
 By Patrick DeHeer, DPM FACFAS, FFPM RCPS (Glasg)
By Patrick DeHeer, DPM FACFAS, FFPM RCPS (Glasg)
First metatarsophalangeal joint (MPJ) arthrodesis has been studied extensively since its inception in 1852. The procedure primarily aims to relieve pain, restore length, and stabilize the medial column of the foot. This in turn helps re-establish the foot’s weight-bearing pattern, contributing to a balanced foot tripod. Despite its long history and effectiveness, MPJ arthrodesis is not without complications, the most notable of which is non-union.
The prevalence of non-union varies with rates ranging from 6.5% to 9.2%. Key strategies to minimize this risk include appropriate plate selection—favoring longer plates—and careful consideration of the dorsiflexion angle, with a 5-degree angle often recommended. Non-union management might involve both medical approaches, such as teriparatide to boost bone healing, and surgical revisions, using techniques such as orthogonal plating and bone grafting to restore proper alignment and length of the first ray.
Benefits of First MPJ Arthrodesis
First MPJ arthrodesis is a well-established procedure with a track record of providing significant benefits for patients. Its primary aim is to alleviate pain and provide stability to the foot. Beyond pain relief, it plays an integral role in correcting foot mechanics and restoring the correct alignment of the medial column of the foot. This procedure helps reestablish a balanced weight-bearing pattern, which in turn contributes to the stabilization of the foot structure.
