
 By Mathias B. Forrester, BS
By Mathias B. Forrester, BS
Abstract
Background: Using ziplines has gained popularity as a form of outdoor recreation. However, using or being in proximity to ziplines may result in injury. The objective of this study was to describe zipline-related lower extremity injuries treated at hospital emergency departments (EDs).
Methods: Data were from the National Electronic Injury Surveillance System (NEISS), a database of consumer product- and activity-related injuries collected from a representative sample of approximately 100 U.S. hospital EDs. National estimates are calculated from database records according to the sample weight assigned to each case based on the inverse probability of the hospital being selected for the NEISS sample. Cases were all records during 2000–2024 with zipline-related injuries treated during 2000–2024 where the most severe diagnosis involved the lower extremity. The distribution of estimated zipline-related lower extremity injuries was determined for selected variables.
Results: Of an estimated 7,962 zipline-related lower extremity injuries treated at U.S. hospital EDs, 0.7% were treated during 2000–2004, 3.8% during 2005–2009, 21.3% during 2010-2014, 31.5% during 2015–2019, and 42.7% during 2020–2024. The most severe diagnosis was 31% fracture, 22.1% contusion or abrasion, 21.8% strain or sprain, 7.1% laceration, and 18.1% all other or not stated. The location of the incident was 72.5% place of recreation or sports, 7.8% home, 3.6% school, 1.3% other public property/street or highway, and 14.8% not recorded. The mechanism of the injury was 32.9% fall, 31.1% collision or hit, 17.4% other mechanism, and 18.6% unknown mechanism.
Conclusion: Zipline-related lower extremity injuries increased during the last 25 years. Roughly equal proportions of lower extremity injuries were due to falls and collisions or hits. While most of the injuries occurred at a place of recreation or sports, injuries also occurred at home or school. The information in this study may be useful for the creation and implementation of strategies to reduce the risk of zipline-related lower extremity injuries.
A zipline is a horizontal rope, wire, or beam with a mechanical system that allows a person to slide along the rope, wire, or beam by hanging beneath it.1 Ziplines can range from something as simple as a piece of wire and a clothesline pulley to complex assemblies containing cables, attachments, trollies, computer control systems, hydraulics, motors, and sophisticated braking systems.2 Using ziplines has gained popularity as a form of outdoor recreation.3 As of 2020, there were over 400 commercial ziplines in the U.S. that provided more than 70 million rides annually.2,3
Using or being in proximity to ziplines may result in injury, the most common being fractures, soft tissue injuries, strains and sprains, lacerations, and concussions and closed head injuries.4,5 Deaths have been reported with zipline use.1,2,4
Published research on zipline-related injuries is limited. The objective of this study was to describe zipline-related lower extremity injuries treated at hospital emergency departments EDs. One previous study reported that 24% of all zipline-related injuries involved the lower extremity.5
 Methods
Methods
This study used data from the National Electronic Injury Surveillance System (NEISS database available at https://www.cpsc.gov/cgibin/NEISSQuery/home.aspx). The author has previously described the NEISS database in Lower Extremity Review.6 To summarize, NEISS collects data on consumer product- and activity-related injuries from a probabilistic sample of the EDs of approximately 100 U.S. hospitals. National estimates are calculated from database records according to the sample weight assigned to each case based on the inverse probability of the hospital being selected for the NEISS sample.7,8 The data are publicly available and de-identified, so the study is exempt from institutional review board approval. Several previously published studies used NEISS data to examine zipline-related injuries;4,5 however, neither study focused on lower extremity injuries.
Zipline-related injuries reported to NEISS were identified using criteria similar to that used in a prior study.5 The Narrative text fields (a text field that summarizes the circumstances of the injury) for all records during 2000–2024 were searched for the following letter groups: (1) “zip” and “line,” “lini,” “cord,” “swing,” or “wire” or (2) “fly” and “fox.” The Narrative fields of the resulting subset of records were then individually reviewed by the author to verify that the record involved a zipline-related injury. At the same time, the mechanism of the injury as stated in the Narrative was identified and assigned of the following categories: fall, collision or hit (including being hit by a part of the zipline), other, and unknown. If a person fell and then collided with something, the mechanism was categorized as a fall. If the person collided with something and then fell, the mechanism was categorized as a collision or hit.
