
By Alex Rizzato, Matteo Bozzato, Luca Rotundo, Giuseppe Zullo, Giuseppe De Vito, Antonio Paoli, and Giuseppe Marcolin
Posterior malleolus fractures have been associated with ankle instability because the ligament pull that follows such fractures can lead to movement of the fracture fragment and consequently disrupt the weight-bearing surface’s integrity.
 Falls are a multifactorial phenomenon and a cause of increasing rates of mortality and morbidity in older adults, and are significant contributors to disability or early institutionalization. An age-dependent decrease in postural balance control and a progressive loss of lower limb muscle strength have been addressed as crucial causes of the risk of falling. A growing amount of evidence has contended that a multidisciplinary approach is required to lower the incidence and consequences of falls, also outside geriatric contexts, and that falls in older adults can be prevented with appropriately tailored exercise programs.
Falls are a multifactorial phenomenon and a cause of increasing rates of mortality and morbidity in older adults, and are significant contributors to disability or early institutionalization. An age-dependent decrease in postural balance control and a progressive loss of lower limb muscle strength have been addressed as crucial causes of the risk of falling. A growing amount of evidence has contended that a multidisciplinary approach is required to lower the incidence and consequences of falls, also outside geriatric contexts, and that falls in older adults can be prevented with appropriately tailored exercise programs.
Due to their practical benefits and widespread applications, there has been growing interest in using unstable devices in training protocols. This study aimed to assess the effectiveness of 2 multimodal exercise interventions (ie, on stable and unstable surfaces) on dynamic balance control and lower limb strength in older adults.
Methods
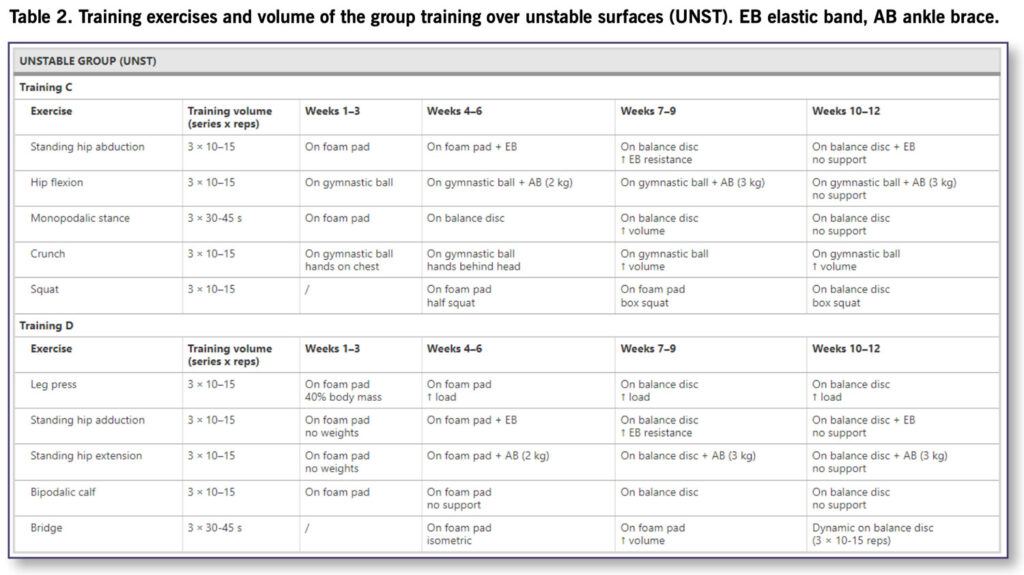
Sixty-two older adults, age 60–85 years, who were autonomous in activities of daily living, were randomly assigned to 2 intervention groups (N = 20, stable group; N = 19, unstable group), and to a control group (N = 18); 57 participants completed the study. In this single-blinded randomized controlled study, the 2 intervention groups underwent a 12-week training program twice a week for 45 minutes, consisting of strength and balance exercises. The stable (ST) group performed the training program over stable surfaces (Table 1), while the unstable (UNST) group over unstable surfaces (Table 2).
