
 By Jonathon Spanyer, Lauren A. Barber, Harrison Lands, Alexander Brown, Mary Bouxsein, Marilyn Heng, and Madhusudhan Yakkanti
By Jonathon Spanyer, Lauren A. Barber, Harrison Lands, Alexander Brown, Mary Bouxsein, Marilyn Heng, and Madhusudhan Yakkanti
Bisphosphonates are currently one of the most commonly prescribed medications to prevent osteoporotic fractures. Bisphosphonates are frequently used as first-line agents for postmenopausal osteoporosis. Alendronate was first synthesized in the 1970s, and by 2006 about 30 million prescriptions were written annually in the Unites States, accounting for nearly 15% of postmenopausal women. Because the incidence of osteoporotic fractures is expected to increase with the aging population, the prescriptions of bisphosphonates had also been predicted to increase. Yet with the advent of newer medications to treat osteoporosis, and with concerns about rare side effects from bisphosphonates such as osteonecrosis of the jaw and atypical femoral fractures (AFFs), a relative decrease in projected bisphosphonate utilization in the past decade has been realized.
Not limited to management of osteoporosis, bisphosphonates have been used to treat a variety of pathologies ranging from Paget’s disease of bone to hypercalcemia of malignancy. Safety profiles for bisphosphonates show they are generally well-tolerated, but more recently there have been concerns about the long-term use of bisphosphonates. In 2005, Odvina et al first reported on a small number of patients who experienced primarily non-spinal fractures of the lower extremity and femur while on bisphosphonate therapy, with histological analysis showing markedly suppressed bone formation after prolonged bisphosphonate use. Subsequently, several authors have reported similar findings, all associated with chronic bisphosphonate use. In each case, the fractures were found to be secondary to low-energy mechanisms, presented with prodromal thigh pain, and demonstrating a prominent femoral cortex medial spike radiographically (Figure 1). Bilateral AFFs have been reported in up to 48% of cases. Cortical thickening near the fracture site and delayed union after surgical repair have also been reported.
A taskforce committee report commissioned by the American Society for Bone and Mineral Research (ASBMR) has established definitions of the emerging phenomenon to standardize investigations into the pathophysiology, epidemiology, and orthopedic clinical and medical management of AFFs. Numerous authors have reported on patients who have sustained AFFs, including presentations, treatments, duration and type of bisphosphonate use, and final clinical outcomes. Although the radiographic characteristics and potential risk factors for AFFs have been well-described, less has been reported about the health-related quality of life (HRQOL) outcomes after patients have undergone surgical treatment for their AFF.
The objective of this study was to collect HRQOL outcomes from patients who underwent surgical treatment for their AFFs and compare them to a similar cohort who underwent surgical treatment for diaphyseal femoral fractures. In this way, we aimed to determine the relative effect of repaired AFFs compared with an otherwise healthy cohort sustaining a similar isolated fracture on quality-of-life (QOL) measures.

Figure 1. Representative atypical femur fracture radiograph. A 65-year-old female patient was taking bisphosphonates for 6 years, with 6 months of progressive prodromal thigh pain. She had seen an orthopedic surgeon 1 month prior to the fracture with pelvic X-rays showing no evidence of significant osteoarthritis at the time. Note the periosteal thickening of the lateral cortices (black and white arrows), noncomminuted transverse fracture, and the medial cortical spike (big arrow) that are typically seen in atypical femur fractures.
Methods & Results
Two large trauma center databases were retrospectively queried for surgically treated femur fractures. Fractures were grouped into AFFs and compared to a control cohort. Controls for the AFF group included women with diaphyseal fractures without additional AFF characteristics. Patients were contacted for administration of the Short Form36, version 2 (SF-36v2) Health Survey. Surveys were completed an average of 30.3 months (range, 6–138 months) and 25.5 months (range, 5–77 months) postoperatively for the AFF and non-AFF groups, respectively. All patients were female, with 46 patients in the AFF and 26 patients in the non-AFF group. The average age of the AFF group was 70.1 years compared with an average age of 67.4 years in the non-AFF group (P = 0.287). Over 90% (91.3%) of patients in the AFF group had a history of bisphosphonate use while 26.9% of patients in the non-AFF group had used bisphosphonates (P < 0.0001).
Table 1 details the group comparisons. Patients with AFF reported their postoperative physical and mental health to be no different than similarly aged patients with femoral diaphyseal fractures, as measured by the SF-36v2 Health Survey. These data suggest that mid-term patient-reported QOL outcomes are similar among women who sustain an AFF compared to a cohort of more typical femoral diaphyseal fractures.
Discussion
In this study, we aimed to assess self-reported HRQOL outcomes in women who sustained atypical femur fractures compared to those with isolated femoral diaphyseal fractures, both of whom underwent surgical repair of their fractures. The SF-36v2 questionnaire used to assess an individual’s health status can be used to compare outcomes between groups of patients by type of intervention or disease. The questionnaire consists of 8 scales yielding 2 summary measures: Physical Component Score (PCS) and Mental Component Score (MCS). With an average follow-up time of 2.4 years, both groups reported similar postoperative PCS and MCS.
