
By Michael J. Callaghan, Jinal Pravin Gala, and Edward Roddy
There is a need for guidance to help allied healthcare professionals manage an evidence-based treatment plan of usual care for ankle osteoarthritis.
 International clinical guidelines recommend non-pharmacological interventions such as exercises and weight loss as first-line management for osteoarthritis (OA), regardless of joint site. Whereas several evidenced-based non-surgical management options for clinicians and patients are available for other joints, specific evidence for ankle OA interventions is sparse and patients report mixed experiences of non-surgical management. Extrapolating recommendations from other joints may not be appropriate and there is a lack of guidance for clinicians on treatment best practices. Therefore, the study authors undertook a survey of United Kingdom (UK)–based physiotherapists and podiatrists to understand better how painful ankle OA is managed in current clinical practice.
International clinical guidelines recommend non-pharmacological interventions such as exercises and weight loss as first-line management for osteoarthritis (OA), regardless of joint site. Whereas several evidenced-based non-surgical management options for clinicians and patients are available for other joints, specific evidence for ankle OA interventions is sparse and patients report mixed experiences of non-surgical management. Extrapolating recommendations from other joints may not be appropriate and there is a lack of guidance for clinicians on treatment best practices. Therefore, the study authors undertook a survey of United Kingdom (UK)–based physiotherapists and podiatrists to understand better how painful ankle OA is managed in current clinical practice.
Methods
UK-based physiotherapists and podiatrists who treat patients with ankle OA completed a self-administered online questionnaire about their professional and clinical service characteristics, diagnostic criteria, treatment aims, preferred treatment options, and treatment outcome measures. Participants were required to care for people with symptomatic ankle OA in their clinical practice but there were no exclusions for age, length of experience, or clinical setting. Participants were advised that for the purpose of this survey ankle OA was defined as talocrural (tibiotalar) joint OA and did not include the subtalar joint. Data were collected anonymously and stored on JISC online survey (www.onlinesurvey.ac.uk). ‘Usual care’ was defined as a combination of ‘Always’ and ‘Frequently’, and ‘Not usual care’ was defined as ‘Sometimes,’ ‘Rarely,’ ‘Never’, and ‘not applicable’ combined. Statistically significant differences in responses between the physiotherapists and podiatrists were analyzed using X2 tests for each treatment modality. Statistical significance was set at P < 0.05.
Results
Between June 1 and August 31, 2021, 98 valid responses to the survey were received from 63 physiotherapists and 35 podiatrists. The most common treatment aims in both professions were to reduce pain (n = 87, 89%) and improve quality of life (n = 82, 84%). Several outcome measures were used, most commonly patient satisfaction (n = 62, 63%) or a visual analogue scale (n = 51, 52%) or a numerical rating scale (n = 42, 43%) to measure pain. Physiotherapists and podiatrists relied upon various features to diagnose ankle OA, with the 3 most common being reduced ankle range of motion (n = 90, 92%), the site of pain (n = 81, 83%), and imaging (n = 85, 87%). Fifty respondents (51%) offered 3 or 4 treatment sessions and 53 respondents (54%) saw patients for 30–40 minutes at the first treatment session.
The 5 most common modalities used by physiotherapists were patient education (n = 63, 100%), teaching self-management (n = 58, 92%), lifestyle modification (n = 54, 86%), ankle strengthening (n = 55, 87%), and proprioception exercises (n = 54, 86%) (Figure 1). For podiatrists, these were patient education (n = 35, 100%), ankle strengthening (n = 31, 89%), activity pacing (n = 28, 80%), lifestyle modification (n = 27, 77%), and gait training (n = 27, 77%). Less than 30% of respondents in either profession opted for ankle bracing or taping as usual care. Physiotherapists used the treatment options of proprioception (P = 0.003), hip strengthening (P = 0.007), hydrotherapy (P = 0.031), and self-management (P = 0.001) significantly more often than podiatrists (Figure 2). Taping (P = 0.025), bracing (P = 0.04), orthotics (P = 0.002), referral for surgery (P = 0.029), and corticosteroid injections (P = 0.004) were used significantly more often by podiatrists than physiotherapists (Figures 1, 2).
