sources include animal products and seafood. It is an essential trace element vital for the function of over 300 enzymes and plays a critical role in cellular processes such as cell division and apoptosis. Zinc plays a crucial role in wound healing as it acts as a cofactor in various transcription factors and enzyme systems, including zinc-dependent matrix metalloproteinases. Matrix metalloproteinases constitute a group of calcium-dependent zinc-containing enzymes responsible for degrading the extracellular matrix.
Metalloproteinases and their inhibitors play a crucial role in regulating the degradation and deposition of the extracellular matrix during wound repair. Mansooreh Momen-Heravi et al, in their randomized, double-blinded, placebo-controlled trial, observed significant benefits in the reduction of ulcer length and width with zinc supplements for a period of 12 weeks in diabetic foot ulcer patients. The Charu Yadav et al study showed a statistically significant decrease in the serum levels of zinc in diabetic foot ulcer cases as compared with subjects without ulcers. As with other previous studies, in this study, zinc levels were significantly lowered in DM foot patients compared to healthy people.
Copper is essential for the crosslinking of elastin and collagen and mediates angiogenesis via the induction of pro-angiogenic factors, with innate immunity and protection against free radicals. It plays a crucial role in skin regeneration and the formation of new blood vessels, accelerating the healing process by stimulating the production of vascular endothelial growth factor (VEGF) and angiogenesis via the action of hypoxia-inducible factor 1-alpha (HIF-1α). Charu Yadav et al noticed a significant decrease in the serum levels of Cu in the diabetic foot ulcer group. However, in this study, Cu in DM foot patients was significantly higher than in healthy people.
Vitamin B12, also known as cobalamin, is a vitamin essential to the proper functioning and development of the central and peripheral nervous systems, ensuring effective nerve-impulse transmission. The Mohammed Badedi et al study showed that vitamin B12 deficiency was associated with diabetic foot ulcer development in patients with Type 2 Diabetes Mellitus (T2DM) in Jazan, Saudi Arabia. However, in this study, there was no significant difference in vitamin B12 levels in DM foot patients compared with healthy people.

Diagrammatic synopsis of the etiology of diabetic foot ulcers involving prolonged hyperglycemia, diabetic peripheral neuropathy, and peripheral arterial diseases. The sustained hyperglycemia impairs the wound-healing process via collagen crosslinking disorder, cell defense disorders, decreased inflammatory response, and disrupted angiogenesis; peripheral neuropathy affects the sensory, motor, and autonomic nervous systems, causing protective sensation loss, bone deformation, dry skin, skin fissures, and infections; peripheral arterial diseases such as ischemia, inflammation in lower limb microcirculation, and high plantar pressure in the foot can occur from atherosclerosis and elevated oxidative stress. Reprinted from Ansari et al. Appl. Sci. 2022;12:11777. https://doi.org/10.3390/app12221177 7.
High-density lipoproteins (HDL) are circulating particles composed of phospholipids, cholesterol, and proteins. HDL has attracted lots of attention mainly because of its protective effect against the development of atherosclerosis. Lower levels of HDL cholesterol were associated with increased risk for foot ulceration in patients with diabetes (odds ratio 0.427, 95% confidence interval [CI] 0.228–0.799, P = 0.008). No significant associations were found between diabetic foot and LDL cholesterol. In this study, HDL cholesterol was significantly lowered in DM foot patients compared to healthy people. In the case of LDL cholesterol, there was no difference in DM foot patients compared with healthy people.
Study limitations include: single institution, limited sample size, and lack of long-term research on the effects of trace elements. Based on the results of this study, it was found that trace elements can affect diabetic foot ulcers, and additional research is needed on this.
Conclusion
Compared with healthy foot patients, the levels of albumin, Hb, iron, and zinc were low in diabetic foot ulcer patients in our study. In the prognostic assessment and treatment of diabetic foot ulcers, the VIPS classification, which emphasizes vascular, infection, and pressure, as well as nutrition and trace elements as a source of healing, is crucial. Low levels of these parameters can negatively impact wound healing; thus, correction should be considered in the treatment of diabetic foot ulcers.
Authors Sang Heon Lee, Sung Hwan Kim, Ho Sung Kim, and Young Koo Lee are with the Department of Orthopaedic Surgery at the Soonchunhyang University Hospital Bucheon, Gyeonggi-do, Republic of Korea.
Author Kyung Bum Kim is with the Department of Orthopaedic Surgery at the NEW Korea Hospital, in Gyeonggi-do, Republic of Korea.

This article has been excerpted from “Factors Influencing Wound Healing in Diabetic Foot Patients” by same authors as published in Medicina (Kaunas). 2024; 27;60(5):723. doi: 10.3390/medicina60050723. Editing has occurred, including the removal and renumbering of tables and figures, and references have been removed for brevity. Figures are reprinted from Ansari P, Akther S, Khan JT, et al. Hyperglycaemia-Linked Diabetic Foot Complications and Their Management using Conventional and Alternative Therapies. Appl. Sci. 2022;12:11777. https://doi.org/10.3390/app12221177 7. Use is per CC Attribution 4.0 International License.





