Background: Posterolateral ankle impingement typically presents as pain on the posterolateral aspect of the ankle that worsens with plantar flexion and passive or active great toe flexion. Typically, the condition is caused by repetitive low-grade trauma into plantar flexion. This is a type 3 case study on posterolateral ankle impingement in a collegiate soccer player.
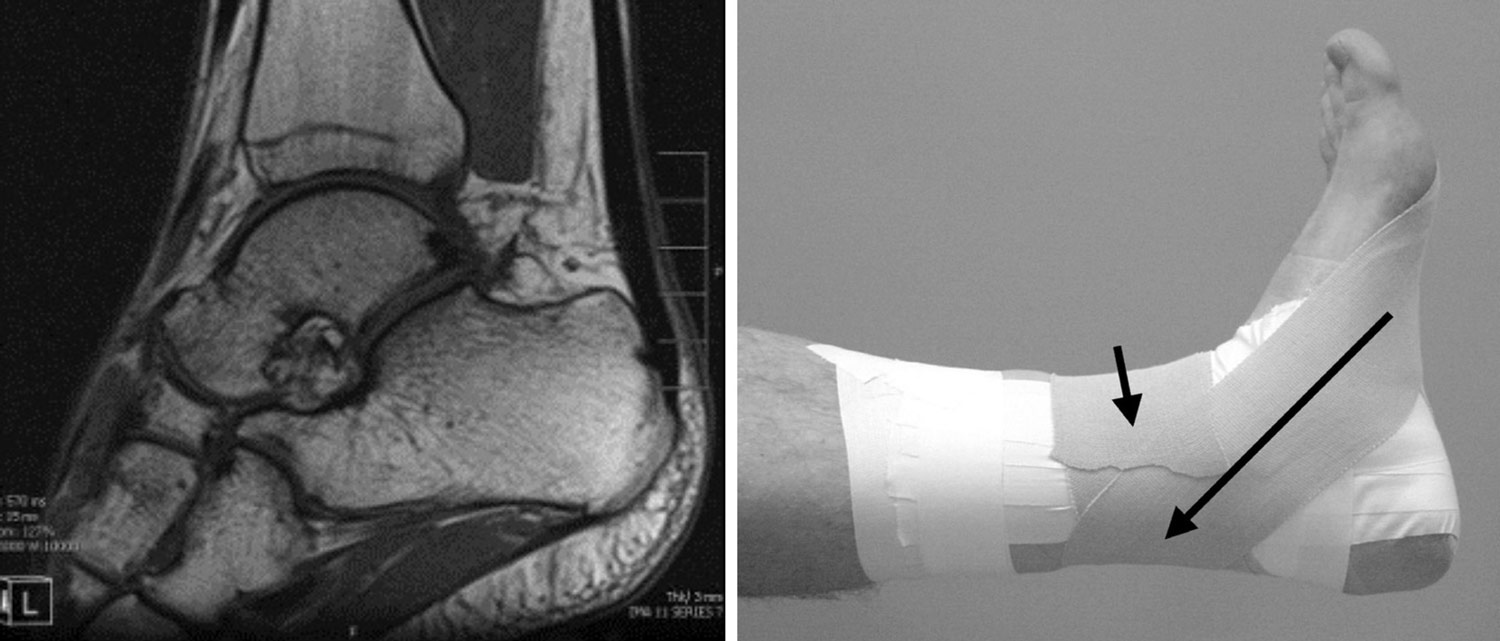
Patient: The patient is a male collegiate soccer goalkeeper diagnosed with posterolateral ankle impingement. He initially complained of anterolateral ankle pain that moved into the posterolateral aspect of his leg during the fall season of 2020. The patient had an X-ray and MRI in 2020, at which time a peroneal resection was recommended. The patient also presented with Os trigonum. The patient underwent surgery in February of 2021 and completed rehabilitation that summer. The pain persisted, however, after being released.
Intervention & Treatment: Mid-September of 2021, the patient briefly found pain relief in noxious stimulation. In October 2021, the team physician diagnosed the injury as posterolateral ankle impingement. Rehabilitation consisted of strengthening both the gluteus maximus and medius, eccentric biased calf exercises and manual strengthening of the ankle. The eccentric exercises and manual strengthening exercises were performed with silicon cups on the working muscles. Additionally, a custom tape job was designed like a talar sling in combination with a reverse Achilles to reduce any symptoms the patient may have been experiencing. The athlete was also prescribed diclofenac by the team physician for pain and inflammation.
Outcomes or Other Comparisons: Posterolateral ankle impingement is most common in dancers; however, we identified it in a soccer keeper as a result of excessive kicking. In 2018 about 27% of injuries from dance involved the ankle with over half of them being posterior ankle impingement syndrome or flexor hallucis longus tendinopathy (Rietveld et. al). The presence of Os trigonum may cause symptoms, however, the presence of the Os trigonum often remains asymptomatic.
In October 2021, the athlete opted for conservative treatment rather than surgical intervention. The athlete continued to rehabilitate through the spring of 2022. In September of 2022, the athlete decided to pursue surgery post-season to pursue a professional career but will continue conservative treatment to play in the fall of 2022 season.
Conclusions: This case of posterolateral ankle impingement presented with both anterolateral and posterolateral ankle pain and no pain with great toe flexion. Typically, there is no anterolateral ankle pain and there is also pain with passive and active great toe flexion. Treatment of previous cases typically included cortical steroid injections to continue play, whereas this case was treated with rehabilitation. There is no standardization to conservative treatment of posterolateral ankle impingement in athletes, so the rehabilitation was based on the patient’s presentation.
Clinical Bottom Line: Although not as common, posterolateral ankle impingement can occur in any athletic population, not just dancers. Through properly taping the ankle to decrease the symptoms and properly rehabilitating the injury, posterolateral ankle impingement can be treated conservatively to enable the athlete to continue to play. It is important for clinicians to understand the extent of the injury and how best to rehabilitate it to decrease the symptoms.
Source: Becker L, Stevenson P, Norkus SA: A Case of Posterior Ankle Impingement In a Collegiate Level Soccer Player: Type 3 Case Study. J Athl Train. 2023;58(6S):161. Used with permission; all rights reserved.