Discussion
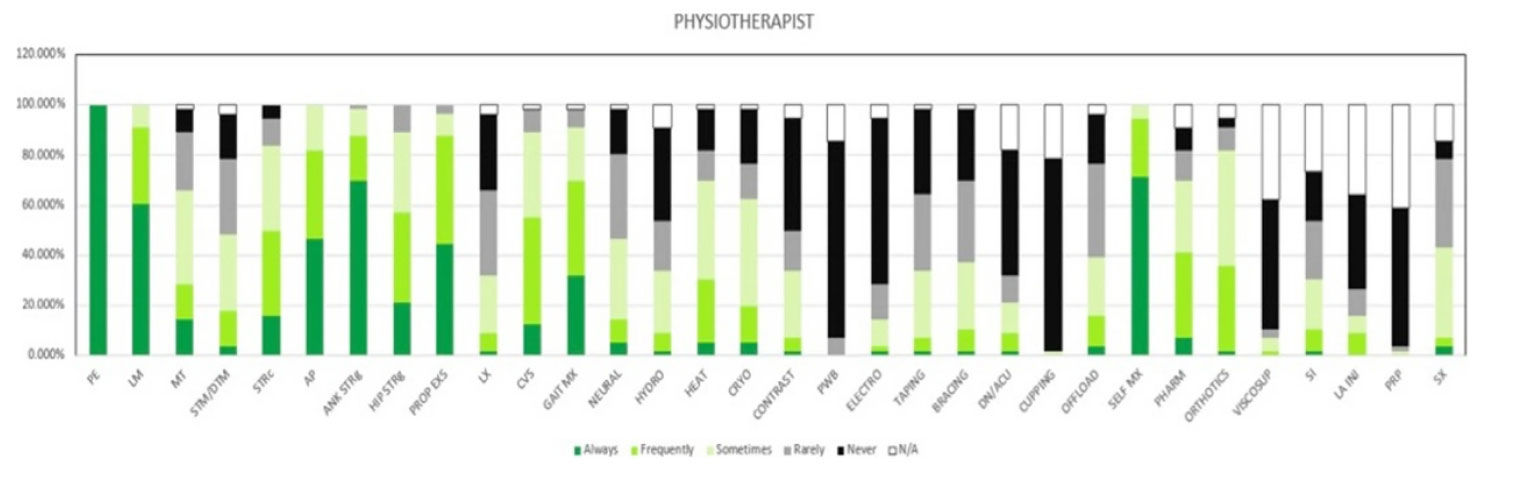
Figure 1: Treatment used for ankle OA by Physiotherapists. Figures are presented as a % of valid responses (n = 98). PE, patient education; LM, lifestyle modification; MT, manual therapy of peripheral joints; STM/DTM, soft tissue mobilisation/ deep tissue mobilisation; STRc, stretching; AP, activity pacing; ANK STRg, ankle strengthening; HIP STRg, hip strengthening; PROP EXS, proprioception exercises; LX, lumbar spine management; GAIT Mx, gait management; NEURAL, neural mobilisation; HYDRO, hydrotherapy; HEAT, heating/ heat therapy; CRYO, cryotherapy; CONTRAST, contrast bath; PWB, paraffin wax bath; ELECTRO, electrotherapy; DN/ACU, dry needling/ acupuncture; OFFLOAD, offloading; SELF MX, self-management; PHARM, pharmacotherapy; VISCOSUP, visco-supplementation; SI, steroid injection; LA INJ, local anaesthesia injection; PRP, platelet-rich plasma injection; SX, refer for surgery
This is the first survey to assess and compare current practice in managing ankle OA amongst physiotherapists and podiatrists in the UK. There is little guidance currently available to help allied healthcare professionals plan an evidence-based management plan of usual care for managing this condition; most guidance is for knee OA and hip OA.
