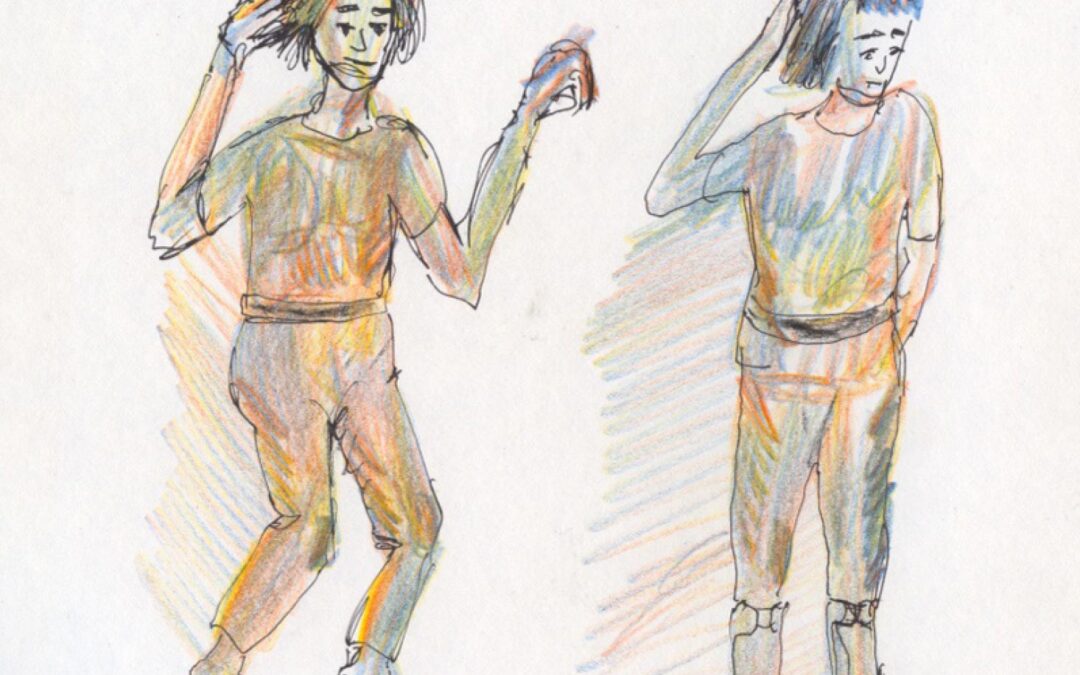

Images of Anka. Left, Anka toe walking without Posterior Leaf Splint Solid Ankle-Foot-Orthoses. Right, note downward heel placement while using Posterior Leaf Splint Solid Ankle-Foot-Orthoses. Original images provided by author.
By Dalia Zwick PT, PhD
The other day, Anka (not her real name), a 19-year-old woman with Autism Spectrum Disorder (ASD) came to our clinic for her regular follow-up visit. While she walked independently, she exhibited severe Toe-Walking Behavior (TWB). She was accompanied by her father and an older brother. Her father was holding a bag with her Posterior Leaf Splint (PLS), a type of ankle-foot orthosis (AFO). When we asked how she is doing, her father said that she is doing very well. He then placed the AFOs and her sneakers on her feet and lower legs, and viola, now she was placing her heel down in standing, sitting, and walking positions—no more TWB.
My clinical role as a physical therapist is to assess needs and provide proper care for individuals with Physical or/and Intellectual Disabilities (PD/ID), including those who have ASD. I work at a clinic we call PT, P&O (short for Physical Therapy, Prosthetics & Orthotics), meaning that during every visit a physical therapist and a certified orthotist are present. Both of us contribute our professional knowledge and although, at times, we might have different opinions, we discuss and develop the best approach that both of us with our different perspectives as well as the individual and their circle of care agree on.
