By Larisa Ryskalin, PhD; Gabriele Morucci, PhD; Paola Soldani, PhD; and Marco Gesi, PhD
Plantar fasciitis is a chronic and painful disabling condition affecting the inferomedial aspect of the heel, usually extending toward the metatarsophalangeal joints. These authors examined the anatomical and biomechanical substrates of plantar fasciitis with special emphasis on the emerging, though largely neglected, fascial system.
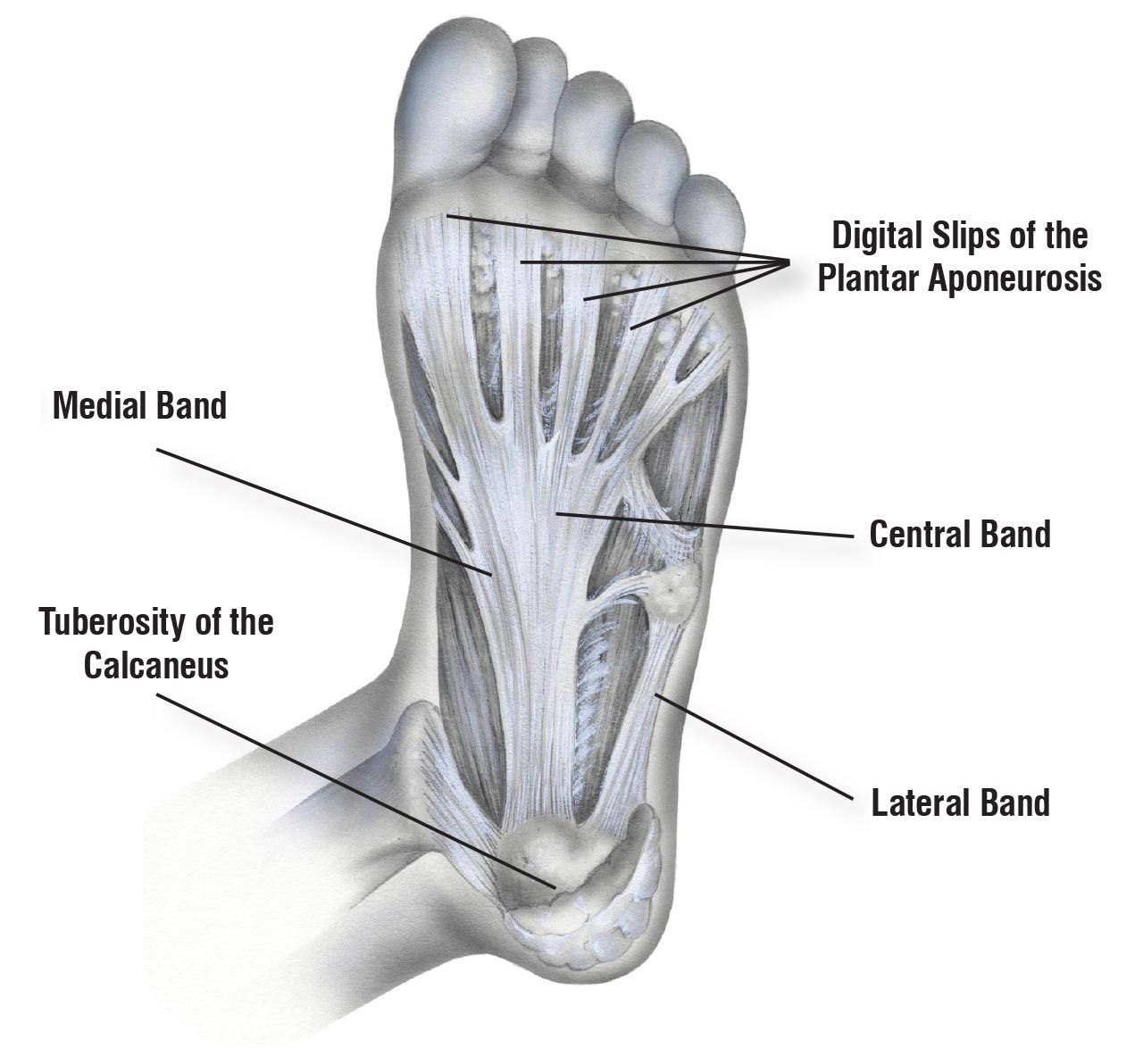
Figure 1. Schematic representation of the anatomy of the plantar aponeurosis.