Both professions always or usually used patient education, lifestyle modification, and ankle strengthening exercises, with physiotherapists additionally using self-management and proprioception exercises, whereas podiatrists additionally used activity pacing and gait training. Outside of these 5, other commonly used ways to manage ankle OA by physiotherapists were hip strengthening (58%) and by podiatrists were orthotics (73%) and self-management (64%). These treatment choices align with the top 3 treatment aims in both professions: to reduce pain, improve quality of life, and teach self-management. This consensus concurs with many general OA guidelines (not ankle OA specific), such as National Institute for Health and Care Excellence (NICE) and Osteoarthritis Research Society International (OARSI), which includes patient education, exercise, and self-management as core treatment options. Additionally, the results of this survey align with the treatment research agenda from an international foot and ankle OA consortium, which recommended understanding usual care of foot and ankle OA to inform the design of control interventions in clinical trials. It is also in line with the modern rehabilitation model for chronic pain, which suggests using education to improve the effectiveness of other treatment options and adding active/self-management techniques as a part of usual care.
Some of the treatment options reported by physiotherapists suggest they extrapolated evidence from other joint sites and applied to ankle OA. Hip strengthening was commonly used by physiotherapists (58%) but not podiatrists (27%), which does not align with a systematic review recommending hip strengthening for the conservative management of knee OA but not ankle OA. There were several treatment options that were used sometimes, rarely, or never by physiotherapists or podiatrists including hydrotherapy, electrotherapy, dry needling/acupuncture, taping, and intra-articular injections of visco-supplementation or platelet-rich plasma (PRP). Possible reasons include lack of access to hydrotherapy, contradictory OA guidelines by NICE and OARSI about acupuncture for OA, a lack of injection skills, and either the limited availability of visco-supplementation products or PRP in the National Health Service or a lack of supporting evidence. The observation that few physiotherapists (4%) and podiatrists (15%) used electrotherapy to treat ankle OA contrasts with NICE and OARSI guidelines recommending transcutaneous electrical nerve stimulation (TENS) to alleviate pain.
Less than a third of respondents in either profession opted for ankle bracing or taping as usual care. This is surprising, particularly with physiotherapists, since taping is commonly used to reduce ankle range of motion and improve joint stability. The aim of ankle braces is similar, but the low uptake of bracing might be due to the survey not specifying the stage of ankle OA clinicians should consider when responding to these questions. It might be that some clinicians only consider ankle bracing in end-stage ankle OA.
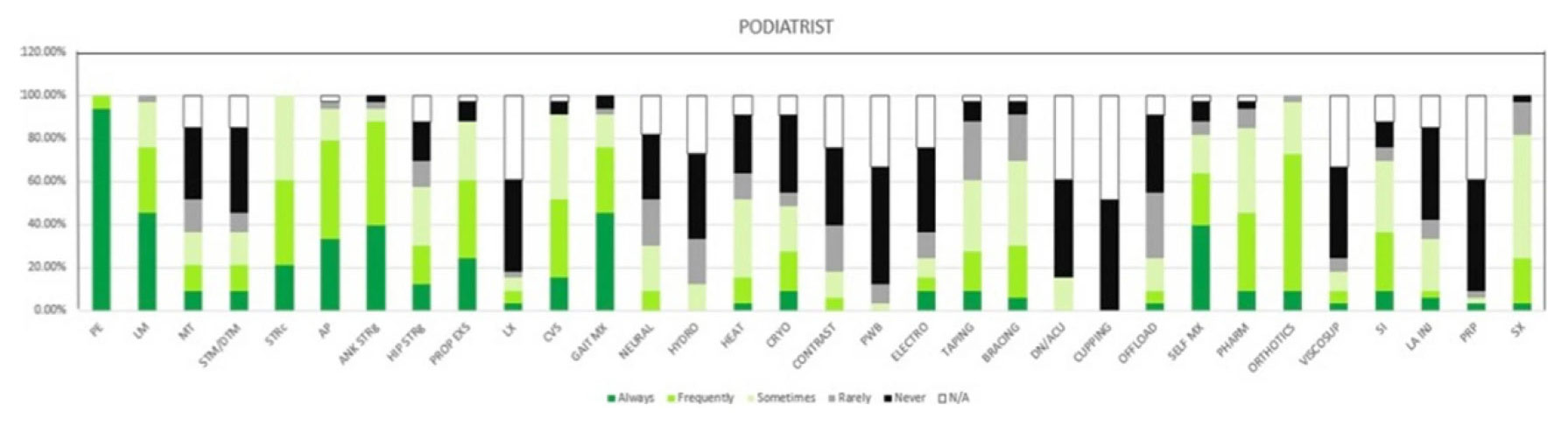
Figure 2: Treatment used for ankle OA by Podiatrists. Figures are presented as a % of valid responses (n = 98). PE, patient education; LM, lifestyle modification; MT, manual therapy of peripheral joints; STM/DTM, soft tissue mobilisation/ deep tissue mobilisation; STRc, stretching; AP, activity pacing; ANK STRg, ankle strengthening; HIP STRg, hip strengthening; PROP EXS, proprioception exercises; LX, lumbar spine management; GAIT Mx, gait management; NEURAL, neural mobilisation; HYDRO, hydrotherapy; HEAT, heating/heat therapy; CRYO, cryotherapy; CONTRAST, contrast bath; PWB, paraffin wax bath; ELECTRO, electrotherapy; DN/ACU, dry needling/ acupuncture; OFFLOAD, offloading; SELF MX, self-management; PHARM, pharmacotherapy; VISCOSUP, visco-supplementation; SI, steroid injection; LA INJ, local anaesthesia injection; PRP, platelet-rich plasma injection; SX, refer for surgery
