
A novel EMG-triggered system syncs spinal and hip stimulation to boost gait in stroke survivors. Image courtesy of Toshiyuki Fujiwara, Juntendo University.
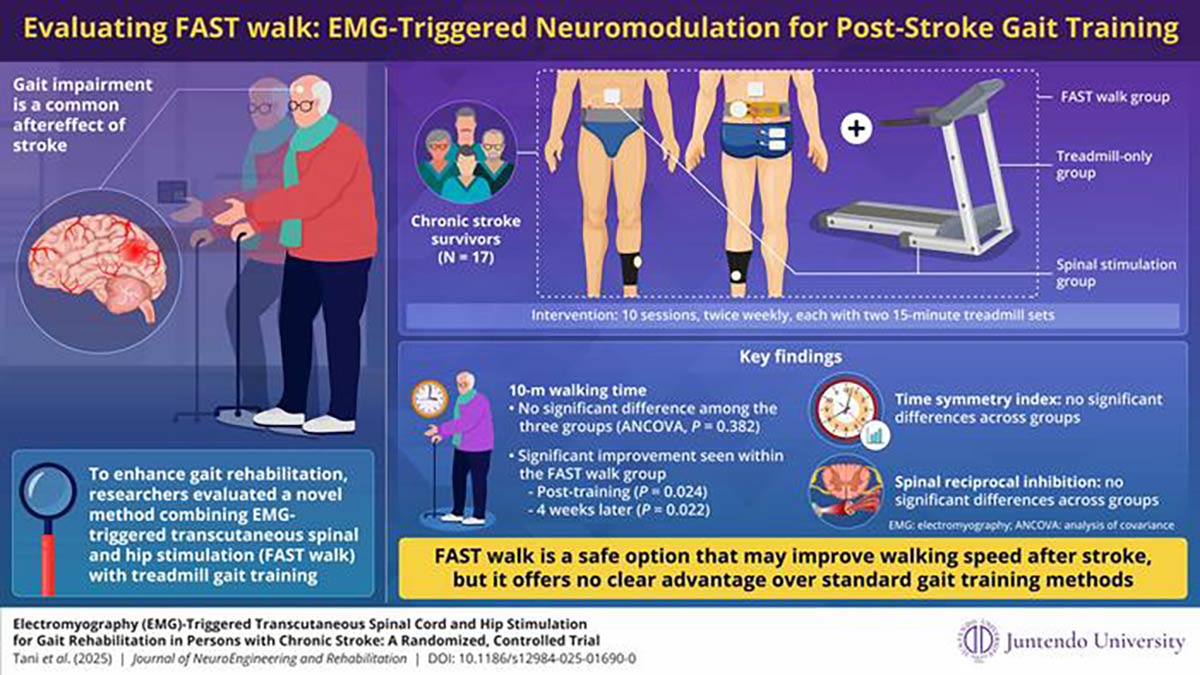
In an effort to address the ongoing challenge of gait impairment after stroke, researchers have developed an innovative rehabilitation approach known as FAST walk, an innovative, electromyography (EMG)-triggered system that synchronizes transcutaneous spinal cord stimulation with hip extensor stimulation. This dual approach uses the patient’s own muscle signals to stimulate precisely during key gait phases. By enhancing the spinal circuit excitability and activating reflexes such as the crossed extensor reflex, the system aims to improve lower-limb coordination and gait efficiency. This study was led by Professor Toshiyuki Fujiwara and Dr. Mami Tani from the Department of Rehabilitation Medicine, Juntendo University Graduate School of Medicine, Japan.
To evaluate the clinical potential, researchers conducted a randomized controlled trial involving 3 groups: FAST walk, spinal stimulation alone, and treadmill training. Each group received 2 gait training sessions per week for 5 weeks. All groups demonstrated improvements in walking speed that exceeded the minimum clinically important difference for chronic stroke (0.15 m/s). Specifically, the FAST walk group improved from 0.55 m/s to 0.70 m/s, the spinal stimulation group from 0.90 to 1.16 m/s, and the treadmill group from 0.90 to 1.09 m/s. However, only the FAST walk group showed a statistically significant improvement in gait speed within groups, suggesting that the combined stimulation may offer added benefit over either approach alone.
The study also assessed spinal reciprocal inhibition (RI) as a potential marker of neural modulation. No significant changes were observed, likely due to the measurement being done at rest rather than during gait, where phase-specific modulation would be more pronounced. The use of orthoses in some participants may have further limited voluntary ankle movement, reducing observable RI changes.
Despite these limitations, the study provides early evidence of FAST walk’s feasibility, safety, and potential efficacy. The fact that meaningful improvements were observed within a short and constrained intervention window underscores its clinical promise. While additional validation is needed, this study marks an important step forward in integrating neuromodulation into post-stroke rehabilitation.