The Critical Coordination between the Triceps Surae Muscle, Achilles Tendon (AT), and Plantar Aponeurosis (PA): the Emerging Role of the Fascia
The potential role of the suro-Achilleocalcaneal-plantar complex in PA pathology
The triceps surae complex represents the main extensor and propulsion system of the foot, and is equipped with a very sophisticated driving belt, namely the AT-posterior part of the calcaneus-PA in continuity with the fibrous skeleton of the triceps surae. This suro-Achilleo-calcaneal-plantar system was first described by Arandes and Viladot in 1954. They showed how the triceps surae complex is placed in series with the PA to ensure force transmission from the triceps surae toward the toes during walking, running, and jumping. Also referred to as the Achilleo-calcaneal-plantar complex (ACP), it was intensively investigated by French and Spanish research groups during the 1990s from both anatomical and biomechanical viewpoints.
The triceps surae muscle contributes differentially to lower limb movements. In detail, the medial and lateral heads of the gastrocnemius cross both the knee and ankle joints, proximally forming the lower boundary of the popliteal fossa. These muscles then connect to each other in the midline of the superficial posterior compartment of the leg, accounting for the characteristic bulge of the calf. In contrast, the soleus is a one-joint muscle. Its fibers originate below the knee, extending more distally along the tibia than those of the gastrocnemius. Thus, the soleus only crosses the ankle joint, having no action on the knee joint. As a result, the gastrocnemius is mostly involved in forward propulsion during walking, running, and jumping, whereas the soleus primarily acts as a foot stabilizer, giving the body vertical support while standing. This is reflected in their muscle fiber type compositions: the gastrocnemius predominantly consists of Type II (or fast twitch) fibers while the soleus contains a high percentage of Type I (or slow twitch) fibers. Consequently, skeletal muscle mass is lost more rapidly in the soleus than in the gastrocnemius, making the soleus a more sensitive indicator of skeletal muscle atrophy in response to muscle “disuse.” This is well documented both in rodents and humans, with considerable similarities.
The soleus is generally considered at lower risk for strains than the gastrocnemius. However, soleus muscle injury could have been underestimated, owing to misdiagnosis as thrombophlebitis or gastrocnemius strain. Furthermore, soleus muscle strains could be underappreciated owing to the traditional use of sonography (ultrasound) for assessing calf muscle injuries. Gastrocnemius strains are easier to detect because the muscle has a superficial anatomical location, while the soleus is located much deeper in the calf region. This could explain why sonography reveals fewer soleus injuries than gastrocnemius injuries.
However, structural alterations in muscle strain injuries or abnormal patterns of skeletal muscle activity are not necessarily restricted to the muscle, but can affect the fascia. Very recently, Otsuka et al. reported changes in the elastic properties and mechanical behavior of the fascia lata associated with underlying quadriceps femoris muscle contractions, measured in vivo by shear wave elastography. The surrounding fasciae of adjacent muscles are intimately connected, creating continuity rather than separation. This challenges the classic concept of muscles as independent actuators of movement, the fasciae being merely passive packing of the underlying skeletal muscles. Contrary to this common assumption, increasing evidence demonstrates that the fascia performs several important functions in the body beyond architectural/structural ones. It is an active player in biomechanical force transmission and tensile load bearing. At the same time, it can change its biomechanical properties in response to musculoskeletal dynamics. This intimate relationship between skeletal muscles and fascia supports the concept of “myofascial continuity,” which emphasizes that an endless and extensive tensegrity network runs throughout the human body. This has enormous potential implications for both training and therapy. An example of this emerging concept is the superficial back line, a myofascial chain/meridian consisting of the PA, the AT, and the gastrocnemius, which then runs toward the hamstrings, the lumbar fascia, the erector spine, and up to the epicranial fascia. These latter findings could provide a plausible explanation for the onset of plantar fasciitis symptoms as a consequence of muscle overuse, where tension is transferred from a stiff gastrocnemius to the sole through the AT-calcaneal-plantar complex. As a proof of concept, gastrocnemius tightness has long been considered a risk factor for plantar fasciitis. For instance, in 2011 Patel and DiGiovanni found that 83% of a sample of 254 subjects with plantar fasciitis had an isolated contracture of the gastrocnemius and/or gastrocnemius-soleus tightness. At the same time, there is evidence that these muscles do not move totally independently of each other. Percutaneous electrical stimulation of the gastrocnemius can induce simultaneous displacement of the soleus, which suggests force transmission between these muscles. Other recent in vivo studies provide evidence for inter- and intramuscular interactions within human calf muscles. Therefore, it seems plausible that even soleus muscle dysfunctions can impair force transmission between the calf muscles and the myofascial system, becoming an etiological factor in plantar fasciitis.