The primary benefit of the first MPJ arthrodesis is pain relief. Patients suffering from severe pain in the first MPJ can find significant relief after undergoing this procedure. Along with mitigating pain, it enhances the stability of the medial longitudinal column, which is essential for the overall balance and functionality of the foot. By providing a stable base, patients can experience improved mobility and function.
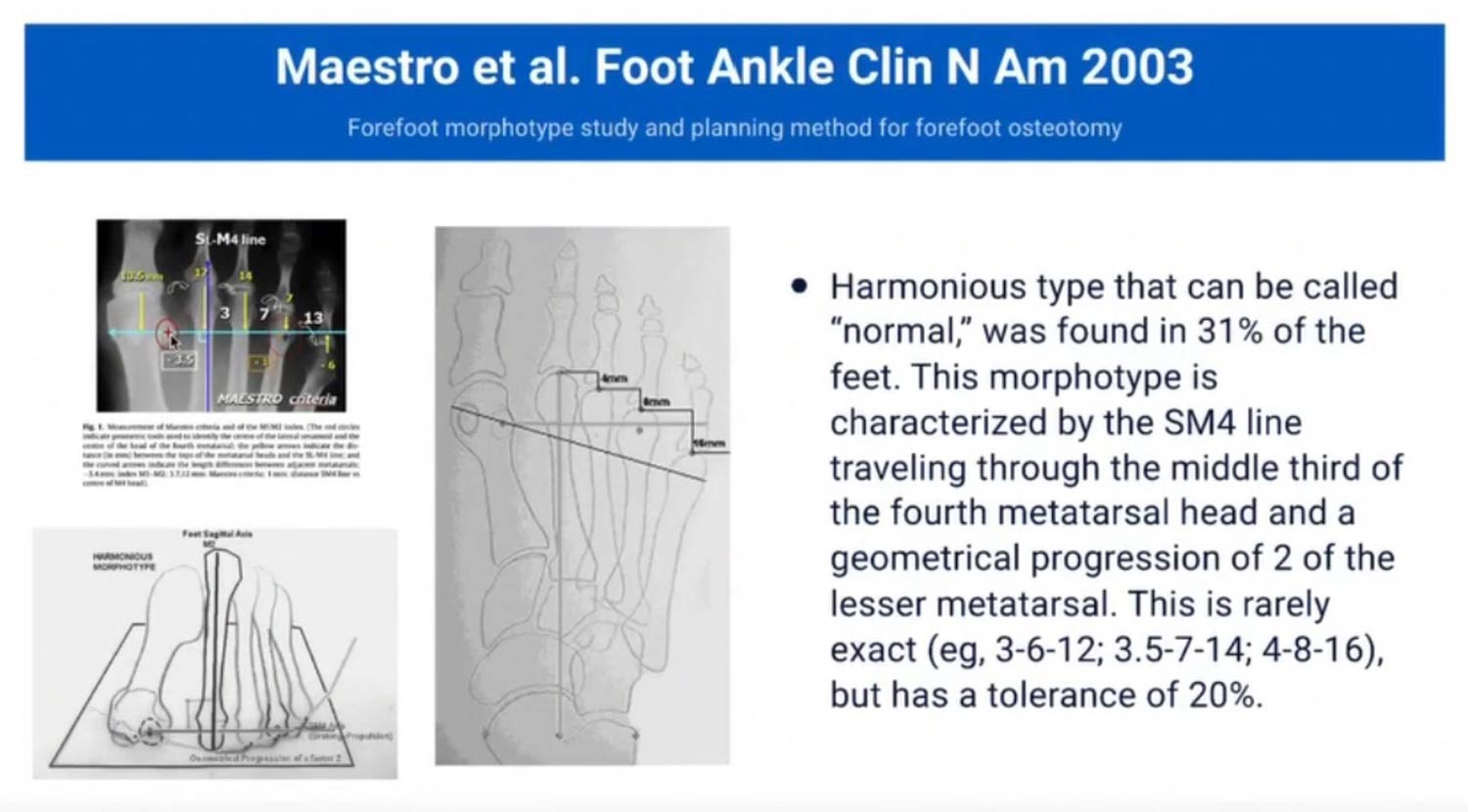
One of the critical goals of this procedure is to restore the original length of the medial column. Maintaining the proper length is vital for effective weight distribution across the foot, promoting a healthier and more balanced walking pattern. This restoration can alleviate transfer metatarsalgia, an issue stemming from uneven weight-bearing across the foot.
Non-Union Rates and Risk Factors
 Non-union is a potential complication following first MPJ arthrodesis, although it occurs in a minority of cases. Understanding the rates and risk factors associated with non-union is crucial for surgical planning and patient education.
Non-union is a potential complication following first MPJ arthrodesis, although it occurs in a minority of cases. Understanding the rates and risk factors associated with non-union is crucial for surgical planning and patient education.
Studies indicate that the non-union rate for first MPJ arthrodesis is approximately 6.5%, meaning these patients did not achieve a complete fusion of the bones post-surgery. Practitioners are advised to speak with patients realistically about potential outcomes, including a 5% to 10% chance of non-union.