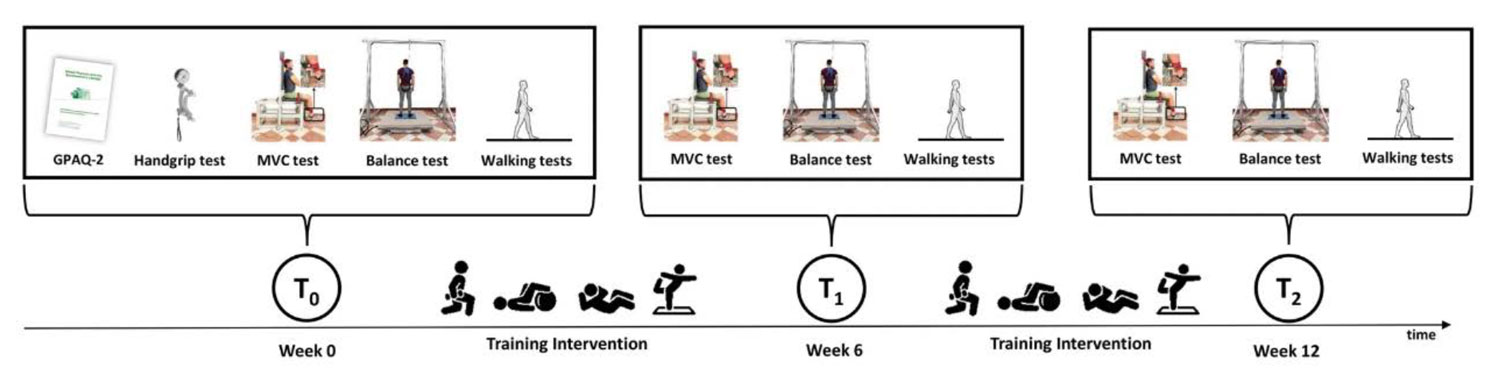
At the beginning of the study (T0), the Global Physical Activity Questionnaire (GPAQ-2) was administered to estimate the daily physical activity level, and the grip strength of the dominant hand was measured using a handgrip dynamometer. The dominant lower limb strength was evaluated in the 3 testing sessions through an isometric maximal voluntary contraction (MVC) of the quadriceps. In the Timed Up and Go (TUG) test, subjects were required to stand up from the chair, walk at the preferred pace to a cone at 3 meters, turn around, and walk back to the chair to sit down. In the 10-minute walking test, subjects were instructed to walk 20 meters at their preferred speed (Figure 1).
 Dynamic balance was assessed by computing the center of pressure (CoP) trajectory while a driven movable platform induced an unexpected perturbation of the base of support. Specifically, the study authors considered the following CoP-related parameters within a 2.5-second temporal window from the beginning of the perturbation: displacement (Area95), mean velocity (Unit Path), anterior–posterior first peak (FP), post perturbation variability (PPV), and maximal oscillations (ΔCoPMax). The dominant quadriceps strength was measured through an isometric MVC on an instrumented chair.
Dynamic balance was assessed by computing the center of pressure (CoP) trajectory while a driven movable platform induced an unexpected perturbation of the base of support. Specifically, the study authors considered the following CoP-related parameters within a 2.5-second temporal window from the beginning of the perturbation: displacement (Area95), mean velocity (Unit Path), anterior–posterior first peak (FP), post perturbation variability (PPV), and maximal oscillations (ΔCoPMax). The dominant quadriceps strength was measured through an isometric MVC on an instrumented chair.
Results
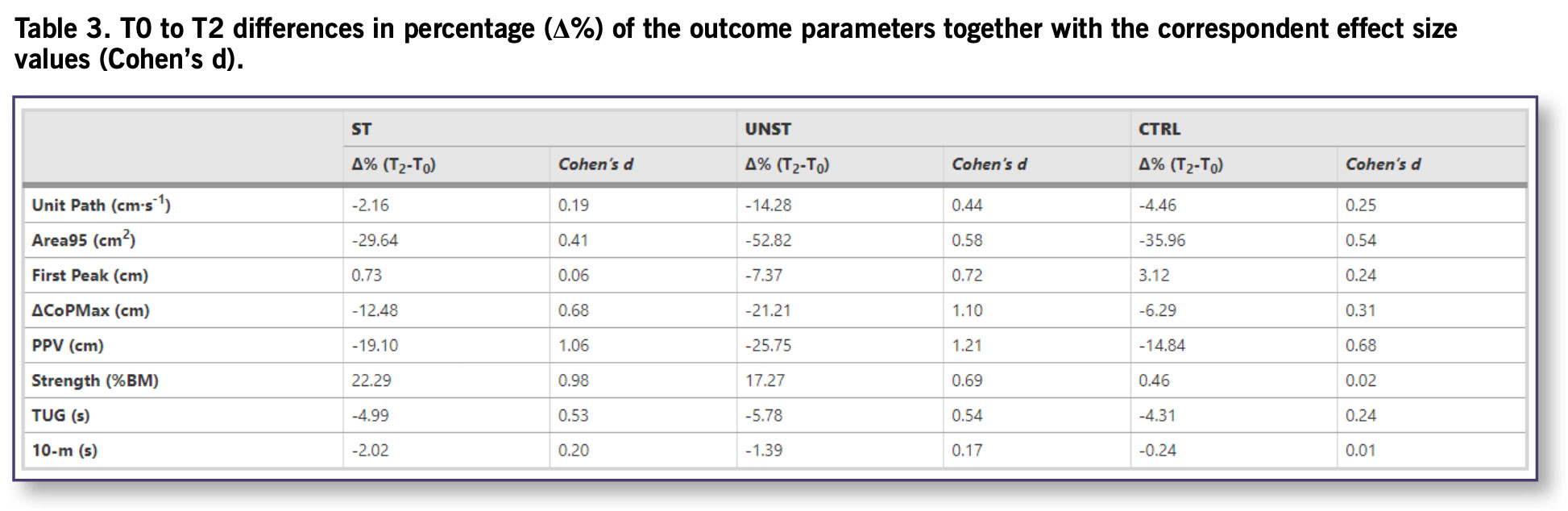
Four out of 5 CoP-related parameters (ie, Area95, Unit Path, ΔCoPMax, and PPV) significantly improved in the UNST group from a minimum of 14.28% (d = 0.44) to a maximum of 52.82% (d = 0.58). The ST group significantly improved only in 2 (ie, ΔCoPMax, and PPV) out of 5 CoP-related parameters with an enhancement of 12.48% (d = 0.68) and 19.10% (d = 1.06). Both intervention groups increased the maximal isometric quadriceps strength (UNST:17.27%, d = 0.69; ST:22.29%, d = 0.98). The control group did not show changes in any of the parameters considered.
Discussion
The present study evaluated the effectiveness of 2 multimodal interventions in older adults, different for the surface where lower limb strength and balance exercises occurred: stable and unstable surfaces for ST and UNST groups, respectively. Both exercise interventions presented in this study improved lower limb strength and dynamic balance at 12 weeks. In detail, the training on unstable surfaces highlighted a better balance performance (ie, lower values of Area95) and a higher efficiency of the postural control systems (ie, lower values of Unit Path) in coping with the external perturbations superimposed by the electrically-driven movable platform. Moreover, although the dynamic balance improvements (Table 3) in both intervention groups were significantly greater compared to the control group, effect sizes were higher in the UNST (Cohen’s d from 0.44 to 1.21) rather than in the ST (Cohen’s d from 0.06 to 1.06) group.