Structural and Functional Coupling between Muscles and Fascia
The potential role of the fascial tissue in PA pathology
Over the years, inexact, ambiguous, or confounding definitions have portrayed the human fascial system as something “mostly left to the imagination of the students”. The differences in characteristics of the fascia depending on the anatomical region (neck, trunk, or limbs) provide an additional challenge to the definition of this organ. Although the fascia remains largely neglected, new methodological findings and assessment methods, along with changes in anatomical dissection, have greatly clarified the anatomical and biomechanical recognition and definition of this fundamental system of the human body.
In recent years, the fascia has received increasing attention as a major contributor to movement perception, coordination, and the pathogenesis of musculoskeletal pain and dysfunction. Contrary to earlier assumptions, it is potentially a force transmitter intimately connected to the underlying skeletal muscle. A 2019 study by Schleip et al. demonstrated that the fascia has inherent contractility, thereby actively influencing musculoskeletal and biomechanical behavior. A potential role of fascia stiffness in limiting the maximal range of motion (ROM) of a joint has been also hypothesized. However, further efforts are needed to optimize the proposed novel methods for estimating the motion pattern of the fascia in vivo and its adaptability during muscle contraction.
At the microscopic level, fascial tissue comprises 2 or 3 layers of collagen fiber bundles, the fibers being differently oriented in each layer. This contributes to the strong resistance to traction of the fascia itself. Remarkably, the fascial system is viscoelastic because it contains high levels of hyaluronic acid (HA) in the interfaces between the collagen layers and between the deep fascia and the underlying muscle epimysium. This allows gliding to occur between the structures during movement and force transmission. The high concentration of HA also enables the facial tissue to undergo greater viscoelastic deformation than muscles and tendons. HA is a linear glycosaminoglycan consisting of regular repeating disaccharide units of N-acetyl-glucosamine and D-glucuronic acid, linked by β1-3 and β1-4 glycosidic bonds, respectively. Proper functioning of a healthy fascia requires specific levels of this essential component of the extracellular matrix. These can differ depending on the anatomical site, so the sliding properties of specific fascia also differ. For instance, Fede et al. reported a significant difference between the amount of HA in the aponeurotic fasciae (fascia lata of the thigh and rectus sheath of the abdomen, about 43 μg/g) and that in the epimysial fascia (or epimysium) of the trapezius and deltoid (about 6 μg/g). This is not surprising since these structures have totally different functions and mechanical properties. The aponeurotic fascia envelops various muscles and has a high potential for gliding, whereas the epimysium adheres more tightly to the underlying muscles. Alterations in the physiological levels or physicochemical properties of HA have been associated with several myofascial diseases.
It is well established that the main phenotypic and biochemical adaptations induced by exercise training involve the skeletal muscles. However, evidence that has emerged in recent decades suggests that the fascial tissue can also undergo molecular adaptations and/or alterations in response to muscle exercise. In particular, muscle overuse, disuse, or misuse can increase HA fascial densification, which results in greater resistance to fascial layer sliding and increased fascial stiffness. Muscle contraction-driven changes in loose fascial connective tissue can include increased HA production, aggregation of HA into supramolecular structures, changes in HA viscoelasticity and viscosity, and reduced HA lubrication. The HA content of the fascia lata was significantly reduced in patients with hip osteoarthritis (OA), where altered joint mechanics, distorted hip posture, and altered gait consequent on the disease resulted in altered fascial structure and behavior, further worsening the OA symptoms. Besides overuse syndromes, connective tissue can become tighter after direct traumatic injuries not involving muscle lesions. For instance, residual alterations in fascial sensitivity and movability (fascial densifications) were more prevalent in the lower limbs of individuals with a history of ankle sprain than in healthy controls.
Therefore, in recent years, different fascia-directed treatment modalities such as fascial manipulation, increased local temperature, and alkalinization have been proposed to reverse these alterations in HA and thus relieve the pain associated with fascial densification. Any impairment of proper fascial gliding results in anomalous tension and altered input transmission from the mechanoreceptors and nociceptors embedded within the fascial layers, which can influence musculoskeletal dynamics negatively and create conditions for the onset of myofascial pain. Indeed, if we inject hypertonic saline into the erector spine muscle, the thoracolumbar fascia, and the overlying subcutis, the patient will complain of more intense and unpleasant pain sensations if the fascia rather than muscular or subcutaneous tissue is injected. This means that the fascia can be considered a fully-fledged major pain generator in the musculoskeletal system. As a proof of concept, compelling evidence demonstrates that the fascia is more strongly innervated with multiple myelinated and nonmyelinated sensory nerve fibers, including nociceptive ones, than the adjacent muscle tissue.
