
 By Mathias B. Forrester, BS
By Mathias B. Forrester, BS
Background: Stingray injuries may occur as a result of stepping on stingrays or while handling stingrays when fishing. Over 1,000 stingray injuries are estimated to occur in the United States (US) annually. The objective of this study was to characterize stingray injuries of the lower extremity treated at emergency departments (EDs).
Methods: An analysis was performed of stingray injuries of the lower extremity using data from the National Electronic Injury Surveillance System of the US Consumer Product Safety Commission during 2000-2021.
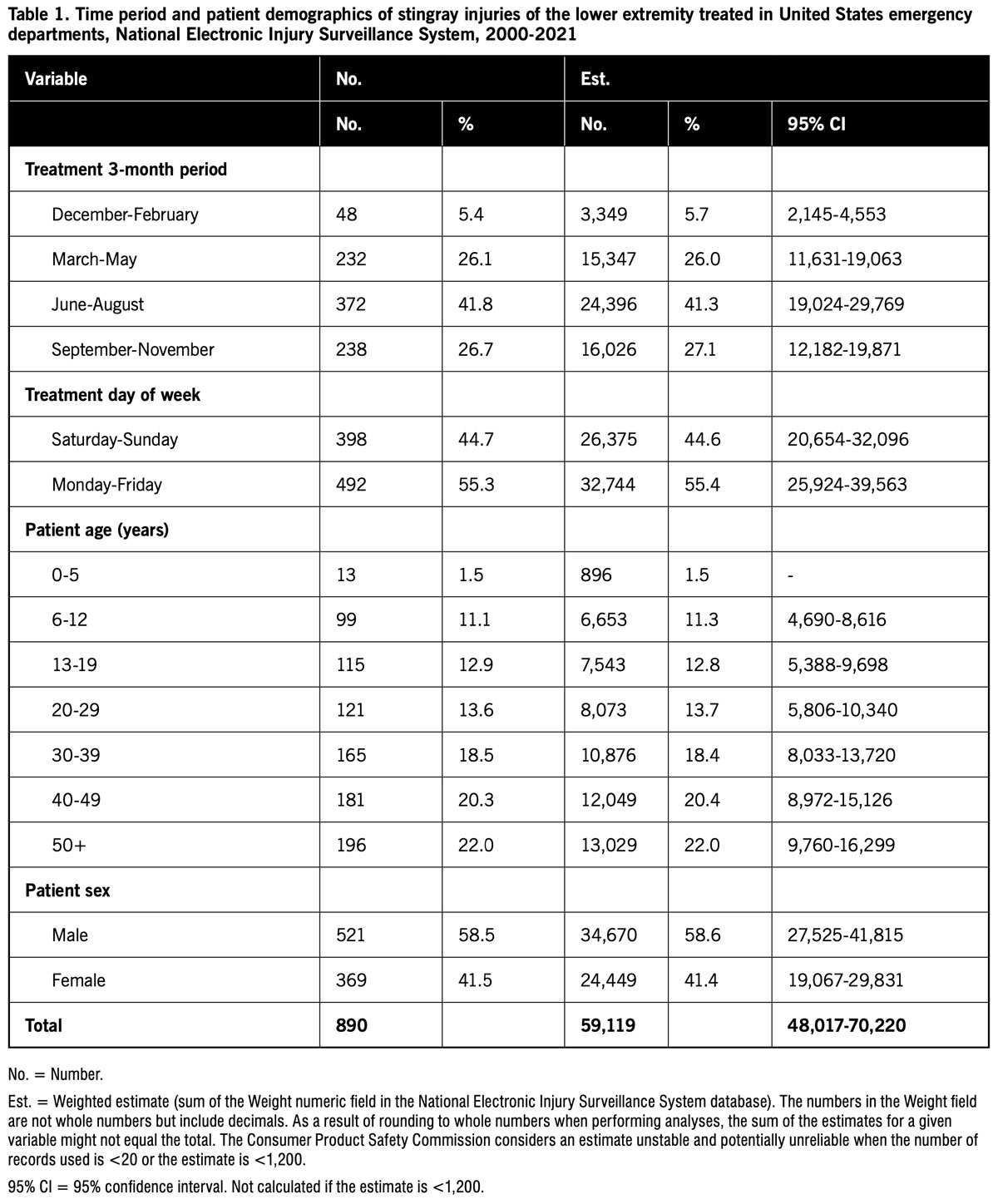
Results: An estimated 59,119 stingray injuries of the lower extremity treated at US hospital EDs during 2000-2021 were identified. The patient age was 1.5% 0-5 years, 11.3% 6-12 years, 12.8% 13-19 years, and 74.5% 20 years or older; 58.6% of the patients were male and 41.4% female. The most frequently reported activities associated with the injury were swimming (91.4%), fishing (4.5%), and surfing (2.4%). The distribution of injuries by 3-month period was 41.3% in June-August, 27.1% in September-November, 5.7% in December-February, and 26.0% in March-May. The affected body part was 89.8% foot, 3.7% toe, 3.6% ankle, 1.9% lower leg, 0.6% knee, and 0.4% upper leg. The patient was treated or examined in the ED and then released in 99.3% of the time.
Conclusions: Stingray injuries of the lower extremity most frequently occurred while swimming. The injuries were seasonal, most often occurring in the summer. The body part most often injured was the foot. The majority of patients were treated or examined and released from the ED.
Stingrays are cartilaginous fish related to sharks with round, flattened bodies and whip-like tails. Stingrays are common to shallow intertidal areas of tropical and subtropical oceans around the world, although some rays inhabit cooler waters and freshwater.1-5 While there are approximately 150 species of ray worldwide, one to two dozen stingray species are found along the United States (US) coasts.4,5
