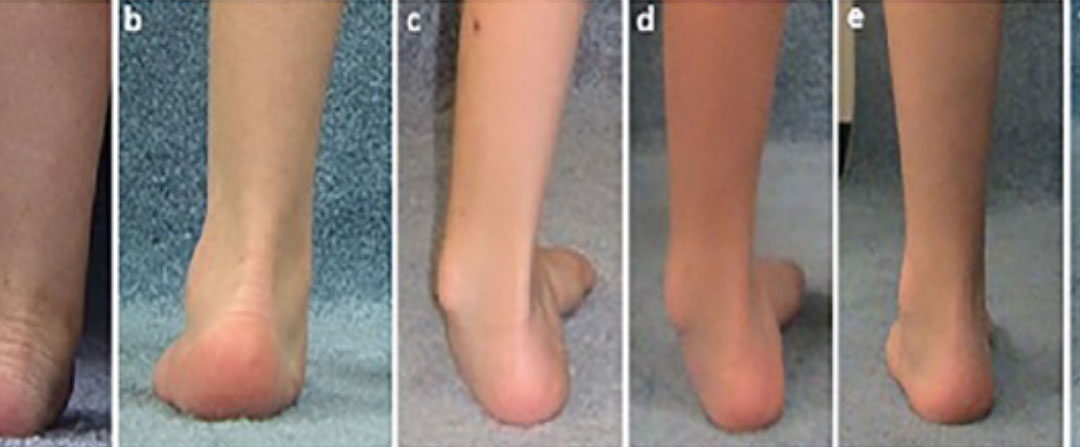

Figure. This girl presented at 2 years of age with a hemiplegic pattern, walking without external support. The main concern was (a) the severe left planovalgus foot, which was treated with a solid AFO. By age 4 years, the planovalgus was a (b) little better and the hinged AFO was continued. From age 4 to 6 years, her AFO was weaned as her foot improved, but then it continued into (c) varus. This required her to return to the AFO use until age 8 years when (d) the deformity was becoming more stiff with reduced AFO tolerance. At age 10 years, she had a gastrocnemius lengthening and a split tibialis posterior transfer. By age 14 years, she is brace-free with (e) improved foot posture, which continued to be (f) maintained with mild further improvement at age 21 years. This pattern of foot posture development from age 2 to 20 years is especially unpredictable in the younger ages.
Researchers from the Department of Orthopaedics at the Nemours Children’s Hospital Delaware (Wilmington, DE) wanted to understand the change in dynamic foot posture in children with cerebral palsy. They were able to track 33 children (54 limbs) who completed 16.9 evaluations from an initial age of 2.9 (±0.7) yrs to 18.6 (±1.7) yrs. They found that early valgus foot posture normalizes in children at Gross Motor Function Classification System levels I/II and persists in children at levels III/IV who do not have foot surgery. They concluded that foot posture in young children with cerebral palsy begins in valgus and tends to normalize in youth who walk without an assistive device. They recommend conservative management of foot deformity in early childhood for this population.
Sources: Church C, Lennon N, Lennon M, et al. Changes in foot posture evaluated with dynamic pedobarography over the course of childhood in ambulatory youth with cerebral palsy. J Child Orthop. 2024;18(1):3-12. doi: 10.1177/18632521231208746.