Our finding of similar self-reported HRQOL between AFF and non-AFF patients was unexpected, given that the AFF group generally experienced lower-energy trauma (ground level fall, break while walking), compared to the non-AFF group. Other authors have shown that high-energy trauma can adversely affect HRQOL outcomes in orthopedic patients. However, Ko and Chang also reported on long-bone fractures with similar outcomes for overall SF-36v2 scores between higher-energy femoral shaft fractures and lower-energy isolated tibial shaft fractures after intramedullary nailing and subsequent implant removal and healing. Yet when divided into the survey’s domains, the PCS had a higher score for femoral shaft fracture patients (P = 0.002). Our study suggests that although generally lower-energy mechanisms were involved in the AFF group, the health effect upon the patient was still similar to the higher energy traumas in the non-AFF group. The clinical significance of our study is that patients with AFF may expect similar mid-term patient-reported physical and mental outcomes to their higher-energy non-AFF counterparts.
Although our study suggests similar mid-term outcomes between the cohorts after healing, other authors have reported higher rates of early postoperative complications among AFF patients with bisphosphonate use. A study by Edwards et al in 2013 reviewed data from the United States Food and Drug Administration Adverse Event Reporting System (FAERS), which revealed that 26% of cases of AFFs exhibited delayed healing or non-healing. Additionally, Bogdan et al in 2015 reported a 12% failure rate as well as delayed average time to union after surgical repair of AFFs.
Although we realize that bisphosphonates remain a choice of therapy for individuals at high risk for fracture, the potential concern of AFFs has come to the attention of practitioners and patients, and prescriptions for bisphosphonates have declined in the past decade. However, the fracture prevention benefits of bisphosphonates remain, and it should be noted that the overall risk–benefit profile of bisphosphonates should be carefully considered in at-risk patient populations. The current study indicates that mid-term health-related outcomes following surgical repair of AFF are similar to those of surgically repaired diaphyseal fractures of the femur.
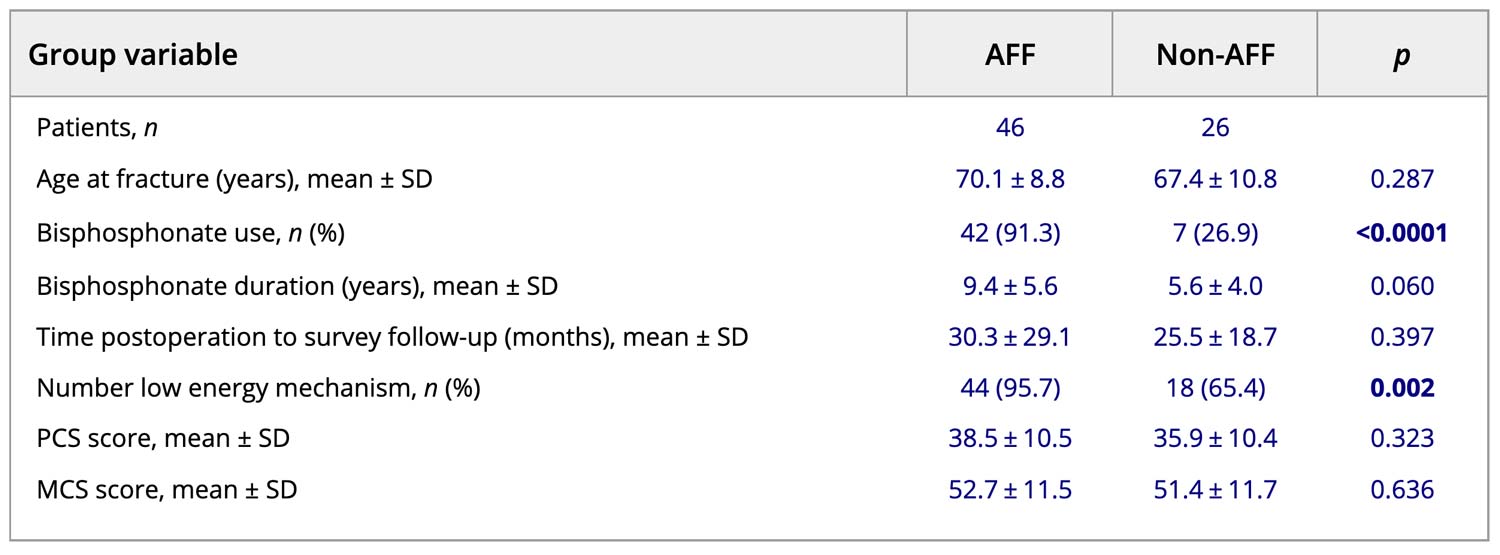
Table 1. Group Comparison
Conclusion
In spite of the small number of patients, to our knowledge, this is the first study to include standardized HRQOL outcomes, SF-36v2, for patients treated surgically for AFFs. The information presented will be useful to the practicing orthopedic surgeon and the medical community, particularly with regard to counseling patients on mid-term postoperative expectations after AFFs.
This article has been excerpted from “Health-related quality of life outcomes after surgical treatment of atypical femur fractures: a multicenter retrospective cohort study,” by the authors noted above, which was published in the September 2021 issue of the Journal of Bone and Mineral Research. 2021;5(11):e10514. doi: 10.1002/jbm4.10514. Editing has occurred, including the renumbering of tables, and references have been removed for brevity. Use is per CC BY 4.0.