 Stingrays have one–three venomous barbed (serrated) blades (spines) on the dorsal aspect of their tails.2,3,5 Stingray venom contains cystatins, peroxiredoxin, and galectin;6 the toxicity varies by species.5 Stingrays typically are not aggressive and usually only attack when provoked.1 Stingray injuries may occur as a result of stepping on stingrays, usually affecting the lower extremities, or while handling stingrays when fishing, usually involving the upper extremities.1-4,7 Stingrays sting more people annually than any other fish, and it is estimated that over one thousand stingray injuries occur in the US annually.2,8
Stingrays have one–three venomous barbed (serrated) blades (spines) on the dorsal aspect of their tails.2,3,5 Stingray venom contains cystatins, peroxiredoxin, and galectin;6 the toxicity varies by species.5 Stingrays typically are not aggressive and usually only attack when provoked.1 Stingray injuries may occur as a result of stepping on stingrays, usually affecting the lower extremities, or while handling stingrays when fishing, usually involving the upper extremities.1-4,7 Stingrays sting more people annually than any other fish, and it is estimated that over one thousand stingray injuries occur in the US annually.2,8
Contact with a stingray blade may cause localized trauma (puncture wound or laceration), bleeding, intense pain, edema, and discoloration and may result in blistering, tissue necrosis, and secondary infection. 1-5,7,9,10 Systemic effects may include nausea, vomiting, diarrhea, headache, fever, chills, seizures, generalized edema, muscle cramping, tremors, weakness, limb paralysis, hypotension, bradycardia, convulsions, and syncope.1,2,4,5,7,9 Although uncommon, deaths have been reported from stingray injuries,1-4 notably that of wildlife expert Steve Irwin in 2006.11
The objective of this investigation was to describe stingray injuries of the lower extremity treated at US hospital emergency departments (EDs).
