
iStockphoto.com 493249207
Using patient-reported outcome tools can give lower extremity clinicians insight into the disability experienced by patients with chronic ankle instability. A combination of instruments may be necessary, as different assessments may capture different aspects of the condition.
By Adam B. Rosen PhD, ATC; and Cathleen N. Brown PhD, ATC
Lateral ankle sprains are the most common athletic injury and account for more than 7% of all injuries reported in collegiate sports.1 Repetitive sprain can lead to an increased risk of ankle joint osteoarthritis and to a debilitating condition known as chronic ankle instability (CAI).2 CAI is characterized by episodes of “giving way, ” is associated with poorer quality of life than in those who have never sprained their ankle, and is difficult to manage for the sports medicine clinician.3 There is no consensus on the exact causes of CAI, however, multiple factors are thought to contribute.4,5 These factors include both mechanical and functional deficits, which decrease the capacity of the individual to control the ankle joint during dynamic movement.4
Recognition and classification of CAI is challenging for sports medicine clinicians, as no gold-standard clinical tests or imaging techniques exist to identify individuals with CAI.6 However, patient-reported outcome tools (PROs) or self-report questionnaires, combined with patient history, are the benchmarks most often used to assess CAI.6 For the sports medicine clinician, understanding the type of questionnaire being used and the aspects of dysfunction being assessed is paramount.
There are different types of PROs, ranging from generic health questionnaires such as the Short form-36 Health Survey to questionnaires that are specific to an anatomic region (eg, Knee Injury and Osteoarthritis Outcome Score [KOOS]), disease (eg, Cumberland Ankle Instability Tool [CAIT]), or dimension (eg, physical activity assessment).7 These instruments will provide the clinician with objective information regarding the patient’s current mobility, limitations, and health-related quality of life (HRQOL).7 Scores may also be used for goal-setting during rehabilitation to monitor progress and functional improvements.
As many self-report questionnaires are readily available and geared toward clinician implementation, users should be aware of each tool’s clinimetric properties and clinical utility, which may vary between tools. Moreover, several clinical factors have been identified as contributing to the disability perceived and the function reported by individuals with CAI.
Assessing self-reported function
A number of frequently used self-report questionnaires for ankle instability exist, each with differing clinical utility and varying levels of support.7,8 This review focuses on region- and disease-specific tools for CAI or functional ankle instability. We selected these tools based on their common usage, endorsement by the International Ankle Consortium (IAC),6 and the evidence to support their use. We have included both discriminative instruments that identify individuals with a specific pathology like CAI, and evaluative instruments that quantify an individual’s perceived level of function.7 We will not discuss dimension-specific or generic tools, though those have been discussed by Houston et al7 and elsewhere.
The tools highlighted are summarized below, and key characteristics are reported in Table 1. The table includes basic information on scoring and interpretation, validity and reliability, and clinical utility where available.
Construct validity, or comparison to a gold standard, is reported, as are test-retest and/or internal consistency. Test-retest is commonly reported as an intraclass correlation coefficient (ICC), where greater than .8 is generally considered good to excellent reliability. Internal consistency between the questions is reported as Cronbach’s alpha, where greater than .7 is generally acceptable. Not all measures of validity and reliability in the literature were reported in the table.
 Clinical utility is reported from original studies, secondary analysis, or as calculated from tabled data. Sensitivity, the ability of the test to correctly identify patients with the disease, and specificity, the ability of the test to correctly identify patients without the disease, are reported.9 Generally higher values are better (>.8), but not always, and values may be interpreted in relation to one another.9
Clinical utility is reported from original studies, secondary analysis, or as calculated from tabled data. Sensitivity, the ability of the test to correctly identify patients with the disease, and specificity, the ability of the test to correctly identify patients without the disease, are reported.9 Generally higher values are better (>.8), but not always, and values may be interpreted in relation to one another.9
Likelihood ratios provide information for the probability a person with a given test result does have the condition.9 Positive likelihood ratio (LR+) values greater than 10 represent large and important shifts in probability and are meaningful, while values of 5-10 are moderate shifts in probability and are probably meaningful.9 Values less than 5 are likely not clinically meaningful.9 Negative likelihood ratio (LR-) values less than .1 represent large and important shifts in probability and are meaningful. Values of .1-.2 represent medium shifts in probability and are probably meaningful, while values greater than .3 are likely not clinically meaningful.9
Minimal detectable change (MDC) is the smallest change value needed to surpass measurement variability, while minimal clinically important difference (MCID) is the smallest change value patients report as beneficial.7 Not all clinimetric values were available in the literature for all instruments reported in this review.