These findings support multimodal training on unstable surfaces as an effective choice to improve dynamic balance control in older adults. The main mechanism underpinning the overall better balance performance of the UNST group could be attributed to the stimuli the unstable surfaces gave the participants. Indeed, the induced instability could have introduced repeated changes in acting forces and unpredictable sensory inputs that highly stimulated the proprioceptive system. In this regard, the training protocol on unstable surfaces could have improved the demand on the nervous system to perceive sensory signals and generate appropriate motor commands. Conversely, the less striking improvements in dynamic balance control in the ST group could be attributable to the control mechanisms of the CoP displacement within the base of support that is related more to sensory perception than to muscle strength.
Overall, in a dynamic environment, CoP-related parameters are more sensitive than functional test outputs in the balance scoring process, reducing the risk of not highlighting training advancements. Indeed, the employment of an electrically driven movable platform and the specific CoP-related parameters represented a novelty in this longitudinal study. The FP reflects the efficacy of the earliest feet-in-place postural responses to the perturbation of the base of support and depends mainly on the spinal cord-mediated stretch reflexes with the shortest latencies (< 70 ms). The non-significant changes of FP over the 12 weeks in both ST and UNST groups could depend on the training modalities that did not include exercises with sudden unexpected perturbations. Conversely, voluntary responses have more prolonged latencies (> 150 ms) and produce highly variable motor responses. Since most of the dynamic CoP-related parameters calculated (ie, Area95, Unit Path, ΔCoPMax, and PPV) assessed postural responses with latencies longer than 150 ms, the study authors speculate that exercises of both interventions (Tables 1 and 2) trained mainly voluntary controlled mechanisms.
 Moreover, unlike previous studies, the exercises in this multimodal training programs differed completely from the dynamic balance test performed over the electrically driven movable platform. Consequently, in agreement with Bierbaum and colleagues, these findings provide indirect evidence that both multimodal training protocols produced motor and perceptive schemes useful outside of the specific training domain. It has been argued that new postural strategies may be ascribed to a shift from prefrontal activity to a subcortical circuit, accompanied by increased automatic balance performance. Considering the higher balance improvements of the UNST group, the study authors speculate that repetitive training with unstable devices could boost sensorimotor adaptations transferable to daily living postural control. Indeed, the repeated exercises proposed with the unstable training protocol enhanced balance skills not only within the same repeated exercises but also in other untrained demanding balance tasks (ie, responding to a sudden perturbation of the base of support). Hence, the multimodal training protocol over unstable surfaces could supposedly help minimize the risk of falls in older adults.