Methods
This study used data downloaded from the National Electronic Injury Surveillance System (NEISS) website at https://www.cpsc.gov/cgibin/NEISSQuery/home.aspx. The NEISS has been described in detail previously.12 Briefly, the NEISS collects data on consumer product-related injuries from the EDs of a stratified random sample of 100 US hospital EDs. NEISS coders view the medical charts at participating hospitals and, for patients with injuries that meet NEISS inclusion criteria, collect and code information such as treatment date; patient age, sex, and race; injury diagnosis and body part injured; discharge disposition; consumer product(s) involved in the injury; location where the incident occurred; and a brief narrative describing the incident.13-15 Since the data are publicly available and de-identified, the study is exempt from institutional review board approval.
Cases were stingray injuries of the lower extremity included in the NEISS database during 2000-2021. In order to identify cases, the Narrative text field (a brief summary of the circumstances of the injury) of all records was searched for any mention of both of the letter groups “sting” and “ray.” For the resulting subset of records, the narrative field was reviewed to determine whether the injury appeared to be due to a stingray. Cases were included in the study only if the Body_Part numeric field contained codes for a lower extremity body part (upper leg, knee, lower leg, ankle, foot, toe). An additional numeric field (Body_Part_2) collects information if a second body part was injured (or the same body part experienced a different type of injury). However, this field was added in 2019, so data in the Body_Part_2 field were excluded from the analysis. The two cases with a lower extremity coded in the Body_Part_2 field also had a lower extremity coded in the Body_Part field.
The variables examined were the time of treatment (year, three month period, and day of week), patient age and sex, location where the injury incident occurred, activity during which the injury occurred, type of injury, body part affected, and patient disposition. The activity during which the injury occurred was identified by review of the Narrative text field and Product_1, Product_2, and Product_3 numeric fields and grouped into the following categories: swimming, fishing, surfing, and other/unknown.
Analyses were performed using Office Professional 2007 Access and Excel (Microsoft Corporation, Redmond, Washington, US). The distribution of cases and national injury estimates were determined for the variables. National injury estimates were calculated by summing the values in the Weight numeric field in the publicly available NEISS database, and 95% confidence intervals (CIs) were calculated for the estimates. The CPSC considers an estimate unstable and potentially unreliable when the number of records used is <20 or the estimate is <1,200.13 For those variable subgroups where the estimate was <1,200, 95% CIs were not calculated.
Results
 There were a total of 890 stingray injuries of the lower extremity treated at a sample of US hospital EDs during 2000-2021, resulting in an estimated 59,119 (95% CI 48,017-70,220) such injuries (88.4% of the 66,894 total estimated stingray injuries of any body part). The estimated annual number of stingray injuries of the lower extremity was 15,558 in 2000, declining to 164 in 2021. The mean annual estimated number of injuries was 8,112 during 2000-2005, 1,152 during 2006-2011, 325 during 2012-2016, and 370 during 2017-2021.
There were a total of 890 stingray injuries of the lower extremity treated at a sample of US hospital EDs during 2000-2021, resulting in an estimated 59,119 (95% CI 48,017-70,220) such injuries (88.4% of the 66,894 total estimated stingray injuries of any body part). The estimated annual number of stingray injuries of the lower extremity was 15,558 in 2000, declining to 164 in 2021. The mean annual estimated number of injuries was 8,112 during 2000-2005, 1,152 during 2006-2011, 325 during 2012-2016, and 370 during 2017-2021.
Table 1 presents stingray injuries of the lower extremity by time period and patient demographics. The highest proportion of injuries were treated in June-August and the lowest proportion in December-February. Almost 45% of the injuries were treated on the weekend. The majority (74.5%) of patients were adults, and most patients were male.