We’ve been following Anka’s posture and gait challenges at our clinic, every 6 months for the last 7 years. Our approach to her posture and gait issues is to observe her standing, sitting, and walking with and without shoes and to assess her ankle range of motion (ROM). We then compare current assessments to the previous visits and adjust the angle of plantar flexion in the AFO accordingly. We review home physical therapy (PT) instructions with the family, which includes drawings of exercises, and reminders of posture care, which means alignment in every posture and support under the heel even when sitting and wearing the AFO while awake. The PLS AFO type of brace is customized to support and prevent her from plantar flexion tendency with a lift, as a support under the heel. Every 6 months we alter, repair, and reduce the amount of the heel lift as her plantar flexor contractures elongate (Figure 1). Anka received PT at her school, but it was inconsistent and eventually halted as the PTs were unable to justify the therapy within the educational system. Common, yet unfortunate reality.
So why has today’s visit left us with feelings of failure and disappointment? Are we doing everything we can to help Anka with her posture and gait issues? Before answering these questions let’s review the general understanding of the underlying issues of posture and Autism.

Figure 1. Sketch depicting the process of fitting the brace with a lift and gradually reducing the need for the heel lift or the brace; custom orthotics continue to support the ankle/foot complex. A) Toe walking without a brace. B) Heel is still up, but brace with a lift is added. C) Heel is slowly and volitionally lowered reaching the brace. D) Heel is down, and a lifelong custom orthotic is provided to help support the ankle/foot complex.
Posture and Autism
Postural and gait impairments, including toe walking, are extremely prevalent among individuals with Intellectual Disability and those who have ASD or are on the spectrum. Why this occurs in this population is not fully known.
What we do know is that the tendency to hold a particular body position in an abnormal way causes stress on the joints, muscles and vertebrae column. It appears that many individuals with ASD have a limited repertoire of movement combined with sensory processing issues and therefore they are less likely to change from an unnatural position into a better posture. Change in posture occurs when the body gives a sensory signal of discomfort. It is obvious that long duration of staying in an abnormal posture may cause body distortions, soft tissue changes, weakness, and pain. Eventually this may lead to a reduction in ability or motivation to participate in functional daily activities.
Some of the postural impairments that are often observed are kyphosis, scoliosis, leg length discrepancy, distortions of foot and ankle joints, and various gait deviations. Many of these postural impairments are manifestations of the disorder: they result from the individual staying in or holding unnatural positions which force muscles, tendons, and ligaments to be under biomechanical stresses which increase pressure on joints, bones, and spinal discs. These positions may happen while lying, sitting, standing, and/or walking (Figure 2). Research in this area is extremely limited and it is mostly from anecdotal reports from patient chatboards or websites such as Quora.
Here’s a comment from an individual with ASD describing his awkward sitting posture on an internet chatboard1—note the drive for comfort in one’s own body:
“I don’t know why I prefer to sit that way…I wish I could break the habit; I think it’s bad for my lower back. But when I have my feet on the floor, I feel uncomfortable, and I have to keep shifting around a lot.”

Figure 2. A) good standing position; B), C), and D) represent unnatural positions, which, when held too long, can become habitual and changes the shape of the body.
Here’s what other patients have told us:
- “TWB is it’s an urge it’s a need it’s a need to tighten”
- “Many individuals with ASD have an urge to tighten we have tight shoulders some of us we some of us don’t move our arms when we walk”
- “Lack of grounding or a kind of flowing in a river floating along and there’s no ground there’s no support, no stability no firm foothold grounding”
- “A sign of fear it’s a sign of anxiety and a defense against that fear and a defense against that anxiety”
- “It might have something to do with retained primitive reflexes some of these reflexes we might have it as infants”
- One girl’s father told us: “Look at boxers before a fight.” So I googled and found this: It’s a gesture that people make when they are excited or impatient. They are standing on the ground while they use their toes to bounce up and down.
Assessing Posture in Clinic

Figure 3. Office sketches with annotations.