The following variables were examined: affected body part, most severe diagnosis (type of injury), patient disposition, mechanism of injury, location of the incident, year and month of treatment, and patient age and gender. The NEISS database contains multiple fields for documenting the diagnosis and/or affected body part; however, only 2 fields were used consistently throughout the study period: Diagnosis (a numeric field for coding the most severe diagnosis) and Body_Part (a numeric field for coding the body part associated with the most severe diagnosis). (All diagnoses are supposed to be documented in the Narrative, but this is not performed in a consistent manner.) Therefore, only the Diagnosis and Body_Part numeric fields were used to analyze the diagnosis and affected body part. The study was limited to those zipline-related injuries where the Body_Part field included codes for parts of the lower extremity.
Analyses were performed using Microsoft 365 Access and Excel (Microsoft Corporation, Redmond, WA). For the selected variables, the distribution of the national injury estimates was determined. National injury estimates were calculated by summing up the values in the Weight numeric field in the NEISS database. The US Consumer Product Safety Commission (CPSC), which operates the NEISS, considers an estimate unstable and potentially unreliable when the estimate is <1,200.7
 Results
Results
An estimated 7,962 zipline-related injuries were treated at U.S. hospital EDs during 2000–2024 where the most severe diagnosis affected the lower extremity. This represented 17.1% of the estimated 46,572 such injuries affecting all body parts. There were 58 (0.7%) zipline-related lower extremity injuries treated during 2000–2004, 300 (3.8%) during 2005–2009, 1,696 (21.3%) during 2010–2014, 2,504 (31.5%) during 2015–2019, and 3,403 (42.7%) during 2020-2024. There were an estimated 749 (9.4%) injuries treated in December-February, 1,900 (23.9%) in March-May, 3,646 (45.8%) in June-August, and 1,667 (20.9%) in September-November.
The patient age distribution was 112 (1.4%) 0–5 years, 2,909 (36.5%) 6–12 years, 821 (10.3%) 13–19 years, 886 (11.1%) 20–29 years, 562 (7.1%) 30–39 years, 1,211 (15.2%) 40–49 years, 603 (7.6%) 50–59 years, 731 (9.2%) 60–69 years, and 126 (1.6%) 70 years and older. The patients were 4,783 (60.1%) female and 3,179 (39.9%) male.
The location of the incident was 5,768 (72.5%) place of recreation or sports, 623 (7.8%) home, 283 (3.6%) school, 106 (1.3%) other public property/street or highway, and 1,181 (14.8%) not recorded. The mechanism of the injury was 2,616 (32.9%) fall, 2,478 (31.1%) collision or hit, 1,386 (17.4%) other, and 1,481 (18.6%) unknown.