Key risk factors contributing to non-union include male gender, multiple comorbidities, and severe arthritis. These factors, alongside surgical technique and hardware choice, can influence union success rates. Patients should be informed about these risks to maintain realistic expectations and enable proactive management.
The degree of dorsiflexion applied during the fusion significantly impacts the likelihood of a successful union. A dorsiflexion angle of around 5 degrees is often recommended, as it is found to reduce the load applied distally and promote better bone fusion. Conversely, zero-degree plates can increase the risk of non-union due to less optimal load distribution. Achieving the proper angle not only aids in the fusion process but also benefits foot biomechanics by enhancing arch support and promoting a proper gait. Proper angle alignment also avoids transfer metatarsalgia, which is always a potential about which patients need to be advised.
Surgical Technique Considerations
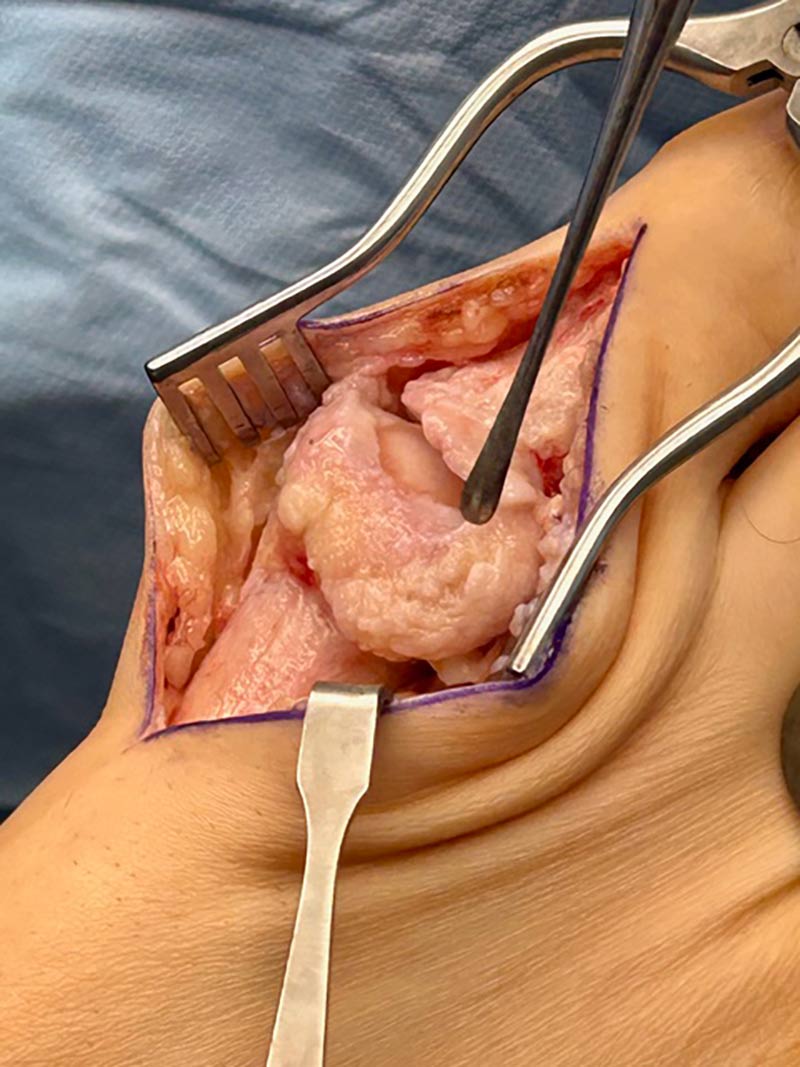
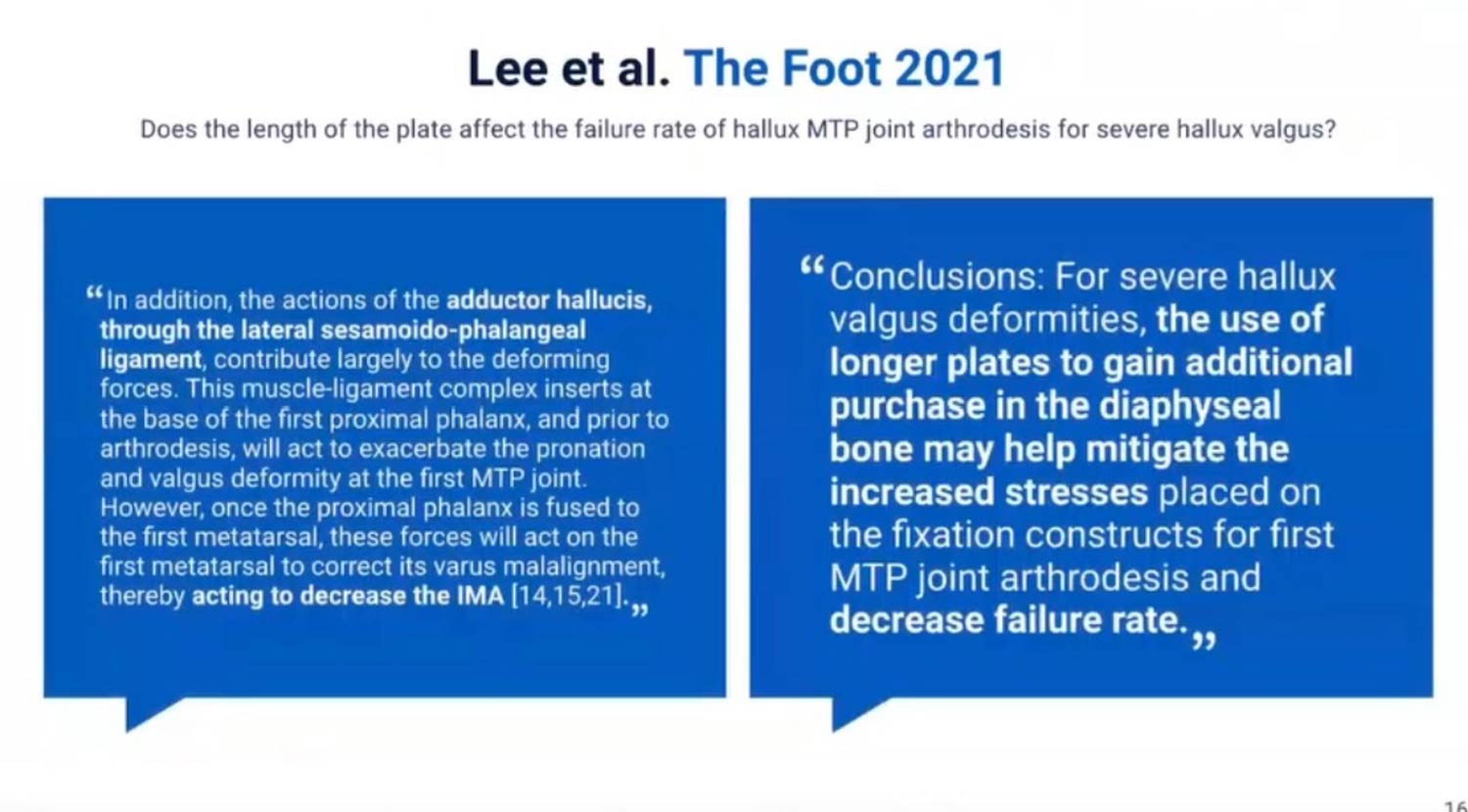 A pivotal component in first MPJ arthrodesis is the adequate preparation of the joint. Properly releasing the joint ensures successful fusion by minimizing non-union risks. Essential steps include the thorough release of the adductor hallucis and sesamoidal-phalangeal ligament. By accessing these structures, surgeons can effectively prepare the joint, ensuring the best chance for a successful outcome. This preparation also plays a crucial role in achieving correct alignment and function of the foot post-surgery.