PT assessment includes observation of an individuals’ posture when they are sitting, standing, and walking barefoot both without and with shoe wear. On certain occasions, lying posture assessment is also needed. I often sketch people on the bus, or subway or while in urban gathering areas. As a therapist, I realized that sketching movement and posture of patients helps me pay attention to important details. I often draw a very rudimentary basic contour outline or even stick figure of an individual’s posture and annotate what I observe (Figure 3). This process helps me explain and share with patients/caregivers.
I try to observe as an artist would. Artists study the shape, angles, and curves of the human body to accurately depict it. The level of attention that is required to do so improves one’s overall observational skill as well as understanding of the human body.
When observing posture, it helps imagining proper posture of the body as a stack of symmetrical, aligned shapes with midline or line of gravity, viewing it from different directions and different positions. When viewing posture, one should try to imagine how the line of gravity passes through the body. Ask yourself the question: Is what you see a set of stacked shapes that is well aligned? Or is it misaligned boxes? (Figure 4.)
Standing Posture
When standing, we all often tend to stay in an asymmetrical posture, shifting weight onto one leg—habitually it will be the same preferred leg. When we do so, we often get a sensation of discomfort, and unconsciously shift to the other leg. It appears that individuals with ASD ignore this discomfort sensation and stay consistently on the same single leg. At times, the bodily discomfort of continuing to stand in this posture, instead of shifting the weight to the other leg, may trigger behavioral issues, such as nervousness or impatience (often described as fidgeting), or fatigue. Standing on the same single leg may have long-term effects of hip migration or limb length discrepancy, and, at a later stage, may cause a reduction in or loss of the ability to walk.2
In art, models are purposely asked to shift weight onto a single leg in standing, so the body will appear asymmetrical with pronounced curvatures. The term used to describe the artistic posture is Contrapposto. Contrapposto standing is characterized by placing most of the body weight on one leg (Figure 5). The leg that carries the weight of the body is known as the engaged leg and it is straight, hyperextended, or at times slightly bent, while the free leg without the weight is often rotated and bent. This posture is often seen in individuals with ASD. However, because of the extended length of time individuals stay in this contrapposto position, it may cause pain, and it often acts as a short leg.