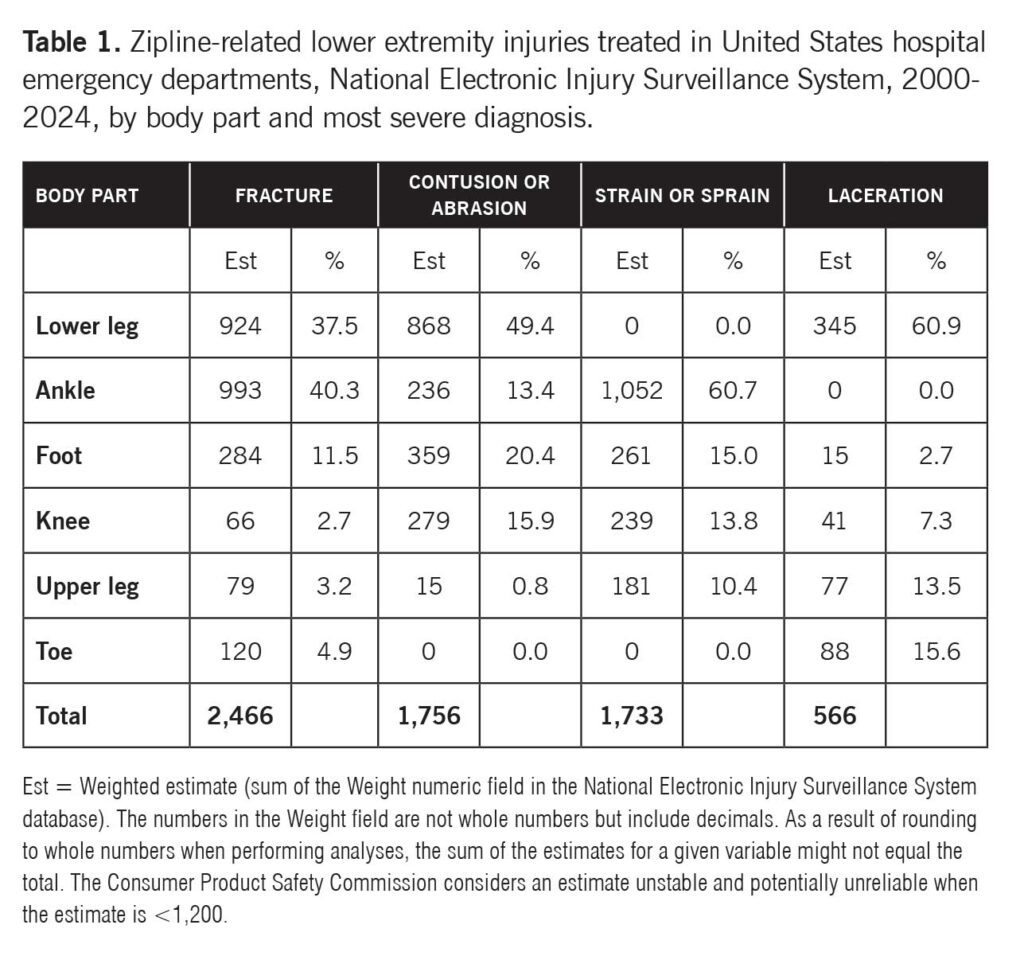
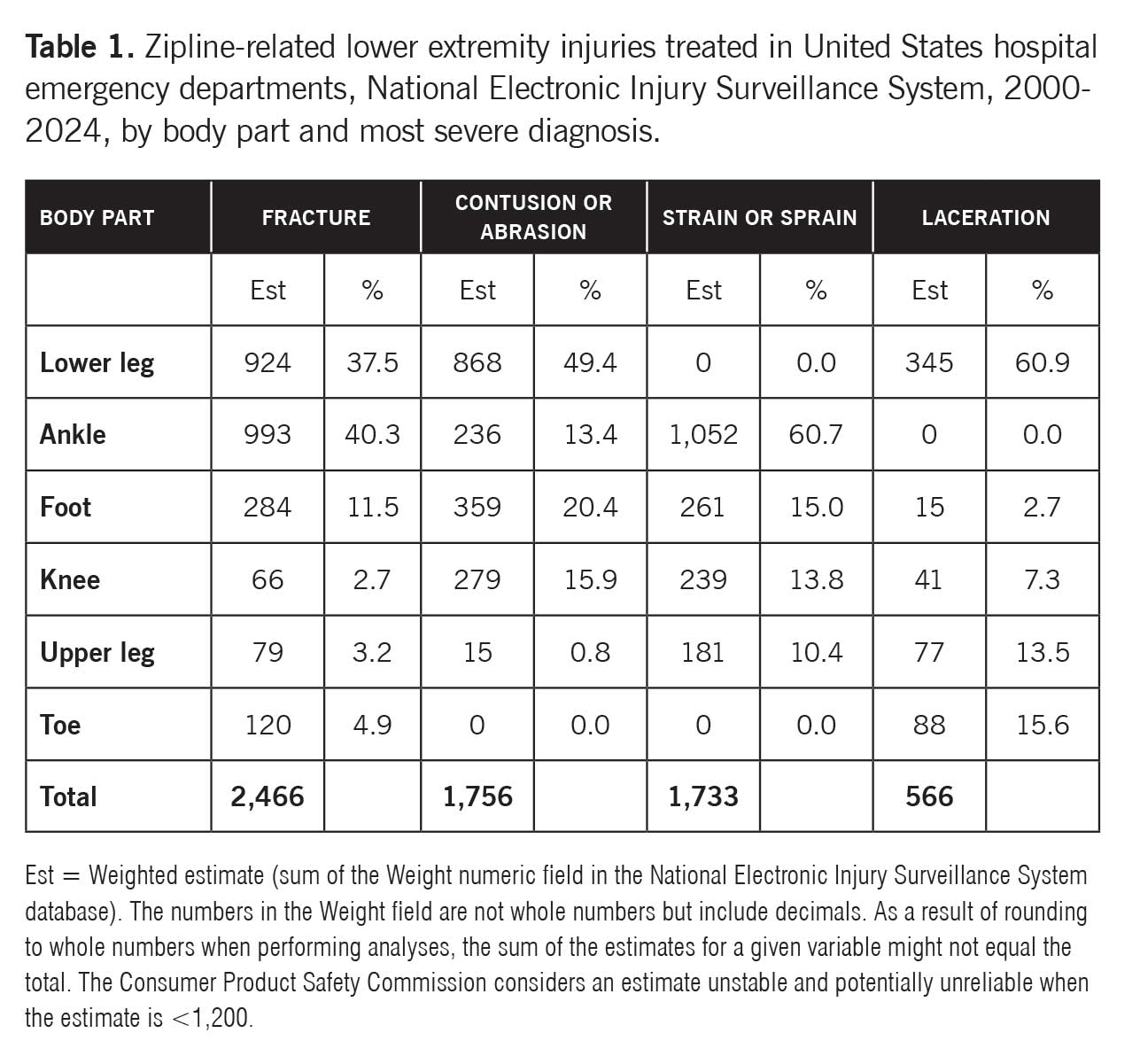
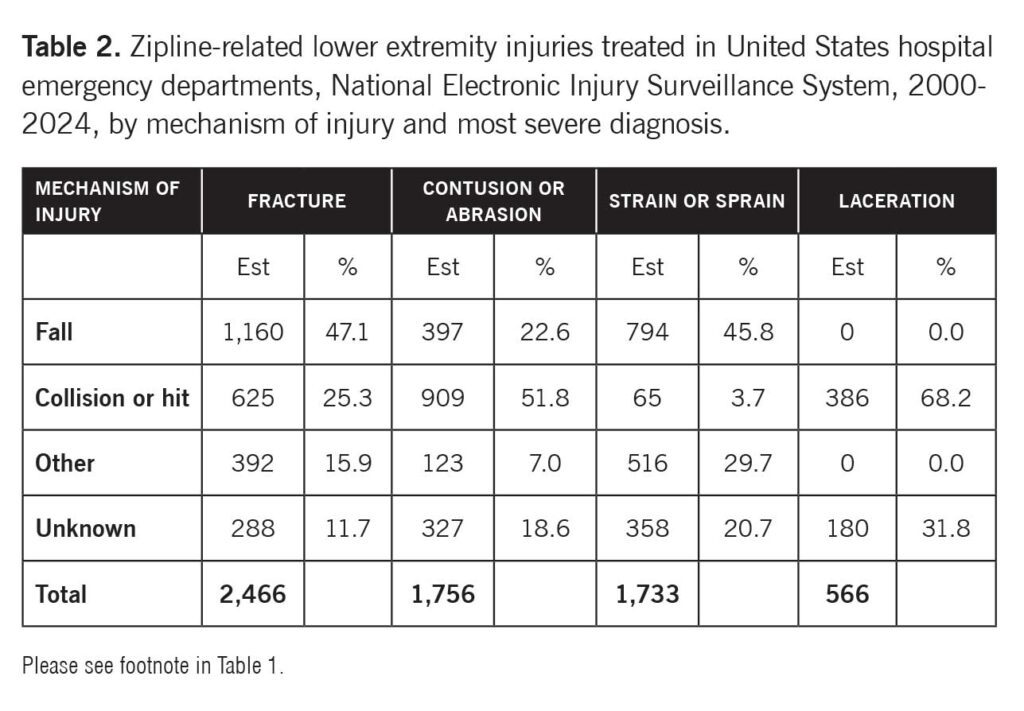
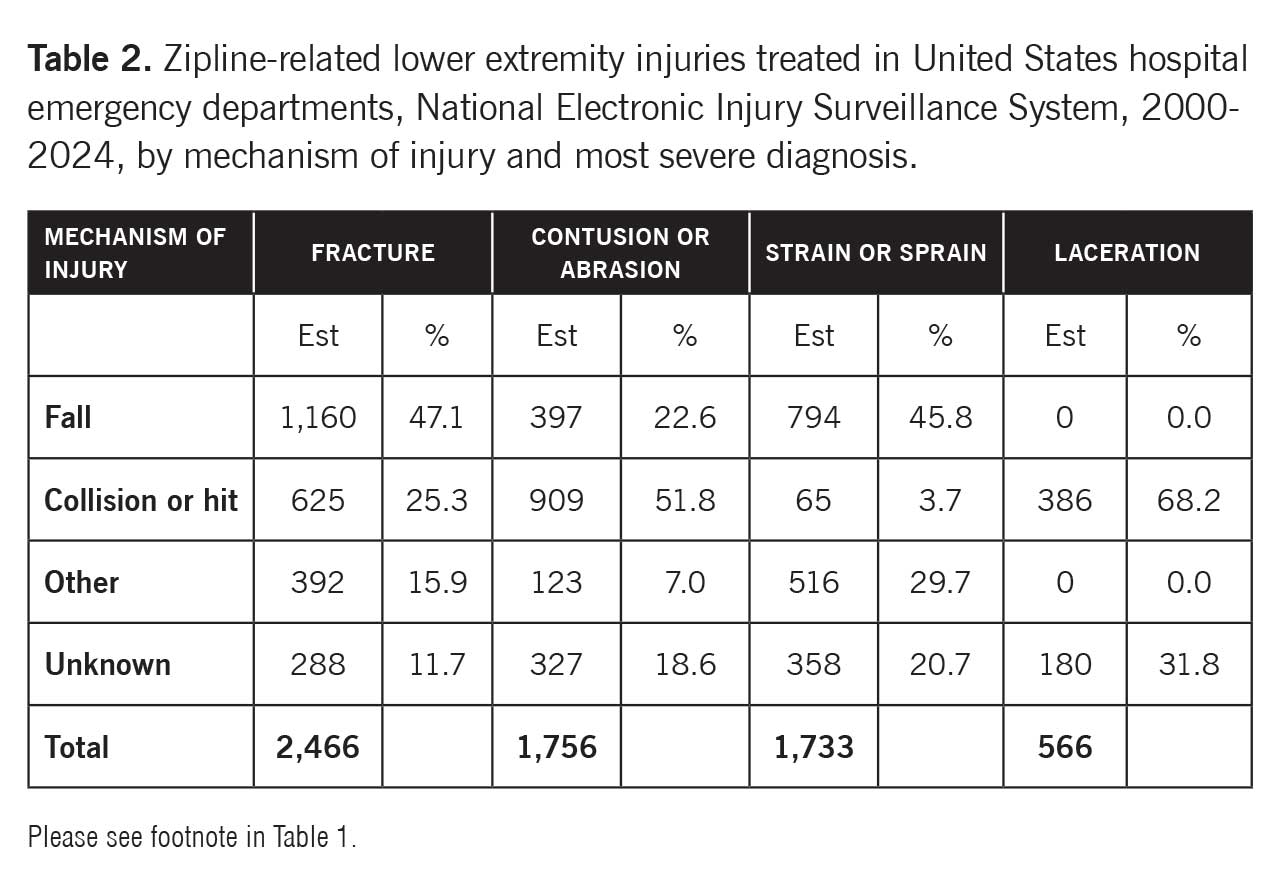
The affected body part was 2,651 (33.3%) lower leg, 2,538 (31.9%) ankle, 1,147 (14.4%) foot, 1,055 (13.2%) knee, 362 (4.6%) upper leg, and 208 (2.6%) toe. The most severe diagnosis was 2,466 (31.0%) fracture, 1,756 (22.1%) contusion or abrasion, 1,733 (21.8%) strain or sprain, 566 (7.1%) laceration, and 1,441 (18.1%) all other or not stated. Table 1 shows the distribution of estimated zipline-related lower extremity injuries by body part and most severe diagnosis. While the highest proportion of fractures involved the ankle followed by the lower leg, the highest proportion of contusions or abrasions involved the lower leg followed by the foot. Most strains or sprains involved the ankle followed by the foot, and the majority of lacerations involved the lower leg followed by the toe. Table 2 provides the distribution of estimated zipline-related lower extremity injuries by mechanism of injury and most severe diagnosis. While the highest proportion of fractures and strains or sprains resulted from falls, most contusions or abrasions and lacerations resulted from collisions or hits.
