
By Kazuaki Kinoshita, Yuichi Hoshino, Naoko Yokota, Masayuki Fukuda, Mika Hirata, and Yuichiro Nishizawa
Sever’s disease can be painful and limit young athletes in competitive endeavors. These authors sought to find physical characteristics that could identify those at risk.
 Sever’s disease, also known as calcaneal apophysitis, is an inflammation of the growth plate in the heels of growing children, typically adolescents. This disease is reported to have an incidence of 2%–16 % among musculoskeletal injuries in children. The pain caused by Sever’s disease is often severe enough that the child limps after physical activities to take weight off the affected heel. Most patients with Sever’s disease take 3 to 6 weeks to return to painless activity. Athletes with Sever’s disease are often disadvantaged in being required to suspend or limit their activities during the injury period.
Sever’s disease, also known as calcaneal apophysitis, is an inflammation of the growth plate in the heels of growing children, typically adolescents. This disease is reported to have an incidence of 2%–16 % among musculoskeletal injuries in children. The pain caused by Sever’s disease is often severe enough that the child limps after physical activities to take weight off the affected heel. Most patients with Sever’s disease take 3 to 6 weeks to return to painless activity. Athletes with Sever’s disease are often disadvantaged in being required to suspend or limit their activities during the injury period.
Sever’s disease is an overuse syndrome that could be prevented by some prophylactic measures. Researchers have hypothesized potential intrinsic and extrinsic factors for Sever’s disease. Mechanical stress on the calcaneal growth plate is derived from both heel contact pressure and from plantar fascia and Achilles tendon traction force and can be exacerbated by intrinsic factors such as ankle joint stiffness and Achilles tendon tightness. Extrinsic factors that have been reported to exaggerate the pathological mechanical stress on the calcaneal growth plate include high impact activities, footwear, and sports activities performed on hard surfaces. Another extrinsic factor in the development of Sever’s disease may involve whole-body physical function. The foot is responsible for maintaining balance through forming a supportive surface and for absorbing shock, based on kinetic chain principles. Sever’s disease affects the proximal segment of the foot, which can make stabilization difficult during static and dynamic activity, with subsequent proximal segment function reciprocally affecting whole body function.
Sever’s disease occurs frequently in gymnasts. Two cohort studies have reported that gymnastics-related inversion ankle injuries are the most frequent lower extremity injuries, followed by Sever’s disease. Gymnastics involves the repetitive, jarring impact of vault takeoffs and dismounts from a variety of heights and tumbling activities. Additionally, gymnasts must perform barefoot without the support of shoes that attenuate impact during jumping and running, and, thus, Sever’s disease is highly disadvantageous for gymnasts. Empirical evidence concerning risk factors or the physical characteristics in Sever’s disease remains limited. Therefore, this prospective cohort study, using functional tests, aimed to determine which physical characteristics of junior gymnasts might contribute to the development of Sever’s disease. We hypothesized that specific risk factors related to the development of Sever’s disease would be identified. The secondary objective is to explore the relationship between these identified characteristics and the incidence of Sever’s disease in gymnasts. Through elucidating these relationships, the findings aim to inform preventive strategies and optimize the management of Sever’s disease in this athletic population.
Methods
This study included 74 limbs from 37 junior gymnastics athletes, of whom 15 were males and 22 were females. The mean age, height, weight, and Rohrer index of the participants were 11.5 ±1.7 years, 140.1 ±10.5 cm, 33.7 ±8.4 kg, and 120.3 ±8.1, respectively. The participants engaged in approximately 18 hours of training per week. During this period, they did not use an orthosis to prevent Sever’s disease. We excluded individuals who had heel pain at the start of the study, ankle injuries and/or complaints, those with neurological or orthopedic abnormalities, individuals who complained of pain during the measurements, and those unable to complete the measurements due to the risk of further injury.
The evaluation items were 4 basic demographic data: age, height, weight, and Rohrer index; 3 flexibility measurements: generalized joint laxity (GJL), heel buttock distance (HBD), and ankle dorsiflexion angle (knee flexion position); 2 foot alignments: arch height ratio and leg heel angle; 5 trunk function tests: side bridge test, abdominal muscle function, back muscle function, back and abdominal muscles strength ratio; and 3 functional balancing tests; 1-legged standing, Star Excursion Balance Test (SEBT), and figure-of-8 hop. All the items were measured by the same person. All data are expressed as mean ±standard deviation.