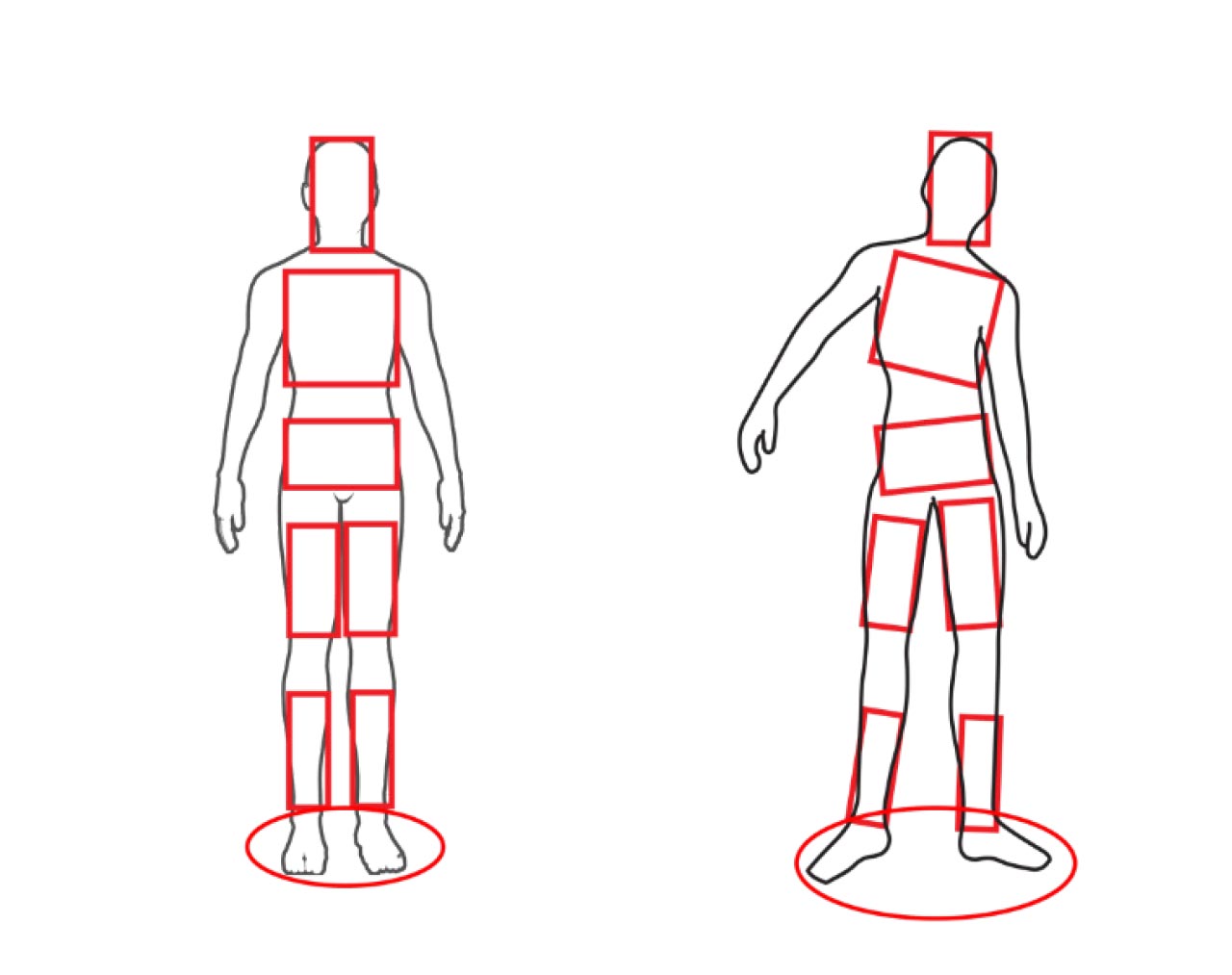
Figure 4. When viewing the body as stack of boxes, it is easier to see the difference between proper posture (left) and misaligned or abnormal posture (right).
Key questions to ask when assessing standing posture include: Is weight evenly distributed on feet, and if not, what leg is bearing most weight? What and where are compensations taking place at the other leg’s knee, foot, and ankle? If you can answer these questions, you will begin to understand the main issue in an individual’s posture.
Sitting Posture
Postural impairments of adults with ASD can be best explained as the consequence of early life poor habits untreated, or undermined and unresolved issues. In sitting, we often see abduction and external rotation of the legs which will affect standing. This abduction and external rotation may start as a habit and eventually will be observed in standing and walking (Figure 6). Placement of feet will affect the rest of the body, causing distortion to different body parts, eg, the externally abducted leg will enhance pronation at the subtalar joint.

Toe-Walking Behavior
Toe walking is most frequent in children with ASD, followed by individuals with communication disorders and learning disabilities.3 A 2019 study by Leyden et al reported that 8.4% of patients with ASD had a diagnosis of toe walking compared with typically developing children where only 0.47% had a diagnosis of persistent toe walking.4
Toe walking is a bilateral gait abnormality in which a normal heel strike/contact is absent and most weight bearing throughout stance phase of gait is on the forefoot.5 It is often observed in standing as well as during sitting. Toe walking by itself is described as Idiopathic Toe Walking (ITW, without a known reason).6 Here we focus on toe standing and walking behavior (also referred to as Toe-Walking Behavior or TWB), a better term which describes this phenomenon as extending beyond just walking.

Figure 5. Note Contrapposto posture with left leg carrying most of the weight.
In ASD, restricted and repetitive behaviors (RRBs) are defined as a series of behaviors and activities or interests that manifest regularly and interfere with daily functioning.6 Studies have shown that there is a clear relationship between RRBs and emotional states among individuals with ASD, as RRBs have been linked to anxiety and stress.