The patient disposition was 7,261 (91.2%) treated or examined in the ED and released, 543 (6.8%) treated and admitted for hospitalization (within same facility), 147 (1.8%) treated and transferred to another hospital, 6 (0.1%) held for observation (includes admitted for observation), and 5 (0.1%) left without being seen or left against medical advice.
Discussion
This study found that the estimated number of zipline-related lower extremity injuries treated at U.S. hospital emergency departments increased over the 25-year study period. This might be expected since ziplining has increased in popularity in the U.S.3 It is also consistent with several prior studies of all zipline-related injuries using NEISS data that likewise observed an annual increase in injuries.4,5 Continued monitoring of zipline-related lower extremity injuries may be useful to determine whether this trend continues.
The lower extremity injuries were seasonal, with 46% of the estimated injuries treated in June-August and only 9% in December-February. A previous study also noted a seasonal trend, with 91% treated in April-October, peaking in July.5 Although some ziplines can be found indoors, it is likely that most are used outdoors—and thus more likely to be used during the warmer months. Similarly, children are more likely to use ziplines during the summer, when they are out of school and have more free time.
While the highest proportion (37%) of patients were aged 6–12 years, the next highest proportion (15%) involved patients in the 40–49-year age group. Younger school-aged children might be the age group most likely to use ziplines, or, at least, use them in such a way that they may become injured. That people in their 40s accounted for the next highest proportion of injuries is more difficult to explain. People in this age group may be more likely than other adults to use ziplines or be injured while using the devices.
Most of the patients with zipline-related lower extremity injuries were female, a pattern found in the prior study that examined all zipline-related injuries among people of all ages.5 It may be that females are more likely to use ziplines or use them in a manner that leads to injury.
Although 72% of the lower extremity injuries occurred at a place of recreation or sports, 8% occurred at home and another 4% at school. This suggests that strategies to reduce the risk of zipline-related injuries should not only focus on commercial facilities that offer ziplining or public places, such as public parks, where ziplines may be found but should also include schools and people who may be likely to have ziplines on their own property.
Although falls accounted for the highest proportion (33%) of lower extremity injuries, collisions or hits accounted for almost as many (31%). In one of the previous studies of zipline-related injuries involved people of all ages, 77% of the injuries were due to falls and 13% to collisions,5 and in the prior study that involved only children aged 0-17 years, 86% were due to falls and 14% due to impact with another surface.4. Of the 46,572 zipline-related injuries treated during 2000-2024 affecting all body parts, 28,477 (61.1%) involved falls, 9,131 (19.6%) collisions or hits, 4,006 (8.6%) other mechanisms, and 4,958 (10.6%) an unknown mechanism. This suggests that lower extremities are less likely than other body parts to be injured in falls and more likely to be injured in collisions or hits. This may need to be taken into consideration when trying to implement strategies to prevent zipline-related lower extremity injuries. A strategy that reduces the risk of falls but not collisions or hits, or vice versa, may have differential impact on injuries to different body parts.
