 By Elke Lathouwers, María Alejandra Díaz, Alexandre Maricot, Bruno Tassignon, Claire Cherelle, Pierre Cherelle, Romain Meeusen, and Kevin De Pauw
By Elke Lathouwers, María Alejandra Díaz, Alexandre Maricot, Bruno Tassignon, Claire Cherelle, Pierre Cherelle, Romain Meeusen, and Kevin De Pauw
A better understanding of the therapeutic benefits of performing daily activities with passive, quasi-passive, and active ankle-foot prostheses in people with a lower limb amputation can help gauge the impact of these prostheses on quality of life.
After lower limb loss, assistive devices are a fundamental part of rehabilitation with the aim to restore daily activities and improve quality of life. A prosthesis is generally favored among assistive devices as it enables a person to carry out daily activities as naturally as possible. The current evolution in prosthetic development is shifting from developing passive prostheses to quasi-passive and active prostheses in order to minimize prosthetic-related adverse events affecting quality of life. It also helps to enhance self-esteem as it ensures that people diverge as little as possible from the physical appearance of able-bodied individuals.
Lower limb prostheses also complicate the performance of daily activities. This performance is affected by several factors, including the type of prosthesis, prosthetic embodiment, the level and cause of the amputation, degree of mobility, and presence of comorbidities. These factors complicate tasks such as positioning the foot in space, walking horizontally, going up and down ramps and stairs, crossing obstacles, walking on slippery floors, and transitioning between activities. For instance, it has been well-established that walking with a lower limb prosthesis results in aberrations in gait kinetic and spatiotemporal parameters compared to able-bodied walking. Additionally, prosthetic use may cause falls and secondary injuries, including low back pain and osteoarthritis of the healthy knee and hip, entailing high medical costs and diminishing quality of life.
Despite that enhancing the quality of life of people with a lower limb amputation is critical in prosthetic development and rehabilitation, no overview is available concerning the impact of passive, quasi-passive, and active ankle-foot prostheses. With that objective in mind, the study authors conducted a systematic review of the therapeutic benefits of performing daily activities with passive, quasi-passive, and active ankle-foot prostheses in people with a lower limb amputation.
Methods
A search of the Pubmed, Web of Science, Scopus, and Pedro databases was conducted. Only English-written randomized controlled trials, cross-sectional, cross-over, and cohort studies were included when the population comprised adults with a unilateral transfemoral or transtibial amputation, wearing passive, quasi-passive, or active ankle-foot prostheses. The intervention and outcome measures had to include any aspect of quality of life assessed while performing daily activities. The participants’ characteristics, type of prosthesis, intervention, outcome, and main results were synthesized.
Results
The study authors identified 4,281 records and included 34 studies in total. The prosthetic evaluation was mainly conducted through level walking tasks. All studies investigated the short-term effects of performing daily activities with prosthetic ankle-foot devices, and none of the studies examined long-term effects. Biomechanical outcome measures were most frequently gathered, and to a lesser extent physiological, performance, and subjective measures were gathered. Results indicate that quasi-passive and active prostheses are favored over passive prostheses based on biomechanical, physiological, performance, and subjective measures in the short-term. All studies had a moderate or high risk of bias.
Discussion
The purpose of this study was to systematically review the therapeutic benefits of performing daily activities with passive, quasi-passive and active ankle-foot prostheses in people with a unilateral lower limb amputation. Remarkably, no studies investigated the long-term therapeutic benefits.
