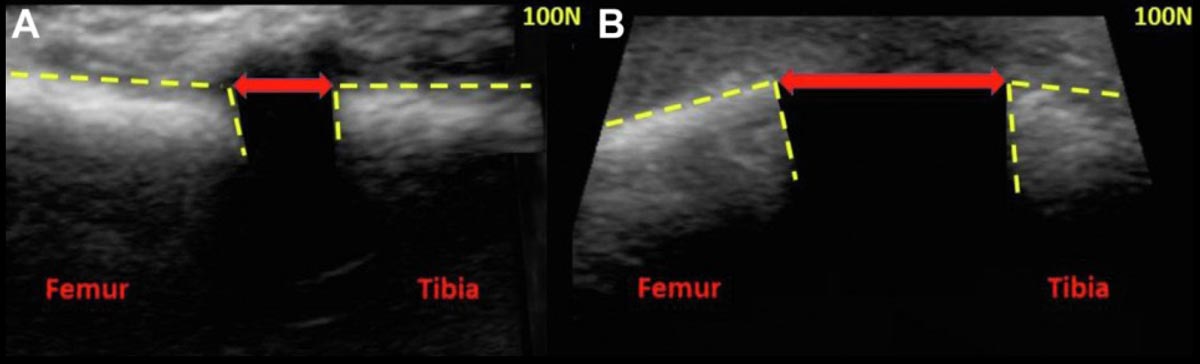
Figure. Ultrasound images of the medial compartment of the left knee taken at 20° of flexion with a portable ultrasound probe positioned perpendicular to the medial joint line over the medial collateral ligament. The medial tibiofemoral distance was calculated by measuring the distance between the articular margins (indicated by dashed yellow lines) of the medial femoral condyle and the medial tibial plateau. (A) Ultrasound image demonstrating medial tibiofemoral distance under 100 N of valgus force in an intact knee. (B) Ultrasound image demonstrating increased medial tibiofemoral distance under 100 N of valgus directed force after transection of the deep medial collateral ligament and posterior oblique ligament.
The purpose of this cadaveric study was to quantify the severity of medial knee injuries based on medial compartment gapping as measured by stress ultrasonography.
Methods: In 8 cadaveric knees, the distance between the medial tibial and femoral condyles was measured using ultrasonography. These measurements were obtained in the intact state and repeated after open sequential transection of the superficial medial collateral ligament (sMCL), deep medial collateral ligament (dMCL), posterior oblique ligament (POL), and arthroscopic transection of the anterior cruciate ligament (ACL). Knees were evaluated at 0° and 20° of knee flexion using the Telos device under 0 N and 100 N of valgus force. Receiver operating characteristic curve analysis and the DeLong test were used to determine whether measurements could distinguish between successive severity of MCL injury after identifying the optimal cutoff value for each injury state.
Results: Of the 8 cadaveric knees in this study, 3 were male and 5 were female; mean age was 58 ± 11 years (range 48–82 years). When measured using ultrasonography at 20° knee flexion with valgus load, the medial tibiofemoral distance significantly increased with increasing severity of medial knee injury (P values ranging from .049 to <.001). Optimal cutoff values for distinguishing between an intact knee and sMCL injury were 8.3 mm (area under the curve [AUC] = 0.98), between sMCL and dMCL injury 9.9 mm (AUC = 0.89), dMCL and POL 16.7 mm (AUC = 0.88), and POL and ACL 18.6 mm (AUC = 0.84). When the study authors compared combined intact and sMCL-transected stages with dMCL-transected stage, optimal cut-off point to differentiate stable from unstable injuries was equal to13.8 mm of medial tibiofemoral distance (AUC = 0.97; sensitivity = 100%; specificity = 94.1%).
Conclusions: Dynamic ultrasonographic assessment can accurately quantify the severity of medial knee ligament injury based on medial compartment gapping without the need for radiation and at point of care in multiple clinical settings. This study found medial tibiofemoral distance >13.8 mm at 20° knee flexion under valgus force indicates the presence of dMCL injury with a diagnostic accuracy of 0.97.
Source: Bhimani R, Lubberts B, DiGiovanni CW, Tanaka MJ. Dynamic ultrasound can accurately quantify severity of medial knee injury: a cadaveric study. Arthrosc Sports Med Rehabil. 2022;4(5):e1777-e1787.