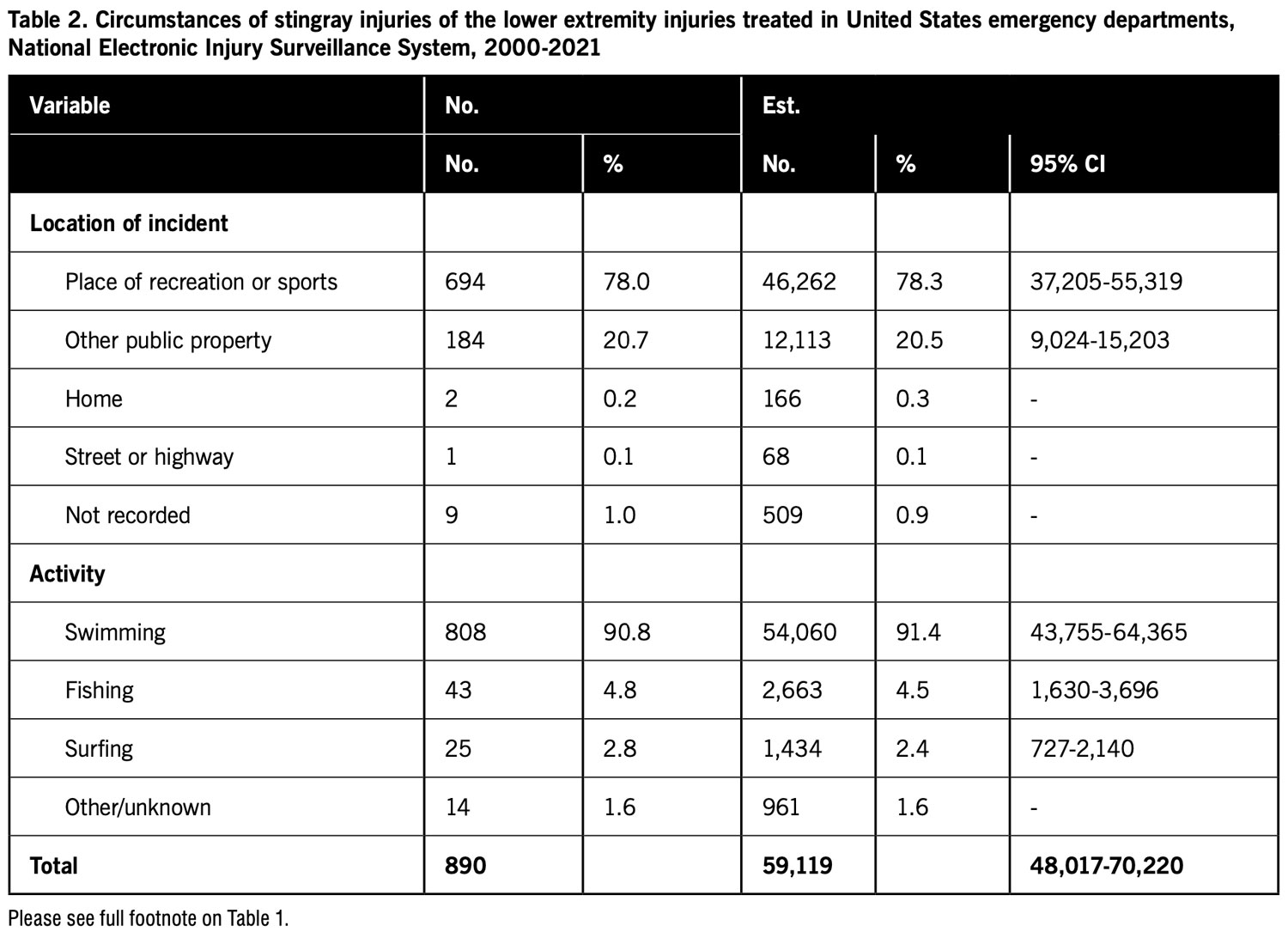
The majority of the injuries occurred at a place of recreation or sports or other public property, and most occurred while the patient was swimming (Table 2). Of the estimated 57,105 total stingray injuries of any body part that occurred while swimming, 54,060 (94.7%) involved the lower extremity. Of the estimated 7,191 total stingray injuries of any body part that occurred while fishing, 2,663 (37.0%) involved the lower extremity. All of the estimated 1,434 total stingray injuries that occurred while surfing involved the lower extremity.