Assessment tools
The Ankle Instability Instrument (AII) was designed specifically to determine ankle instability. It captures the severity of the initial injury, history of ankle instability, and instability during activities of daily living (ADLs).10 It has good test-retest reliability and is endorsed by the IAC,6 but little evidence exists detailing its clinical utility. The sensitivity and specificity values are good, but likelihood ratios may not be meaningful.
The Ankle Joint Functional Assessment Tool (AJFAT) compares limbs bilaterally, thus assuming unilateral instability in the patient.11 There is limited evidence for clinical utility,12 but it may be responsive to treatment/rehabilitation interventions.
The CAIT was developed to identify and quantify the degree of instability and assess each ankle independently.13 It has good validity and reliability values. The IAC has recommended lowering the initial cut-point from 27.513 to 2514 to 24.6 The CAIT’s sensitivity and specificity show good clinical utility, but the likelihood ratios are only moderate.
The Foot and Ankle Ability Measure (FAAM) and its Sport subscale (FAAM-S)15 are refinements of the Foot and Ankle Disability Index (FADI) and its Sport subscale (FADI-S), which are described in the next paragraph.16 The FAAM focuses on ADLs and sports, and has five fewer questions than the FADI and FADI-S. Points are scored numerically but converted to a percentage. It has good evidence for validity and reliability, but only moderate clinical utility. MDC and MCID values exist for both subscales. The IAC has endorsed it with cut-off scores,6 and it is likely responsive to treatment/rehabilitation interventions.8,15
The FADI is the original version of the FAAM, including one sleep-related question and four pain-related questions that were dropped when creating the FAAM.16 It has ADL and Sport subscales, and each limb is scored separately and converted to a percentage. It displays moderate to good reliability depending on the scale, MDC values are available,17 and it may be responsive to treatment/rehabilitation interventions. Most researchers currently support use of the FAAM over the FADI.6
The Foot and Ankle Outcome Score (FAOS) is a longer questionnaire with five areas: pain, other symptoms, ADLs, sport/recreational function, and foot/ankle quality of life.18 Scores are transformed to a percentage. It demonstrates good reliability and internal consistency and moderate clinical utility, and is endorsed by the IAC with cut-off values.6,8

The Identification of Functional Ankle Instability (IdFAI) was developed from the AII and CAIT.19 It has good clinical utility,20 but MDC and MCID values do not appear to be available.
With regard to region-specific HRQOL outcomes, a systematic review indicated consistent results across 27 studies for the FAAM, FADI, CAIT, and AJFAT.7 Individuals with CAI consistently scored lower than uninjured controls and copers (individuals who had an ankle sprain but recovered).7 Comparison of copers and controls is not as clear or consistent.
Clinical contributions
Although much knowledge has been derived from these questionnaires regarding CAI patients’ quality of life, less is known about which clinical factors contribute to reports of decreased function.