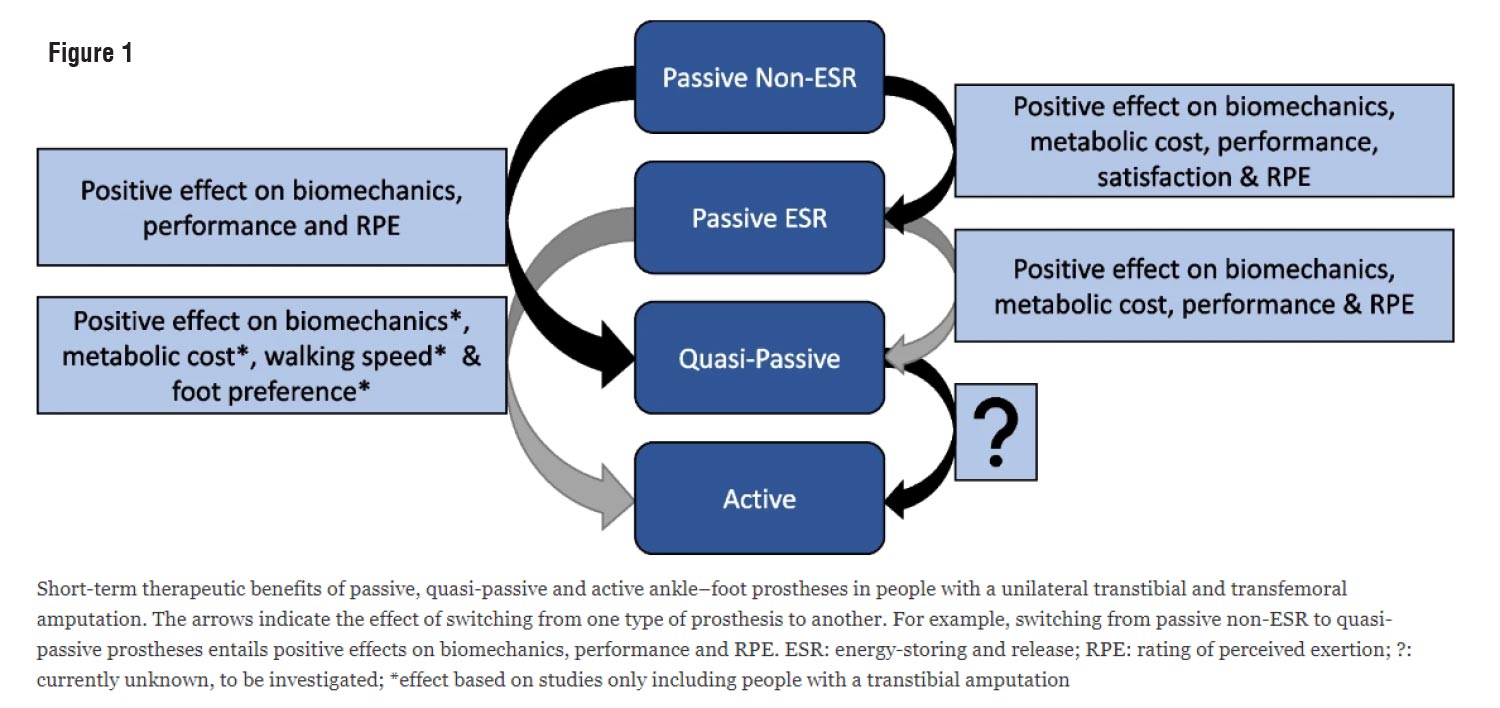 Figure 1 captures the short-term therapeutic benefits of passive, quasi-passive, and active prostheses. This figure shows the domains in which benefits were found. It was not possible to provide such an overview at the outcome measure level due to high heterogeneity. Overall, the numerous outcome measures per study yielded positive results on biomechanical, physiological, performance-related, or subjective outcomes for the more advanced prostheses, implying therapeutic benefits for the individuals walking with them, though all studies also identified no or unfavorable effects. The technological innovations contribute to improving the quality of life in the short-term when people with lower limb amputations switch the conventional passive cushion foot for a more advanced prosthesis (ie, the passive energy-storing release feet, the surface-adaptive quasi-passive feet, the active feet generating an external force through an actuator). However, comparisons between active prostheses and quasi-passive devices have not yet been conducted.
Figure 1 captures the short-term therapeutic benefits of passive, quasi-passive, and active prostheses. This figure shows the domains in which benefits were found. It was not possible to provide such an overview at the outcome measure level due to high heterogeneity. Overall, the numerous outcome measures per study yielded positive results on biomechanical, physiological, performance-related, or subjective outcomes for the more advanced prostheses, implying therapeutic benefits for the individuals walking with them, though all studies also identified no or unfavorable effects. The technological innovations contribute to improving the quality of life in the short-term when people with lower limb amputations switch the conventional passive cushion foot for a more advanced prosthesis (ie, the passive energy-storing release feet, the surface-adaptive quasi-passive feet, the active feet generating an external force through an actuator). However, comparisons between active prostheses and quasi-passive devices have not yet been conducted.
Among the included studies, quality of life has been evaluated using biomechanical, physiological, performance-related, or subjective measures. The biomechanical and physiological dimensions of quality of life have been assessed during level and slope walking in 94% of the included studies, while only 29% included the subjective dimension. In general, gait efficiency and efficacy improved in parallel with technological advances, though gait asymmetries remained. Further in-depth discussion of these parameters is not feasible due to the heterogeneity in outcome measure among the biomechanical and physiological parameters. Nevertheless, it is the ultimate goal of prosthetic development to strive toward the most efficient gait patterns by seeking complete gait symmetry and matching the gait patterns as closely as possible to those of able-bodied individuals. Furthermore, the limited data on the subjective dimension of quality of life revealed that the perceived effort and satisfaction increased in line with the advancement of the devices. The limited use of subjective measures can be attributed to the prohibitive cost of most active and quasi-passive devices for a subset of individuals. This factor might introduce a confounding variable in the data affecting subjective feedback. Conversely, these paywalls will not affect the biomechanical or physiological data. Nevertheless, subjective measures (eg, perceived effort, satisfaction, feedback on the noise of motors in active prostheses) should be more prominent in prosthetic evaluations, as they are crucial to assessing the quality of life.