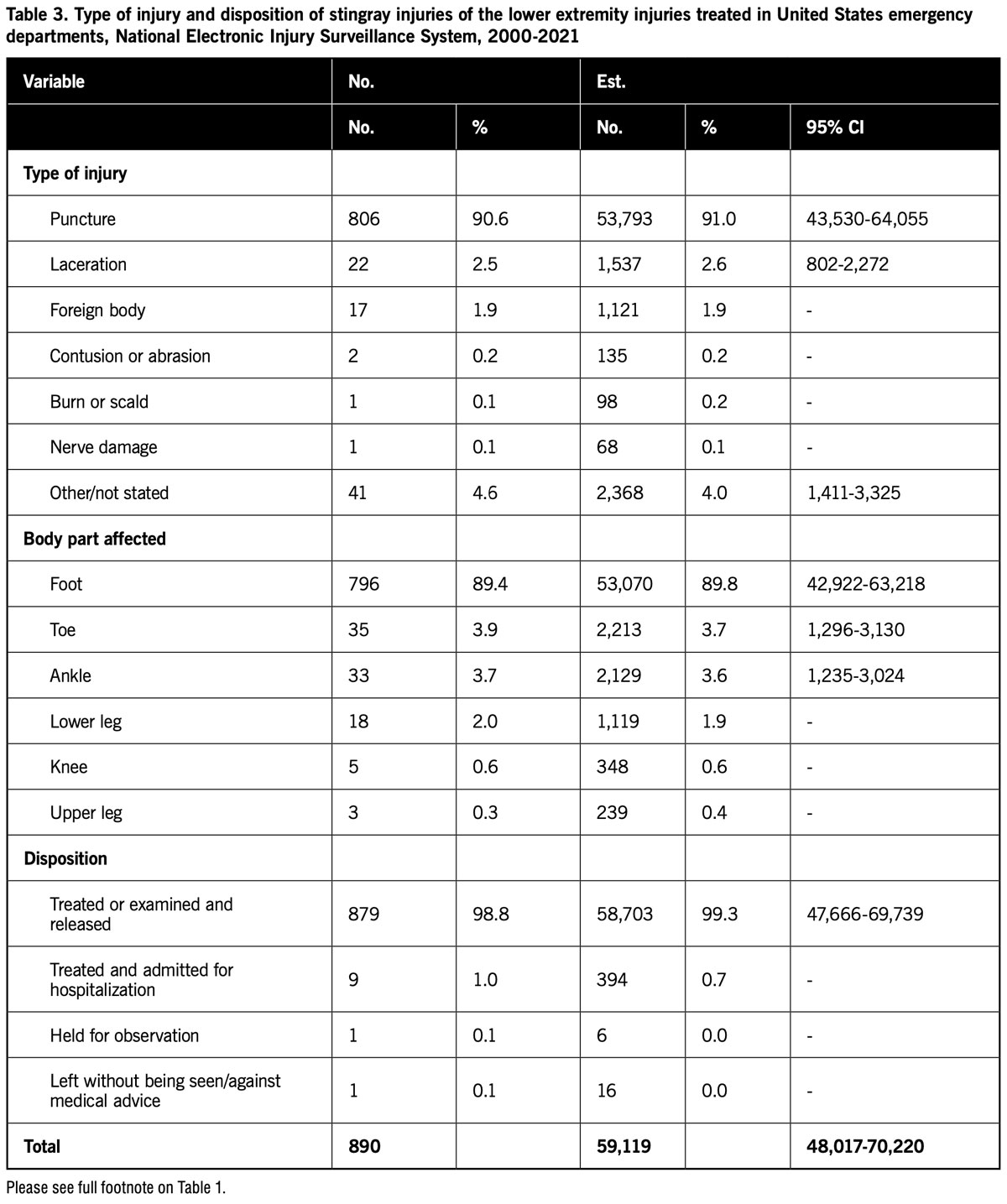
Table 3 shows the distribution of stingray injuries of the lower extremity by type of injury and patient disposition. The majority of injuries were a puncture, and most of the injuries involved the foot. The majority of patients were treated or examined in the hospital ED and released.