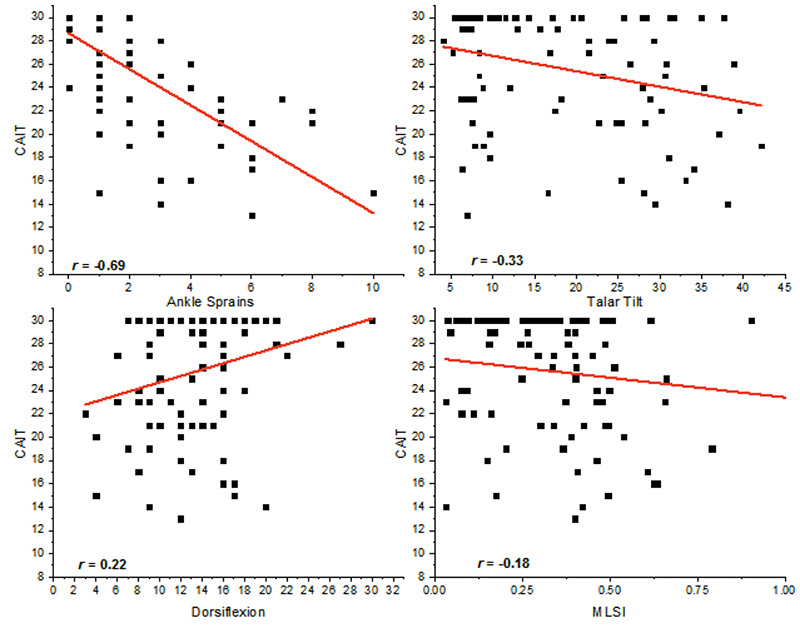
Figure 1. Scatter plots of individual factors that contribute to the Cumberland Ankle Instability Tool: ankle sprain history (top left); inversion laxity talar tilt (top right); dorsiflexion range of motion (bottom left); Medial Lateral Stability Index (bottom right).
Several studies have investigated clinical measures and their contributions to self-reported function as indicated by PROs, both individually and through multivariate analyses. These studies assess a range of factors and their relationships with various instrumented questionnaires.
For example, Hubbard and colleagues21 evaluated the FADI and FADI-S in 30 individuals with CAI while also measuring a number of clinical measures including fibular position, an ankle arthrometer assessment of laxity, static and dynamic postural stability, isokinetic ankle and hip strength, and dynamic balance based on the Star Excursion Balance Test. The authors found that the FADI and its Sports subscale demonstrated moderate correlations with center of pressure measures during eyes-open and eyes-closed balance, indicating those with poorer function also had worse static balance. In a subsequent study by Hubbard,22 mechanical laxity and the FADI and FADI-S were evaluated in 120 participants with unilateral CAI. Anterior laxity was strongly to moderately correlated (r = -.88) with the FADI and FADI-S (r = -.65), while inversion talar tilt was moderately correlated with the FADI (r = -.53) and FADI-S (r = -.45). These results suggest that increased laxity, especially anteriorly, may contribute to the perceived dysfunction reported by patients with CAI.
With regard to multivariate analysis, only two manuscripts have been published, one by our research team23 on the CAIT, and another by Houston et al24 that investigated several health-related quality of life measures.
Our study assessed 93 individuals with varying histories of ankle injury. Injury history, range of motion, dynamic postural stability, and laxity were taken for each of the participants. We found a history of lateral ankle sprain had the greatest influence on CAIT score, followed by laxity, dorsiflexion deficits, and medial-lateral dynamic postural stability, respectively (Figure 1). Combined, these variables accounted for 57% of the variability of the CAIT. This suggests those who report greater numbers of sprains report worse function, and that increased laxity, worse dynamic postural stability, and less dorsiflexion also contribute to perceived dysfunction, but to a lesser extent than injury history.
In the other study to include a multivariate assessment, Houston et al24 evaluated isometric strength, static and dynamic balance, plantar cutaneous sensation, dorsiflexion range of motion, and laxity in 40 individuals with CAI. They examined these measures against four different self-report questionnaires; the Short Form-12 (both mental and physical components), Disablement in the Physically Active Scale (DPA), Fear-Avoidance Beliefs Questionnaire (FABQ), and FAAM. Of the clinical measures assessed, static and dynamic postural control, dorsiflexion ROM, plantar cutaneous sensation, and laxity explained between 7% and 35% of the variability in PRO scores, depending on the questionnaire. More specifically, worse postural control, sensation, dorsiflexion, and laxity explained a significant portion of health-related quality of life in individuals with CAI.
Clinical implications
Using PROs can provide insight into the disability a patient with CAI experiences. For the sports medicine clinician, choosing an appropriate PRO or questionnaire to assess disability or for rehabilitation monitoring can be a daunting task, as many are available.
