
The man who moves a mountain begins by carrying away small stones. Confucious
 By Taru Garthwaite, Tanja Sjöros, Saara Laine, Henri Vähä-Ypyä, Eliisa Löyttyniemi, Harri Sievänen, Noora Houttu, Kirsi Laitinen, Kari Kalliokoski, Tommi Vasankari, Juhani Knuuti, and Ilkka Heinonen
By Taru Garthwaite, Tanja Sjöros, Saara Laine, Henri Vähä-Ypyä, Eliisa Löyttyniemi, Harri Sievänen, Noora Houttu, Kirsi Laitinen, Kari Kalliokoski, Tommi Vasankari, Juhani Knuuti, and Ilkka Heinonen
Reduced sedentary time and increased light- and moderate- to vigorous-intensity physical activity had beneficial effects on several cardiometabolic risk markers in adults with metabolic syndrome.
The modern lifestyle has reduced daily physical activity (PA) demands in the recent decades, and now the majority of waking time (~8–9 h/day) is spent sitting. Physical inactivity and sedentary behavior (SB) increase the risk of chronic diseases and mortality, and SB has been adversely associated with cardiometabolic outcomes (eg, waist circumference [WC], HDL-cholesterol, triglycerides and insulin). Due to the accumulating observational evidence of the detrimental effects of sitting, an increasing number of interventions are targeting reductions in SB and investigating whether sitting less can improve health. As a major proportion of adults globally are insufficiently physically active, reducing SB instead of increasing PA may be a more feasible method for achieving health benefits.
Recent meta-analyses have shown that SB interventions can reduce sedentary time by 24–82 min/day and produce beneficial effects on common cardiometabolic outcomes (eg, weight, WC, blood pressure [BP], fasting insulin, HDL). However, previous interventions have mainly targeted healthy populations and occupational sitting, and the majority have lasted for less than 3 months or reported attenuations in SB reductions with longer follow-ups. Additionally, accelerometers are typically used only for ≤7 days at the beginning and end of interventions, which may not accurately reflect actual changes during the intervention or habitual behaviors. Thus, the current evidence of cardiometabolic benefits of reduced SB is limited, particularly in populations at increased cardiometabolic disease risk.
Therefore, we investigated the effects of a 3-month free-living intervention aiming at 1 h/day SB reduction on cardiometabolic outcomes in inactive sedentary adults with metabolic syndrome (MetS). In contrast to previous studies, accelerometers were used continuously throughout the intervention. In addition to the traditional cardiometabolic biomarkers, we investigated the effects on liver enzymes alanine aminotransferase (ALT), aspartate aminotransferase (AST) and γ-glutamyltransferase (GGT), which have not been studied in the context of SB reduction previously. These enzymes are markers of liver health, and they can thus provide novel and valuable information to further understand the effects of SB on metabolic health. We hypothesized that reduced SB, without intentionally adding exercise and moderate-to-vigorous PA (MVPA), has beneficial effects on cardiometabolic outcomes.
Methods
Sixty-four sedentary middle-aged adults with metabolic syndrome were randomized into intervention (INT; n=33) and control (CON; n=31) groups. INT participants were guided by a researcher in 1-hour tailored personal counseling sessions to sit less by increasing standing and light intensity PA (LPA), without intentionally adding exercise or MVPA. Ways to increase standing and LPA were discussed individually according to participants’ preferences, and could include eg, use of sit-stand desks, standing during phone calls and taking stairs instead of elevators. CON was instructed to maintain usual habits. Sedentary behavior, breaks in sedentary behavior, standing, and physical activity were measured for 3 months with hip-worn accelerometers connected via a cloud system to an interactive smartphone application. Fasting blood sampling and measurements of anthropometrics, body composition, and blood pressure were performed at baseline and at 3 months. Linear mixed models were used for statistical analyses. (Full details are available in the online article.)
Results
Sixty-three participants completed the 3-month intervention period (mean duration 3.2 [0.6] months). Only one participant dropped out (personal reasons). The mean age was 58 (SD 7) years, and 37 participants (58%) were women; 41% of the participants were overweight and 59% obese. At baseline, the participants spent 10.04 (SD 1.01) h/day sedentary, 1.79 (0.59) h/day standing, 1.74 (0.44) h/day in LPA, and 0.97 (0.32) h/day in MVPA and took 5149 (1825) steps and 29 (8) breaks in SB daily.