A pivotal component in first MPJ arthrodesis is the adequate preparation of the joint. Properly releasing the joint ensures successful fusion by minimizing non-union risks. Essential steps include the thorough release of the adductor hallucis and sesamoidal-phalangeal ligament. By accessing these structures, surgeons can effectively prepare the joint, ensuring the best chance for a successful outcome. This preparation also plays a crucial role in achieving correct alignment and function of the foot post-surgery.
Another consideration during surgery is the length of the plate used. Research indicates a notable increase in failure rates with shorter plates, with failure defined as incomplete bony union or implant breakage. Hence, utilizing longer plates is advocated to gain additional purchase in the diaphyseal bone. This strategy not only helps to reduce the mechanical stress on the fixation construct but also enhances stability, which is crucial for a durable surgical outcome.
Correct positioning during surgery significantly influences the success of first MPJ arthrodesis. Utilizing an axial K-wire during the procedure helps simulate the weight-bearing surface and achieves the desired dorsiflexion angle of 5 – 10 degrees. Furthermore, maintaining the appropriate length of the first ray is vital to prevent complications, such as transfer metatarsalgia. The alignment and positioning substantially affect foot biomechanics, reinforcing the need for meticulous attention during surgery.
Management of Non-Unions
In cases where non-union occurs, medical treatment options such as teriparatide can be beneficial. This synthetic parathyroid hormone, typically used for osteoporosis, boosts osteoblastic activity, accelerating fracture healing. Studies demonstrate that patients using teriparatide experienced quicker union times, making it a promising treatment adjunct for non-unions in first MPJ arthrodesis cases.
For more severe non-union cases, surgical revision using orthogonal plate fixation is a preferred approach. This method involves placing 2 plates at approximately 90 degrees to each other, offering significantly enhanced structural stability over unilateral plating. The increased strength and stability of orthogonal plating have been supported in studies involving femur and Lapidus fusions, making it an effective strategy for managing non-unions.
Bone grafting plays a crucial role in revision surgeries, as it facilitates the healing process by providing a scaffold for new bone growth. Pre-cut allografts soaked in bone marrow concentrate are often used to ensure healthy, bleeding surfaces and to maintain the length during revision procedures. This technique is essential for creating a conducive environment for fusion and restoring the length and stability of the medial column of the foot.
Conclusion
Meticulous surgical techniques, such as adequate joint preparation and the use of longer dorsal plates, play a critical role in minimizing the occurrence of non-unions. When it does occur, orthogonal plating and teriparatide as proven options as advanced strategies in non-union management. These approaches not only enhance healing outcomes but also improve the overall structural integrity and alignment of the foot, making them vital considerations for optimizing patient results in foot surgery.
Patrick DeHeer, DPM FACFAS, FFPM RCPS (Glasg) is now Medical Director at Upperline – Indiana and Podiatric Residency Director at Ascension St. Vincent Hospital in Indianapolis.
This article is a summary of Dr. DeHeer’s presentation, “Non-union after a 1st MPJ arthrodesis, now what and how I can reduce the odds of this happening again?,” from the APMA Surgical Complications Virtual Seminar held January 28, 2025. To view the full presentation with questions and answers—and see the agenda for the daylong program, visit https://apmasurgical.lerexpo.com/en/login. Continuing education credits are available for this and many of the lerEXPO programs.