In this review, we have highlighted several useful tools with moderate to excellent clinical utility that are easy for clinicians working with CAI patients to administer and interpret, and may be responsive to change over the course of a rehabilitation program. The FAAM likely has the best clinimetric properties overall, but the CAIT, IdFAI, FAOS, and AII are all good alternatives. The IdFAI is a well-supported combination of two measures.25 A combination of instruments may be necessary, as performance on one may be different than on another, and different assessments may capture different aspects of the condition.7,8,17
In addition to the utilization of PROs, understanding the factors that contribute to perceived dysfunction will allow sports medicine clinicians to more effectively treat patients with CAI. Reduced dorsiflexion ROM has been consistently related to dysfunction, indicating that improving ROM may have beneficial effects on self-reported function. Interventions such as joint mobilizations26-28 and static stretching29 have demonstrated robust improvements in dorsiflexion ROM.
Prior work also suggests preventive strategies that aim to reduce future sprains should be emphasized. Bracing and taping interventions may provide multiple benefits to those with CAI to assist in reducing the deleterious effects of mechanical laxity through altered arthrokinematics, as well as providing a secondary benefit of reducing the risk of future ankle sprain.30 Given that both static and dynamic balance demonstrated small to moderate significant correlations with self-reported functional limitations, incorporating balance protocols into rehabilitation and preventive programs appears fundamental.31
The literature on patient-reported outcomes also underscores the concept that each individual with CAI may report a different combination of decreased functional ability and clinical measures. Because CAI is a multifactorial problem affecting a heterogeneous population, providing a comprehensive treatment plan may be necessary to improve individual patient outcomes.
Adam B. Rosen PhD, ATC, is an assistant professor in the School of Health, Physical Education and Recreation at the University of Nebraska at Omaha. Cathleen N. Brown PhD, ATC, is a clinical associate professor in the Department of Athletic Training and Kinesiology at Oregon State University in Corvallis.
- Roos KG, Kerr ZY, Mauntel TC, et al. The epidemiology of lateral ligament complex ankle sprains in National Collegiate Athletic Association sports. Am J Sports Med 2017;45(1):201-209.
- Valderrabano V, Hintermann B, Horisberger M, Fung TS. Ligamentous posttraumatic ankle osteoarthritis. Am J Sports Med 2006;34(4):612-620.
- Hubbard-Turner T, Turner MJ. Physical activity levels in college students with chronic ankle instability. J Athl Train 2015;50(7):742-747.
- Hiller CE, Kilbreath SL, Refshauge KM. Chronic ankle instability: evolution of the model. J Athl Train 2011;46(2):133-141.
- Doherty C, Bleakley C, Hertel J, et al. Recovery from a first-time lateral ankle sprain and the predictors of chronic ankle instability: A prospective cohort analysis. Am J Sports Med 2016;44(4):995-1003.
- Gribble PA, Delahunt E, Bleakley C, et al. Selection criteria for patients with chronic ankle instability in controlled research: a position statement of the international ankle consortium. J Orthop Sports Phys Ther 2013;43(8):585-591.
- Houston MN, Hoch JM, Hoch MC. Patient-reported outcome measures in individuals with chronic ankle instability: a systematic review. J Athl Train 2015;50(10):1019-1033.
- Donahue M, Simon J, Docherty CL. Critical review of self-reported functional ankle instability measures. Foot Ank Int 2011;32(12):1140-1146.
- Fischer JE, Bachmann LM, Jaeschke R. A readers’ guide to the interpretation of diagnostic test properties: clinical example of sepsis. Intensive Care Med 2003;29(7):1043-1051.
- Docherty CL, Gansneder BM, Arnold BL, Hurwitz SR. Development and reliability of the ankle instability instrument. J Athl Train 2006;41(2):154-158.
- Rozzi SL, Lephart SM, Sterner R, Kuligowski L. Balance training for persons with functionally unstable ankles. J Orthop Sport Phys Ther 1999;29(8):478-486.