The most injured body parts were the lower leg and ankle, together accounting for almost two-thirds of the estimated injuries. The most common serious diagnosis was fracture, followed by contusion or abrasion, strain or sprain, and laceration–patterns observed in the previous studies of zipline-related injuries using NEISS data.4,5 The present study found that the diagnoses differed by both affected body part and mechanism of injury. As mentioned previously, the risk of injury to a particular body part may differ by the injury mechanism. Similarly, the risk of a particular type of injury (diagnosis) may differ by both the injury mechanism and body part.
The most common types of injury observed in this study–fractures, contusions or abrasions, strains or sprains, and lacerations–might not be expected to usually require extensive medical intervention. This is consistent with the observation that most of the patients were treated or examined at the ED and released. The prior zipline-related injury studies using NEISS data observed a similar pattern of patient disposition.4,5
This study has limitations. To identify cases, all records where the Narrative fields contained particular letter groups were first selected and then the Narrative field for each record was reviewed to determine whether the injury was zipline-related. The study would not include any records with zipline-related injuries that did not include the letter groups of interest or clearly indicated that the injury was zipline-related.
In addition, a person injured by a zipline may experience multiple injuries of the same or multiple body parts. This study was limited to the data fields that coded the single most severe diagnosis and affected body part because these were the only fields that consistently documented diagnosis and affected body part throughout the entire study period. Thus, a higher proportion of patients may have experienced lower extremity injuries.
Furthermore, only the author selected the records for inclusion in the study and assigned the mechanism of injury. Moreover, the study only included those patients treated at hospital EDs. Examination of patients treated elsewhere would provide a more complete understanding of zipline-related lower extremity injuries.
In conclusion, zipline-related lower extremity injuries increased during the last 25 years. The highest proportion of injuries involved children aged 6-12 years, and most of the patients were female. Roughly equal proportions of lower extremity injuries were due to falls and collisions or hits. While most of the injuries occurred at a place of recreation or sports, injuries also occurred at home and school. The information in this study may be useful for the creation and implementation of strategies to reduce the risk of zipline-related lower extremity injuries.
Mathias B. Forrester, BS, is an independent researcher in Austin, Texas. Now retired, he has performed public health research for various universities, government programs, and other organizations for 40 years.
- Hanway S. Injuries and investigated deaths associated with playground equipment, 2009–2014. US Consumer Product Safety Commission, August 2016. https://www.cpsc.gov/s3fs-public/Injuries%20and%20Investigated%20Deaths%20Associated%20with%20Playground%20Equipment%202009%20to%202014_1.pdf . Accessed December 9, 2025.
- Adamson I. Zip line injuries, risks, and safety. Robson Forensic, March 24, 2020. https://www.robsonforensic.com/articles/zip-line-safety-expert. Accessed December 9, 2025.
- Vianna C. Zipline industry statistics. Xola, July 4, 2023. https://www.xola.com/articles/zipline-industry-statistics/. Accessed December 9, 2025.
- Leeper CM, McKenna C, Gaines BA. Homemade zipline and playground track ride injuries in children. J Pediatr Surg. 2017;52(9):1511-1515.
- Billock RM, Anderegg JJ, Mehan TJ, Chounthirath T, Smith GA. Zipline-related injuries treated in US EDs, 1997-2012. Am J Emerg Med. 2015;33(12):1745-1749.
- Forrester MB. Pickleball-related injuries involving the lower extremity treated in emergency departments. Lower Extremity Review. 2021;13(5):24-30.
- United States Consumer Product Safety Commission. National Electronic Injury Surveillance System (NEISS). https://www.cpsc.gov/Research–Statistics/NEISS-Injury-Data/Explanation-Of-NEISS-Estimates-Obtained-Through-The-CPSC-Website. Accessed December 9, 2025.
- United States Consumer Product Safety Commission. NEISS Coding Manual. January 2025. https://www.cpsc.gov/s3fs-public/JANUARY-2025-NEISS-CPSC-only-Coding-Manual-Rev-1.pdf. Accessed December 9, 2025.