Although toe walking is not described specifically as such in the original The Repetitive Behavior Scale for Early Childhood (RBS-EC),7 it is described as such in the Diagnostic and Statistical Manual of Mental Disorders – 5 TR™ under the item Repetitive Motor definition: consecutive, non-social movements or actions that are repeated in a similar manner. And it is measured as:
0 – behavior does not occur
1 – behavior occurs about weekly or less
2 – behavior occurs several times a week
3 – behavior occurs about daily
4 – behavior occurs many times a day
What Happens During TWB?
Toe-walking behavior is most often or eventually accompanied by shortening of the calf muscle and other lower extremity soft tissues which further increases toe walking and the habitual standing habit. During initial gait phase, the lack of use of ankle dorsiflexion ROM leads to lack of heel contact (or as some describe it, strike), which further contributes to TWB.8 Research shows that there is a relationship between persistent toe walking and the development of ankle limitation in ROM into dorsiflexion which is needed in standing and walking. Persistent TWB in individuals with ASD is related to the shortening of the Achilles Tendon (AT), which leads to a decrease of ankle ROM in dorsiflexion.9 However, it is not clearly understood why some individuals with ASD develop a decrease of ankle ROM in dorsiflexion while others do not.
Calf muscles, especially the gastrocnemius muscle, which is a 2-joint or biarticular muscle, have a role to elongate during the stance phase of gait. Passive insufficiency occurs when an antagonist muscle, in this case the gastrocnemius, is unable to relax and elongate.10 The foot/ankle complex may compensate in various ways for the limited ability to stand and walk with heel touching the ground. As a child matures and gains weight, this limitation may cause pain, discomfort, and even calluses. In adults, it is exhibited by distortions of the foot and ankle complex due to weight, lack of passive elongation flexibility, or weakness (Figure 7). The result is a foot and ankle that are prone to pain, injury, and distortion. This may explain resistive unusual behavior or refusal to continue walking after a short distance.

Figure 6. NA) sitting in abduction with external rotation and feet hanging in plantar flexion; this positioning is often translated into B) standing and C) walking; note the position of the knee and subtalar joint in the side view C).
Most families and some therapists are not aware that individuals who have TWB need to be followed throughout the life span. Insurance companies most often will cover an annual evaluation and will allow for custom orthotics where the condition warrants it so proper support will be provided for the foot/ankle. This support will prevent deformity and instability and allow for continuous proper and safe ambulation. For a brace or device or a brace above the ankle, the coverage is more challenging as the reimbursement is every 5 years unless there is dire need and proper justification.
Can One Outgrow TWB?
It is erroneous to think that TWB will be resolved overtime, on its own. We see in the clinic mostly adults with foot/ankle deformities that result from early non- or limited intervention and follow-up to their TWB. However, even young adults who are considered “grown out” of their TWB may only “appear” to have their heels down during gait. This “appearance” is often due to compensation to loss of the dorsiflexion range by pronation at the subtalar joint, abduction at the midtarsal joints. These young adult feet are now rolling over the medial longitudinal arch forcing the foot to rotate outward. When this compensation continues, over time it becomes rigid, and the result is pressure at the medial aspect of the foot causing redness and eventually even skin irritation and callus. This can lead to difficulty in tolerating shoeware and even barefoot walking.
We recently saw a 4-year child with TWB whose feet were severely pronated and everted. Sadly, the treating therapist had told the mother, “Oh, he is not toe walking as much anymore.” In our evaluation, we saw a similar scenario: a foot and ankle pronated and everted with feet externally pointed in standing and walking. This child needs to be treated by proper orthotic intervention and should be getting passive and active range of motion exercises and a full home exercise plan should be suggested to the circle of care.
In the presence of a Pes Planus type of foot/ankle with hypermobility and muscle weakness or when the foot architecture is more rigid such as of Pes Cavus, TWB may persist into adulthood. TWB may appear slightly reduced due to the weight of the adult body. In the clinic, we still see some adults with TWB with mild to severe foot and ankle deformities.
A Pes Planus foot where there is hypermobility and a loss of the dynamic and static support structures will result in an incrementally worsening plano-valgus deformity.11 So, will children grow out of TWB? That answer is murky at best. Rather, what we see is that with time, the body compensates by pronating and distorting the foot/ankle complex.