Discussion
This study examined stingray injuries of the lower extremity treated in US hospital EDs. Over one thousand stingray injuries are estimated to occur in the US annually.2,8 This study found that 88% of all estimated stingray injuries treated at hospital EDs involved the lower extremity. Thus, examination of the characteristics of stingray injuries focusing on the lower extremity may be particularly useful.

The estimated number of stingray injuries of the lower extremity declined during the 22-year period of the study. This may be due to a decline in the total number of stingray injuries that occur or a decreasing proportion of stingray injuries being treated at hospital EDs. Two studies that examined stingray injuries reported to state poison centers found that the majority of patients were managed outside of a healthcare facility.9,10 Moreover, people may be able to find information on how to treat a stingray injury on the internet. Thus, during the latter part of the study period, people may have increasingly sought treatment of stingray injuries outside of hospital EDs.
Changes in the NEISS itself also may account for the decline in the estimated number of stingray injuries. There may have been changes in the NEISS inclusion or exclusion criteria that resulted in fewer stingray injuries being included in the database. In addition, the specific hospitals that participate in NEISS change over time due to sample redesigns where another stratified random sample of hospitals is performed as well as changes in hospital size and the opening and closure of hospitals.13-15 All hospitals are not equally likely to treat stingray injuries. Since stingrays are predominantly found in the ocean, hospitals closer to the coast may be more likely to treat stingray injuries. Furthermore, stingray injuries may be more likely to occur in coastal areas with larger human populations or where people are more likely to fish or take part in other aquatic activities (e.g., popular fishing spots or public beaches). The study of stingray injuries report to Texas poison centers found that 60% of the injuries were reported from counties along the coast and 33% of the injuries were reported from only two counties.10 Therefore, changes in the hospitals participating in NEISS over time might affect the number of stingray injuries included in the database.
Stingray injuries of the lower extremity were seasonal, with the highest proportion treated in the summer (June-August) and the lowest proportion in the winter (December-February). The two poison center studies found over half of the stingray injuries were reported during June-August.9,10 People may be more likely to engage in ocean activities, and thus more likely to encounter stingrays, in the summer. Almost 45% of the stingray injuries of the lower extremity were treated on the weekend, a time when people are more likely to have free time to engage in ocean activities.
 The majority of patients were adults, and most patients were male. This is consistent with the poison center studies.9,10
The majority of patients were adults, and most patients were male. This is consistent with the poison center studies.9,10
The majority of stingray injuries of the lower extremity occurred while the patient was swimming with smaller proportions occurring when the patient was fishing or surfing. Moreover, 95% of all stingray injuries that occurred while the patient was swimming resulted in lower extremity injuries while only 37% of all stingray injuries that occurred while the patient was fishing resulted in lower extremity injuries. When swimming, a person might be more likely to be injured when they accidentally step on a stingray. In contrast, when fishing, a person might be more likely to receive injuries to other parts of the body, particularly, the upper extremity, as they try to handle a stingray.
The majority of the stingray injuries involved the foot. This might be expected considering that people are most likely to encounter a stingray by stepping on the fish. The most frequently reported diagnosis was a puncture, and approximately 99% of the patients were treated or examined and released from the ED. Punctures and other reported injuries such as lacerations and foreign bodies might be considered relatively minor and usually not require hospitalization.