Moreover, unlike previous studies, the exercises in this multimodal training programs differed completely from the dynamic balance test performed over the electrically driven movable platform. Consequently, in agreement with Bierbaum and colleagues, these findings provide indirect evidence that both multimodal training protocols produced motor and perceptive schemes useful outside of the specific training domain. It has been argued that new postural strategies may be ascribed to a shift from prefrontal activity to a subcortical circuit, accompanied by increased automatic balance performance. Considering the higher balance improvements of the UNST group, the study authors speculate that repetitive training with unstable devices could boost sensorimotor adaptations transferable to daily living postural control. Indeed, the repeated exercises proposed with the unstable training protocol enhanced balance skills not only within the same repeated exercises but also in other untrained demanding balance tasks (ie, responding to a sudden perturbation of the base of support). Hence, the multimodal training protocol over unstable surfaces could supposedly help minimize the risk of falls in older adults.
Although the 2 interventions presented in this study were not fully oriented to increase strength, they showed improvements (Table 3) in the quadriceps isometric strength compared to the control group. After 6 weeks, the isometric strength of knee extensors significantly increased only in the ST group, which maintained this improvement until week 12. Conversely, the unstable training did not trigger a strength increase at the early stage and exhibited nearly similar increases to the stable training only at week 12. Thus, both multimodal trainings led to similar enhancement in lower limb strength over the 12 weeks. However, the different training surfaces used by the 2 intervention groups could account for the earlier strength enhancement in the ST group. Although the perceived exertion was the same for the 2 groups, strength exercises of the UNST group did not allow the same load progressions over the 12 weeks compared to the ST group (mean load: ~ -20%). Indeed, given the need for continuous adaptation to unstable surfaces, exercising with unstable devices might cause reduced force production during training. Overall, strength increments detected in UNST and ST were moderate compared to those following protocols oriented to resistance training, namely ~ 35% [41] and ~ 37% [42]. However, they were in line with increments of similar studies using multimodal exercise protocols on stable surfaces: ~ 20% [43], ~ 20% [10], and ~ 19%. Notably, the mentioned studies were performed on highly deconditioned subjects. Indeed, institutionalized older adults, considering their functional loss, could obtain more significant functional gains following multimodal training (ie, strength, mobility, and balance) compared to healthy, active older adults. Hence, the results of this study expands previous findings in deconditioned subjects, demonstrating that multimodal training protocols based on balance and strength exercises also positively affected strength in active older adults.
 Finally, although dynamic balance control and lower limb isometric strength increased after training, the functional walking tests showed no improvements during and after the training interventions. Even though these tests are valid and reliable in assessing health-related physical fitness, these findings could be explained by the ceiling effect these tests presented when applied in high-functioning older adults.
Finally, although dynamic balance control and lower limb isometric strength increased after training, the functional walking tests showed no improvements during and after the training interventions. Even though these tests are valid and reliable in assessing health-related physical fitness, these findings could be explained by the ceiling effect these tests presented when applied in high-functioning older adults.
Conclusions
The 2 multimodal training programs increased muscular strength and dynamic balance control at 12 weeks. Stable surfaces promoted faster increments of muscular strength. Unstable surfaces were more effective in enhancing dynamic balance efficiency. These findings suggested the employment of multimodal training on unstable rather than stable surfaces to potentially lower the incidence of falls in older adults.
Alex Rizzato, PhD, temporary researcher; Matteo Bozzato, research fellow; Luca Rotundo; Giuseppe De Vito, MD, PhD, professor of human physiology; Antonio Paoli, professor and chair of sport and exercise sciences, director of the Nutrition & Exercise Physiology Laboratory; and Giuseppe Marcolin, assistant professor, are with the Department of Biomedical Sciences, University of Padova, Italy.
Giuseppe Zullo, is a research fellow with the Department of Industrial Engineering, University of Padova, Italy.as
This article has been excerpted from “Multimodal training protocols on unstable rather than stable surfaces better improve dynamic balance ability in older adults. Eur Rev Aging Phys Act 21, 19 (2024). https://doi.org/10.1186/s11556-024-00353-8. Editing has occurred, including the renumbering or removal of tables and figures, and references have been removed for brevity. Use is per CC Attribution 4.0 International License.