Figure 7. These images show outcome of uncorrected toe walking in adulthood (2 different individuals in different age groups). Pronation of subtalar joint, abduction of midtarsal joint and hallux abductis valgus. Without proper bracing, damage will continue to allow soft tissues to shorten, which will lead to improper alignment making the condition into a deformed and permanent condition. This is why lifelong therapy is necessary.
Does this happen in walking? In the stance phase of the gait cycle an increased foot pronation negatively influences lower extremity sagittal plane biomechanics. Foot pronation increases foot segments’ hypermobility and compromises foot lever-arm function during the stance of gait.12 The joints in the foot distort when they need to be rigid causing an inefficiency in walking. Indeed, adults with a history of TWB often report clinical complaints of foot pain or of limited ambulation ability.
Mammal Locomotion Patterns
When trying to understand reasons for TWB, we can look at locomotion of terrestrial mammals which can be classified into 3 types based on contact with the ground (Figure 8). When moving, plantigrade animals keep the heel bone on the ground while digitigrade animals move using only the digits (metatarsals) to touch the ground. Unguligrade mammals walk and run on the tip of digits. Plantigrade is important for stability of body while the 2 other types help produce power, depending on moving speed.13 This can be interpreted as TWB producing muscle activity to gain power; however, in fact, this type of walking reduces stability in standing and walking.
Treatment Options
When the TWB persists, at any age, treatment options include both conservative and surgical management. Nonsurgical managements are often used as first resort and if not successful, in some cases a surgical approach is considered. Most treatment options focus on improving ROM through stretching and serial casting, gait retraining, botox injections, and bracing treatment. Surgical lengthening at either the Achilles Tendon or gastrocnemius level is aimed at improving ankle ROM. Even when the surgery option is applied, the conservative approach is required to ensure positive result:14
- Serial casting to improve ROM.
- Referral to podiatry for biomechanics analysis and assess skin integrity.
- Special shoes and braces – many options from soft garments such as Thera Togs to Sure Step SMO orthotics, or AFOs rigid or hinged. The aim here is to limit the ability to TWB and to allow a person to start placing weight on their heels.
- Physical therapy focusing on enhancing ROM, attention to an improved posture, strength, and gait training. Attention to posture and support to heels when sitting.
- Occupational therapy – focusing on sensory processing and integration.
- Botox Injections: the aim here is to reduce the ability of active plantar flexion.
- Surgery: various aims but mostly to elongate short soft tissue.

Figure 8. Locomotion of terrestrial mammals.
Research conducted in 2014 found that there was no single treatment option reported as having a long-term effect on the gait of children with ITW; it’s important to note, however, that this study was not limited to ASD.15 Another research study from 2016 focused on TW in individuals with ASD reported the lack of and the need for a structured quantitative test to assess TW in individuals with ASD.16
Some suggestions in addition to what was mentioned above:
- Consider and view toe walking and standing behavior as a habit. Merriam Webster’s defines a habit as “an acquired mode of behavior that has become nearly or completely involuntary.”
- To change a habit means to replace small repeatable, sustainable changes.
- Review first-hand experience reports of individuals with ASD (as noted earlier). One report says: “Lack of grounding or a kind of flowing in a river floating along and there’s no ground there’s no support, no stability no firm foothold grounding”
Understanding these first-hand experiences of individuals with ASD would call for adding 4 important elements to therapy:
- Creating an environment for the (individual’s) body to feel a sense of stability and grounding.
- Focusing awareness on bodily sensation by adding support such as boxes, sandbags, and therapist manual guidance. Feet planted on the ground – heel in full contact in sitting. If chair is too high, consider placing a stool under the feet.
- Relaxation by staying in a position well supported and attending to breath.
- Repetition of the same practice routine to create proper habit.

Figure 9. Shoulder and pelvis on the same side are in opposite direction
How To Start
- Observe and write or draw a list of postural issues that you see when an individual is sitting, standing, and walking both with shoes and barefoot.