This study is subject to various limitations. The NEISS collects data on consumer product-related injuries in the US, although the definition of “consumer product-related” does include all injuries where a consumer product, sport, or recreational activity is associated with the reason for the visit or related to a condition treated.14 Therefore, only those stingray injuries related to consumer products (including sport and recreational activities) would be included in the study, a subset of total stingray injuries. However, advantages of the NEISS database are that its data are publicly available and includes hospitals from all regions of the US. Another study limitation was that cases were identified by searching for the letter combinations “sting,” and “ray” in the Narrative field, and the selection of records to be included in the study was performed by a single person. Errors in the selection of records may have resulted in records being included or excluded erroneously. Furthermore, only those stingray injuries of the lower extremity treated at hospital EDs were included in the study. The number of such injuries not seen at EDs (i.e., managed at home or by a private physician) is unknown.
In conclusion, stingray injuries of the lower extremity most frequently occurred while the patient was swimming. The injuries were seasonal, most often occurring during the summer. The majority of patients were adults, and most were male. The foot was the part most often injured. The majority of patients were treated or examined and released from the hospital ED.
Mathias B. Forrester, BS, is an independent researcher in Austin, Texas. Now retired, he previously performed public health research for various university and government programs for 34 years.
- Slaughter RJ, Beasley DM, Lambie BS, Schep LJ. New Zealand’s venomous creatures. N Z Med J. 2009;122(1290):83-97.
- Scharf MJ. Cutaneous injuries and envenomations from fish, sharks and rays. Dermatol Ther. 2002;15(1):47-57.
- Fenner PJ. Dangers in the ocean: the traveler and marine envenomation. II. Marine vertebrates. J Travel Med. 1998;5(4):213-216.
- Meyer PK. Stingray injuries. Wilderness Environ Med. 1997;8(1):24-28.
- Auerbach PS. Marine envenomations. N Engl J Med. 1991;325(7):486-493.
- da Silva NJ, Ferreira KR, Pinto RN, Aird SD. A severe accident caused by an Ocellate River stingray (Potamotrygon motoro) in Central Brazil: How well do we really understand stingray venom chemistry, envenomation, and therapeutics? Toxins (Basel). 2015;7(6):2272-2288.
- Kizer KW. Marine envenomations. J Toxicol Clin Toxicol. 1983;21(4-5):527-555.
- Auerbach PS. Envenomations by aquatic vertebrates. In: Auerbach PS, ed. Wilderness Medicine. 5th ed. St. Louis, MO: Mosby; 2007:1730–1749.
- Clark AT, Clark RF, Cantrell FL. A retrospective review of the presentation and treatment of stingray stings reported to a poison control system. Am J Ther. 2017;24(2):e177-e180.
- Forrester MB. Pattern of stingray injuries reported to Texas poison centers from 1998 to 2004. Hum Exp Toxicol. 2005;24(12):639-642.
- Collins G. Steve Irwin, wildlife master, is killed by a stingray at 44. New York Times September 5, 2006. Available at https://www.nytimes.com/2006/09/05/obituaries/05irwin.html. Accessed January 10, 2023.
- Forrester MB. Dog leash-related injuries of the lower extremity treated at hospital emergency departments. Lower Extremity Review. 2022;14(6):41-42,45,47,49.
- United States Consumer Product Safety Commission. National Electronic Injury Surveillance System (NEISS). Available at https://www.cpsc.gov/Research–Statistics/NEISS-Injury-Data/Explanation-Of-NEISS-Estimates-Obtained-Through-The-CPSC-Website. Accessed January 10, 2023.
- United States Consumer Product Safety Commission. NEISS Coding Manual. January 2021. Available at https://www.cpsc.gov/s3fs-public/January-2021-NT-CPSC-only-NEISS-Coding-Manual.pdf?xa_nMM1kB4SGpuSMOwf0NHkkkIqNcn8F. Accessed January 10, 2023.
- Huang G [Internet]. Improving the capture of poisonings in children and youth by the Canadian Hospital Injury Reporting and Prevention Program. July 28, 2011. Available at https://dspace.library.uvic.ca/bitstream/handle/1828/3812/Huang_Grace_MPA_2j011.pdf?sequence=1&isAllowed=y. Accessed January 10, 2023.