Orthotics were used significantly more by podiatrists (73%) than physiotherapists (37%), consistent with the finding of a survey of physiotherapists’ and podiatrists’ treatment of plantar fasciitis that foot orthotics were considered the specialist role of podiatrists. It is possible that physiotherapists refer to other services for orthotics but this survey did not distinguish those fitting orthotics themselves and those referring to podiatric or orthotic services. The use of footwear, as opposed to orthotics, was not available as a treatment option in the survey and it is possible that respondents may have opted for this if it had been available. Interestingly, despite podiatrists being asked to contribute at the survey’s development stage, a ‘footwear’ option was not suggested and so was not included in the final version. Although this survey provides data from physiotherapists and podiatrists as to what is current practice for ‘usual care’ in ankle OA, this has not yet been robustly assessed for its efficacy and should be the target for future funding applications.
A survey on the management of foot and ankle OA by general practitioners in Australia found that pharmacological management was favored over active and self-management techniques. The survey reported on herein found medications were used by nearly half of both physiotherapists and podiatrists. There are about 1,400 physiotherapists and 450 podiatrists registered as independent or supplementary prescribers in the UK, but the survey did not ask whether medications were prescribed directly by the physiotherapist or podiatrist, or whether the patient was required to see another healthcare professional to obtain a prescription.
Conclusions
This first-ever survey revealed UK-based current practices of physiotherapists and podiatrists to treat painful ankle OA. This study provides a better understanding of how ankle OA is treated in UK current clinical practice and can inform future clinical trials to assess usual care and compare this with new treatment modalities.
Michael J. Callaghan, PhD, MPhil, MCSP, is professor of clinical physiotherapy with the Faculty of Health & Education, Department of Health Professions, Manchester Metropolitan University, UK. He researches in physiotherapy and rehabilitation medicine. He is an MAHSC honorary clinical professor at the Centre for Musculoskeletal Research, University of Manchester, and research fellow/clinical specialist physiotherapist, with the Department of Physiotherapy, Manchester University Hospitals NHS Foundation Trust.
Jinal Pravin Gala, is a physiotherapist with the Department of Health Professions, Manchester Metropolitan University, UK.
Edward Roddy, PhD, is a professor of rheumatology with the School of Medicine, Keele University, Staffordshire, UK, and works clinically and as an Honorary Consultant Rheumatologist at Haywood Hospital, Midlands Partnership NHS Foundation Trust. He is a Fellow of the Royal College of Physicians.
This article has been excerpted from “Ankle osteoarthritis: an online survey of current treatment practices of UK-based physiotherapists and podiatrists.” Journal of Foot and Ankle Research. 2023;16:8. https://doi.org/10.1186/s13047-023-00683-3. Editing has occurred, including the renumbering or removal of tables and figures, and references have been removed for brevity. Use is per CC Attribution 4.0 International License.