Sample list of observed issues:
a. Weight bearing on left lower extremity more than the right
b. External rotation of lower extremities – origin is from hip
c. Shoulder and pelvis on the same side are in opposite direction (Figure 9) - Repeat this observation step every time you see the individual. This will give your observation credence depicting intra-rater reliability, a statistics term which means the degree of agreement among repeated tests performed by a single rater.
- Start thinking of therapy: Share with the individual, their teacher, or caregiver what you see and listen to what they say about what they see and what is their concern.
- Draw or write down the therapy program, share it with the individual, caregivers, and teachers. The attached drawing will explain some positioning and exercises to practice. Stay with a limited number of exercises, keep their order, and repeat them during sessions. Refine but stay with the same groupings.
What About Our Case Study, Anka?
The disappointment that we experienced comes from the fact that Anka does not use the braces all the time as suggested. Usually, she comes to our clinic with her PLS AFOs on her feet and when we remove them, she still walks with her heels on the ground when barefooted. At home she is without her braces and indeed she goes back to TWB. The benefit from the wear of braces is that she has proper range of motion and has the ability to lower her heel down. We are also disappointed that she does not receive PT at school. We realize it is a difficult task for families to take over the role of the therapist; however, we always encourage, provide, guide, and rehearse a limited Home Exercise Program with the individual’s circle of care. We are aware though that often the family is already overwhelmed by the patient’s other needs. The revisits and the specific drawing of exercises, or images, allow us to follow the progress and prevent unnecessary changes to the foot and body posture as a whole.
Behavioral Challenges
There is no doubt that working with individuals with behavioral issues can be difficult but understanding their needs, as evidenced in the first-hand experience reported above, certainly helps us to serve our patients as best as we can. Research is clear that attending to postural and walking difficulties should start early and continue throughout the life span. We all have a role to play in making sure that happens.
Dalia Zwick, PT, PhD, is Clinical Supervisor and Physical Therapist, at the PT, P&O clinics at Premier HealthCare & YAI Center for Specialty Therapy, NYC. Contact her at
Da*********@*ai.org.
- [Anonymous]. Why is it that people with ASD tend to have bad posture. Quora.com. Available at https://www.quora.com/Why-is-it-that-people-with-ASD-tend-to-have-bad-posture-What-is-a-good-way-for-them-to-improve-their-posture. Accessed Sept. 15, 2024.
- Zwick D. Clinical Perspective: Assessing Relaxed Standing Alignment and Posture in Autism Spectrum Disorder. Lower Extremity Review. 2020;3:41-48.
- Sala DA, Shulman LH, Kennedy RF, Grant AD, Chu ML. Idiopathic toe-walking: a review. Dev Med Child Neurol. 1999;41(12):846-8. doi: 10.1017/s0012162299001681.
- Leyden J, Fung L, Frick S. Autism and toe-walking: Are they related? Trends and treatment patterns between 2005 and 2016. Journal of Children’s Orthopaedics. 2019;13(4):340-345. doi:10.1302/1863-2548.13.180160
- Glod M, Riby DM, Rodgers J. Relationships between sensory processing, repetitive behaviors, anxiety, and intolerance of uncertainty in autism spectrum disorder and Williams syndrome. Autism Res. 2019;12(5):759–765. doi: 10.1002/aur.2096.
- Wolff JJ, Boyd BA, Elison JT. A quantitative measure of restricted and repetitive behaviors for early childhood. J Neurodev Disord. 2016;8:27. doi: 10.1186/s11689-016-9161-x.
- Wolff JJ, Boyd BA, Elison JT. The Repetitive Behavior Scale for Early Childhood (RBS-EC). Available at https://www.cehd.umn.edu/edpsych/research/resources/rbs-ec/. Accessed Sept. 1, 2024.
- Sobel E, Caselli MA, Velez Z. Effect of persistent toe walking on ankle equinus. Analysis of 60 idiopathic toe walkers. J Am Podiatr Med Assoc. 1997;87(1):17-22. doi: 10.7547/87507315-87-1-17.