The study observed gymnasts with Sever’s disease over 6 months from the first date of measurement. Those diagnosed at a medical institution as having Sever’s disease were classified into a Sever’s disease group, and those who did not have pain or who had not been diagnosed at a medical institution were classified into a no-symptom group. Participants were required to seek medical attention if they experienced pain lasting more than 2 weeks. If, during that examination, Sever’s disease was ruled out, they were categorized into the no-symptom group. This study incorporates elements of a cohort study rather than a cross-sectional design. The Mann–Whitney U test was used to compare the 2 groups. A stepwise logistic regression analysis was used to identify factors involved in Sever’s disease at 6 months, with the above mentioned factors as explanatory variables, and the odds ratios and 95% confidence intervals were calculated. The explanatory variables were narrowed down in advance by using the variable increase or decrease method. The input or removal values at this time were P = 0.20–.25. Statistical analysis was performed using IBM SPSS Statistics for Windows, (IBM Corp., Armonk, NY, USA). The statistical significance level was set at P < 0.05.
Results
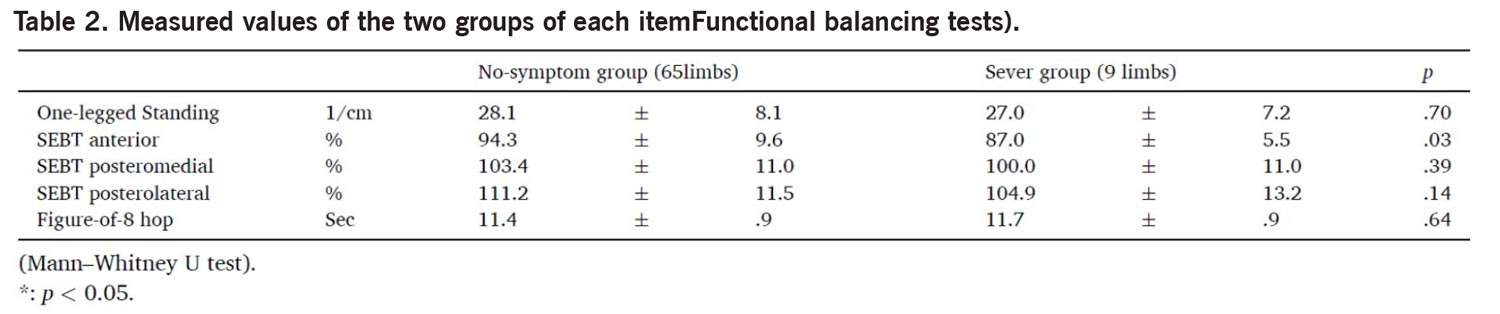
The Sever’s group comprised 9 limbs (males, n = 2 limbs; females, n = 7 limbs). One male and 2 females exhibited symptoms bilaterally. Therefore, the total number of individuals in the Sever group was 6. The arch height ratio was significantly lower in the Sever group (12.4 ± 1.6 %) than in the no-symptom group (13.9 ± 2.1 %) (Table 1). The anterior SEBT values were significantly lower in the Sever’s group (87.0 ± 5.5 %) than in the no-symptom group (94.3 ± 9.6 %) (Table 2). There were no other significant differences between the 2 groups. Logistic regression analysis was conducted to identify the independent relationships between Sever’s disease and suspected risk factors. The explanatory variables were first narrowed down through applying a refining process. The result included 3 items (Rohrer index, arch height ratio, and anterior SEBT values). Finally, the arch height ratio and anterior SEBT values were applied to the model (Table 3).


Discussion
The main study findings indicated that there was a lower arch height ratio and reduced dynamic postural balancing function, as evaluated using the anterior SEBT, among the junior gymnasts who developed Sever’s disease.