- Wikstrom EA, Tilman MD, Chmielewski TL, et al. Dynamic postural control but not mechanical stability differs among those with and without chronic ankle instability. Scand J Med Sci Sports 2010;20(1):137-144.
- Hiller CE, Refshauge KM, Bundy AC, et al. The Cumberland Ankle Instability Tool: a report of validity and reliability testing. Arch Phys Med Rehabil 2006;87(9):1235-1241.
- Wright CJ, Arnold BL, Ross SE, Linens SW. Recalibration and validation of the Cumberland Ankle Instability Tool cutoff score for individuals with chronic ankle instability. Arch Phys Med Rehabil 2014;95(10):1853-1859.
- Martin RL, Irrgang JJ, Burdett RG, et al. Evidence of validity for the Foot and Ankle Ability Measure (FAAM). Foot Ankle Int 2005;26(11):968-983.
- Hale SA, Hertel J. Reliability and sensitivity of the Foot and Ankle Disability Index in subjects with chronic ankle instability. J Athl Train 2005;40(1):35-40.
- Eechaute C, Vaes P, Van Aerschot L, et al. The clinimetric qualities of patient-assessed instruments for measuring chronic ankle instability: a systematic review. BMC Musculoskel Dis 2007;8:6.
- Roos EM, Brandsson S, Karlsson J. Validation of the foot and ankle outcome score for ankle ligament reconstruction. Foot Ankle Int 2001;22(10):788-794.
- Simon J, Donahue M, Docherty C. Development of the Identification of Functional Ankle Instability (IdFAI). Foot Ankle Int 2012;33(9):755-763.
- Gurav RS, Ganu SS, Panhale VP. Reliability of the identification of functional ankle instability (IdFAI) scale across different age groups in adults. N Am J Med Sci 2014;6(10):516-518.
- Hubbard TJ, Kramer LC, Denegar CR, Hertel J. Correlations among multiple measures of functional and mechanical instability in subjects with chronic ankle instability. J Athl Train 2007;42(3):361-366.
- Hubbard-Turner T. Relationship between mechanical ankle joint laxity and subjective function. Foot Ank Int 2012;33(10):852-856.
- Rosen A, Ko J, Brown C. A multivariate assessment of clinical contributions to the severity of perceived dysfunction measured by the Cumberland Ankle Instability Tool. Int J Sport Med 2016;37(14):1154-1158.
- Houston MN, Hoch JM, Gabriner ML, et al. Clinical and laboratory measures associated with health-related quality of life in individuals with chronic ankle instability. Phys Ther Sport 2015;16(2):169-175.
- Simon J, Donahue M, Docherty CL. Critical review of self-reported functional ankle instability measures: a follow up. Phys Ther Sport 2014;15(2):97-100.
- Cruz-Diaz D, Lomas Vega R, Osuna-Perez MC, et al. Effects of joint mobilization on chronic ankle instability: a randomized controlled trial. Disabil Rehabil 2015;37(7):601-610.
- Delahunt E, Cusack K, Wilson L, Doherty C. Joint mobilization acutely improves landing kinematics in chronic ankle instability. Med Sci Sports Exerc 2013;45(3):514-519.
- Harkey M, McLeod M, Van Scoit A, et al. The immediate effects of an anterior-to-posterior talar mobilization on neural excitability, dorsiflexion range of motion, and dynamic balance in patients with chronic ankle instability. J Sport Rehabil 2014;23(4):351-359.
- Terada M, Pietrosimone BG, Gribble PA. Therapeutic interventions for increasing ankle dorsiflexion after ankle sprain: a systematic review. J Athl Train 2013;48(5):696-709.
- Doherty C, Bleakley C, Delahunt E, Holden S. Treatment and prevention of acute and recurrent ankle sprain: an overview of systematic reviews with meta-analysis. Br J Sports Med 2017;51(2):113-125.
- Kosik KB, McCann RS, Terada M, Gribble PA. Therapeutic interventions for improving self-reported function in patients with chronic ankle instability: a systematic review. Br J Sports Med 2017;51(2):105-112.