Consistent with this hypothesis, repetitive microtraumas to the gluteus maximus muscle from overuse and misuse led to myofascial pain syndrome. Likewise, a recent report showed that the onset of acute Achilles paratendinopathy could be related to histological and biomechanical changes in the crural fascia resulting from calf muscles injury. Another recent study described a case series of 9 athletes with pain in the Achilles region who had tears in the fascia cruris from the attachment to the paratenon and AT. The deep crural fascia also has been implicated in overuse injuries such as medial tibial stress syndrome (MTSS), also known as “shin splints”. Bouché and Johnson hypothesized that the tenting effect of the tendons of the deep leg flexors, caused by eccentric muscle contraction, exerts a tensile strain load on the deep fascia directed toward its tibial crest insertion. It is therefore not surprising that manual treatment of the crural fascia is emerging as an effective option for relieving pain and restoring exercise tolerance in MTSS patients. Concerning the calf muscles, fascial lesions are more prevalent following muscle strain injuries within the soleus than the gastrocnemius or the hamstrings. Besides muscle contraction-driven changes in the mechanical properties of the fascia, mechanical adaptations at the fascial level after chronic stretching interventions have also been hypothesized. However, how and to what extent fascial tissue properties are affected by muscle overuse, misuse, or trauma still merits further investigation.
Future Directions and Perspectives
From the present narrative review, it transpires that clinicians and therapists who are going to treat plantar fasciitis should be more aware of the complex anatomical and biomechanical substrates that can underly the onset and development of PA pathology. In particular, their attention should not be restricted to the plantar aspect of the foot, but rather focused upstream on the myofascial chain consisting of the PA, the AT, and the triceps surae muscle and their fasciae. Evidence reported in the present paper has highlighted that biomechanical abnormalities within the myofascial unit can be crucial since they can place excessive stress on the PA and ultimately contribute to heel pain and plantar fascitiis. At the same time, the fascial tissue should not be neglected since it is potentially a prime contributor to the pathophysiology of several chronic musculoskeletal painful conditions. Clearly, the structure, function, and biomechanics of the fascial system still deserve more attention. Notwithstanding the decisive involvement of the fascia in the onset of overuse muscle injuries and painful syndromes, fascial injuries and alterations continue to be generally overlooked and are seldom considered. Future research efforts should be focused on the optimization of novel approaches to studying fascial mobility in vivo in both physiological and pathological conditions. This will allow clinicians to optimize treatment strategies and rehabilitation protocols to obtain better outcomes for patients affected by lower-limb musculoskeletal conditions such as plantar fasciitis.
Finally, because of the intimate anatomical and biomechanical relationship between the PA and the triceps surae complex, calf-stretching exercises are commonly used in therapeutic and rehabilitation protocols for plantar fasciitis. However, despite their widespread clinical application, their effectiveness in managing this condition has sometimes been questioned and conflicting data are reported in the current literature. This indicates the need for more carefully designed studies within this field. Other conservative treatments should be considered. This is the case, for instance, with eccentric calf-muscle exercises, which are increasingly being used to reduce pain and improve function in patients with Achilles tendinopathy. Thus, future research efforts should focus on evaluating the effectiveness of eccentric loading exercises for calf muscles and also for plantar fasciitis. Additional knowledge of the mechanisms that could underpin their clinical benefit would affect both the management and treatment of plantar fasciitis.
The authors serve s teaching or research faculty in the Department of Translational Research and New Technologies in Medicine and Surgery, and the Center for Rehabilitative Medicine “Sport and Anatomy” at the University of Pisa in Italy.
This article has been excerpted from “Do the fasciae of the soleus have a role in plantar fasciitis?” from Clin Anat. 2023 Aug 4. doi: 10.1002/ca.24102, by the same authors. Editing has occurred, including the renumbering or removal of tables, and references have been removed for brevity. Use is per CC Attribution 4.0 International License. Part I, which focused on the current understanding of plantar fasciitis, a brief on the anatomy of the Achilles tendon and its pathophysiology, and the anatomical and structural continuity between the plantar aponeurosis and Achilles paratenon, appeared in our Oct/Nov 2023 issue.