In this study, no difference or association was observed in the ankle dorsiflexion angle. Instead, the Sever’s group had a greater ankle dorsiflexion angle approaching significance. Potential intrinsic factors include a limited range of ankle dorsiflexion motion. The calcaneal growth plate and apophysis are situated in an area susceptible to high stress from the plantar fascia and Achilles tendon and may be affected by increased tension on the calcaneus. Sever’s disease has also been reported to be caused by tightness of the Achilles tendon. But Rolf et al questioned the existence of excessive tightness in the triceps surae. The reason is that in studies of patients with Sever’s disease, multiple raters typically evaluate the dorsiflexion of the leg, which reduces the uniformity of measurement and the reliability of the results. Furthermore, there are significant differences between the current study and previous literature in the methods used to assess ankle dorsiflexion angle. In previous studies examining ankle dorsiflexion angle and heel pain, participants were assessed with the knee extended. Since knee extension biases the gastrocnemius muscle, while knee flexion has a Soleus bias, it is possible that tightness in the gastrocnemius muscle may have gone undetected in the case group. Therefore, some studies suggest an increase in ankle dorsiflexion due to the increased range of motion as a causative factor not previously considered. Further discussions are required in the future.
The findings of lower arch height ratio are corroborated by prior research. Sever’s disease also occurs more commonly in children who overpronate and involves both heels in more than half of the patients. Sever and Lewin reported that there may be a slight amount of protonation present, which should be addressed. A lower arch height ratio can cause excessive stress on the surrounding soft tissues, causing muscle imbalance and abnormal joint alignment, as well as overuse syndromes. Clinicians often use postural-control assessments to evaluate the risk of injury, the initial deficits resulting from injury, and the level of improvement after intervention for an injury.
This study yielded a new finding that the decreased SEBT values are associated with Sever’s disease, which has not been previously reported. The SEBT values are used as an index of dynamic postural control (ie, a greater distance reached indicates better dynamic postural control). High school basketball players who had a lower SEBT during the preseason were 7 times more likely to sustain ankle injuries. Particularly, it has a significant relationship with chronic ankle instability. Previous studies have reported that dynamic balance may better reflect the sensorimotor control mechanisms required for sports-specific tasks. Moreover, most overuse injuries occur in the lower extremities, especially the knees, ankles, and feet. The most typical is reported to be Sever’s disease. Additionally, previous studies have reported that the anterior SEBT reach significantly affects ankle dorsiflexion angle and plantar sensory function compared to the posteromedial and posterolateral SEBT reaches. In this study, there were no problems with the ankle dorsiflexion angle, which is considered to be related to dynamic balance. This suggests that dynamic balance is likely involved.
The overlap between these 2 factors may be important in the development of Sever’s diseases. It has been reported that a decrease in the arch height ratio and SEBT leads to decreased lower limb support, neuromuscular control, proprioceptors, and static and dynamic balance abilities. This may lead to overuse of the muscles around the foot and ankle joints. The arch is controlled by both local stabilizers and the global movers of the foot. Local stabilizers are plantar intrinsic muscles that originate and insert on the foot; they have small moment arms and serve primarily to stabilize the arches. Many of these muscles are attached to the heel. Global movers have larger moment arms, are prime movers of the foot, and provide some stability to the arch. These typical Achilles tendons are attached to the heels. In other words, the overuse of these muscles can damage the heel. Furthermore, an unstable lower leg increases the risk of direct damage to the heel. The main theory in the literature on the pathophysiology of Sever’s disease is that it is an overuse syndrome due to repetitive microtrauma caused by increased traction on the apophysis. So, these 2 factors put strain on the calcaneus.
Conclusions
Though limited by its small sample size, this study provided valuable data on the characteristics contributing to the development of Sever’s disease in junior gymnasts. The main study findings indicated that there was a lower arch height ratio and reduced dynamic postural balancing function, as evaluated using the anterior SEBT, among the junior gymnasts who developed Sever’s disease. In this study, there was no observed decrease in the commonly mentioned ankle dorsiflexion angle. These results will contribute to the prevention of Sever’s disease. However, further research is needed to demonstrate the effectiveness of Sever’s disease prevention. Future research will continue to unravel the complex interactions between Sever’s disease and various factors, aiming to discover superior treatment strategies.
Kazuaki Kinoshita is with the Department of Physical Therapy on the Faculty of Rehabilitation at Shijonawate Gakuen University in Osaka, Japan.
Yuichi Hoshino is with the Department of Orthopaedic Surgery in the Graduate School of Medicine at Kobe University in Hyogo, Japan.
Naoko Yokota is with the Kishimoto Orthopedic Rehabilitation Clinic in Osaka, Japan.
Masayuki Fukuda and Mira Hirata are with the Center of Rehabilitation at Kobe Kaisei Hospital in Hyogo, Japan.

Yuichiro Nishizawa is with the Department of Orthopaedic Surgery at the Hiro sports clinic in Hyogo, Japan.