- Valagussa G, Balatti V, Trentin L, Piscitelli D, Yamagata M, Grossi E. Relationship between tip-toe behavior and soleus – gastrocnemius muscle lengths in individuals with autism spectrum disorders. J Orthop. 2020 Aug 20;21:444-448. doi: 10.1016/j.jor.2020.08.013.
- Houghlum PA, Bertoti DB. Brunnstrom’s Clinical Kinesiology. 6th Ed. FA Davis Company. ©2011.
- Richie D. Biomechanics and Orthotic Treatment of the Adult Acquired Flatfoot. Clin Podiatr Med Surg. 2020;37(1):71-89. doi: 10.1016/j.cpm.2019.08.007.
- Resende RA, Pinheiro LSP, Ocarino JM. Effects of foot pronation on the lower limb sagittal plane biomechanics during gait. Gait Posture. 2019;68:130-135. doi: 10.1016/j.gaitpost.2018.10.025.
- Wada N. Mammal’s Locomotion. 4th Version. Revised Feb. 6, 2023. Available at https://mammals-locomotion.com/walking.html. Accessed Sept. 1, 2024.
- Bauer JP, Sienko S, Davids JR. Idiopathic Toe Walking: An Update on Natural History, Diagnosis, and Treatment. J Am Acad Orthop Surg. 2022;30(22):e1419-1430. doi: 10.5435/JAAOS-D-22-00419.
- Williams CM, Tinley P, Rawicki B. Idiopathic toe-walking: have we progressed in our knowledge of the causality and treatment of this gait type? J Am Podiatr Med Assoc. 2014;104(3):253-62. doi: 10.7547/0003-0538-104.3.253.
- Valagussa G, Trentin L, Signori A, Grossi E. Toe Walking Assessment in Autism Spectrum Disorder Subjects: A Systematic Review. Autism Res. 2018;11(10):1404-1415. doi: 10.1002/aur.2009.






The horrid way in which you have pathologised and othered autistic behaviors as if neurotypical postures and socialisation of body behaviors are the most perfect, most natural and somehow standard precendent overshadows the good work you’re putting in. I wish you were able to see autistic bodies behaving as is best suited for themselves and tried to help us adjust better to a world not designed for us rather than encouraging the narrative that there is something innately wrong with us which you must fix. I fear for fellow autists who have be around the kind of language and preconcieved notions you have for us.
@Sheena
Good lord. This website has extensive experience working with people with gait issues. Noticing commonalities amongst people with autism isn’t a bad thing. It could help people from having serious concerns in their future. Have you even considered that these academic individuals typically must specialize in their studies and treatment and that’s why this particular site focuses on autism? The language used here, like “behaviors” is a clinical term for all PT patients. Their goal is fix a behavior – slouching, injuries whatever, it’s a medical term!
Have you witnessed or helped an old person with the long term side effects of these conditions? It’s awful- they’re in pain, they have more injuries that can become life threatening or at least affect their quality of life. You have to look further down the line here regarding current practices that may feel fine now but will develop into something life altering in the future.
Did you consider that linking pronation with autism may help people get physical treatment they otherwise may not be able afford or have access to? That’s incredibly important to realize- medical treatment requires scientific research to support it, often a requirement with medical insurance. They clearly point this out in the article.
Lastly, You don’t speak for all people with autism, like my father- whose gait issues caused a debilitating fall at age 68 that led to paralysis and head trauma, or myself or my child who benefits from PT at school due to studies like these. Speak for yourself please
Sheena: Thank you for your comment. I wrote this article from the perspective of a physical therapist who works with individuals who, over time, lose their ability or desire to stand or walk due to postural challenges. My goal is to help prevent some of these consequences before they become harder to manage.
I recognize that some of the language I used may have come across as pathologizing, and I regret that. I fully respect that individuals know what works best for their bodies, and my intention was never to suggest that neurotypical behavior is the ideal.