Due to its biomechanical focus, the prosthetic evaluation primarily targets aberrated movement patterns that can be remedied in the short term by a prosthesis. However, movement patterns are orchestrated by the intertwining between biomechanical factors and the human brain. This entails that the brain plays a vital role in the organization and performance of human gait. Magnetic resonance imaging revealed that amputation causes thinning of the premotor cortex and visual-motor area combined with a decrease in white matter integrity in the premotor area contralateral to the amputation and at a bilateral connection between both premotor cortices. These changes interfere with movement planning or coordinating eye movements in relation to limbs and lead to decreased perception–action coupling. Additionally, amputation causes changes in limb representation in the primary motor cortex and somatosensory cortex, and causes decreased connectivity between many brain areas, including the primary motor cortex, primary somatosensory cortex, basal ganglia, thalamus, and cerebellum. These changes in connectivity translate toward reduced motor control and balance and potentially lead to falls. Remarkably, only a single study examining the effect on brain functioning across prosthetic ankle-foot prostheses has been included in this review. Unravelling neuroplasticity in relation to the type of prosthesis may provide a new understanding of the effects of prostheses to improve the quality of life in people with a lower limb amputation.
A conceivable approach to account for the brain’s influence is through dual tasks, conditional on adequate familiarization. Dual tasks involve the concurrent performance of 2 tasks and are regarded as a measurement of cognitive-motor capacity as they require executive function and attentional demand. Their performance usually results in decreased mobility and deteriorated gait patterns leading to increment falls. Out of the included articles in this review, only 1 investigated the difference between passive and quasi-passive prostheses during the performance of a dual-task during treadmill walking. That study found that only in individuals with a transfemoral amputation attention demands (reaction times and accuracy) increased during walking with the quasi-passive prosthesis compared to the current prosthesis and able-bodied individuals. Lack of familiarization time to habituate to the new prosthetic device may have influenced these results. As discussed earlier, the negative implications of performing dual-tasks are attributable to cognitive demands associated with prosthetic use, balance and gait disturbances, and brain adaptations. Combined with the fact that dual-tasks represent daily activities, the recommendation is to include dual-task paradigms in the evaluation process of prostheses.
The design, development, and evaluation of prosthetic devices is an iterative process requiring high cross-disciplinary collaboration between multiple research branches. This review reveals that the current emphasis in prosthetic evaluation has been placed on comparing ankle-foot prostheses without long-term evaluation. Since none of the included studies investigated the long-term benefits of comparing different ankle-foot prostheses, the study authors stated that they cannot make any substantiated statements about the association between the onset of secondary injuries and the use of different types of prostheses solely based on studies conducted at a single point in time. Furthermore, it should be emphasized that the included studies mainly involved people with a transtibial amputation. In contrast, only 6 of the included studies involved people with a transfemoral amputation, limiting the results’ generalizability within the prosthetic population. Also, the majority of the studies (94%) are based upon biomechanical and physiological findings during the performance of walking tasks, except for 2, which used performance and subjective measures. Another concern relates to the overall high risk of bias. The high risk of bias can be attributed to the lack of randomization, the inability to blind participants to the prosthetic condition, and the lack of reporting protocol deviations. Specifically, the lack of randomization and inability to blind participants are essentially inherent to prosthetic research. Taken all of the aforementioned elements into account, heterogeneity of the outcome measures combined with small sample sizes, limited familiarization time, and the high risk of bias of the included studies do not allow robust conclusions to be made. Therefore, the recommendation is to perform adequate sampled studies with a limited number of outcome measures and ample familiarization time evaluating a prosthetic device during daily activities. Secondly, the recommendation is shifting the emphasis toward the psychosocial dimension of quality of life through questionnaires finding a suitable poise between objective and subjective measures to obtain a thorough insight into the benefits of prosthetic devices. Lastly, the study authors advise conducting prospective studies assessing the benefits of passive, quasi-passive, and active prostheses in the longer term.
Conclusion
This review evaluated the differences in the quality of life between passive, quasi-passive, and active prostheses for people with a lower limb amputation using biomechanical, physiological, performance and subjective measures. Compared to passive ankle-foot prostheses, quasi-passive and active prostheses improve quality of life. Although short-term therapeutic benefits have been established favoring more advanced prostheses, outcome measures’ discrepancies prevail, the brain’s influence on prosthetic functioning is insufficiently studied, and the long-term benefits remain unknown. Investigating these aspects may improve the quality of life of people with a lower limb amputation.
This article has been excerpted from “Therapeutic benefits of lower limb prostheses: a systematic review,” J NeuroEngineering Rehabil. 2023;20:4. https://doi.org/10.1186/s12984-023-01128-5. Editing has occurred, including the renumbering or removal of tables and figures, and references have been removed for brevity. Use is per CC 4.0 International License.