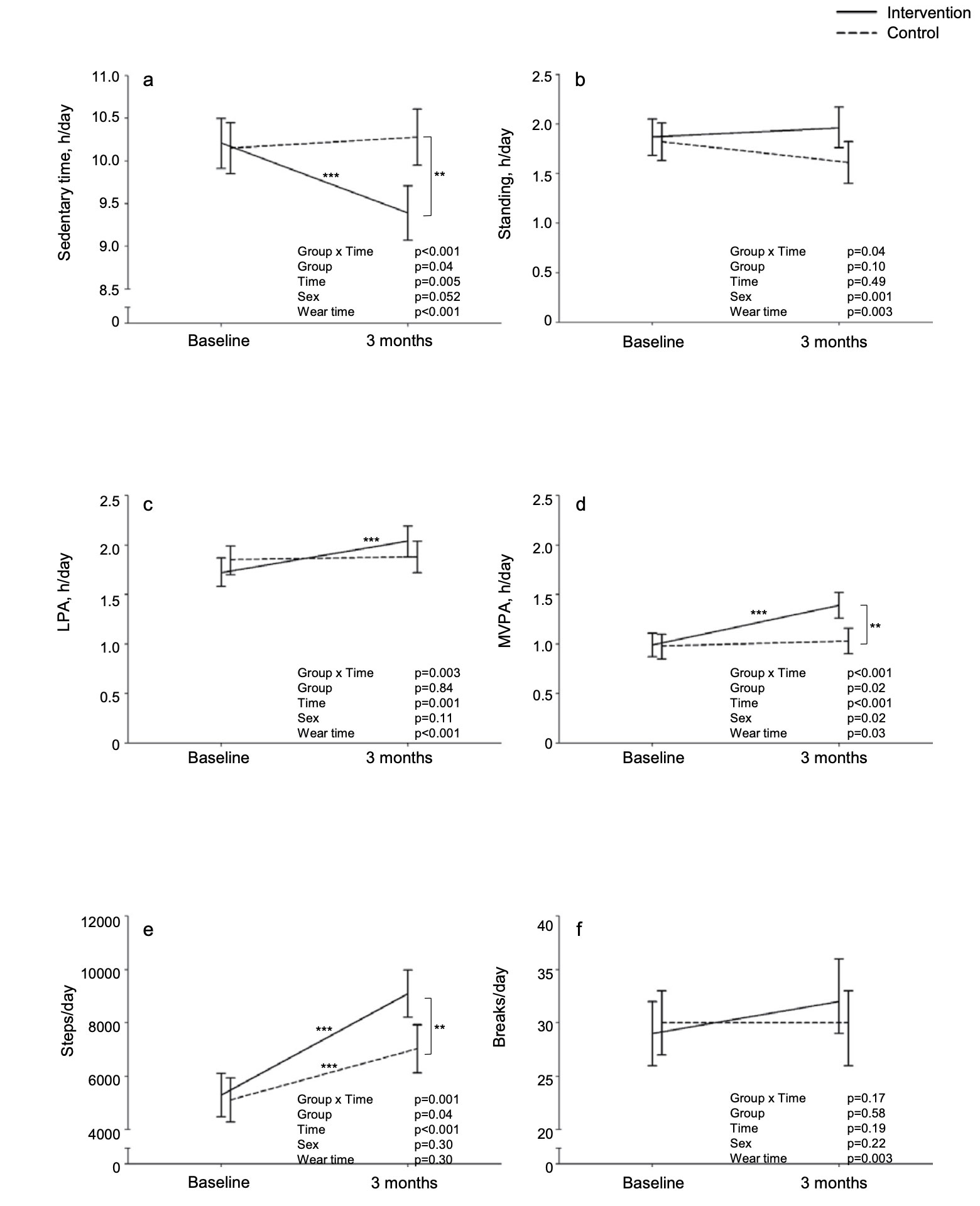
Figure 1. The intervention effects on activity outcomes. a) Sedentary time (h/day), b) standing (h/day), c) light-intensity physical activity (h/day), d)moderate-to-vigorous physical activity (h/day), e) steps/day, and f) breaks in sedentary time/day at baseline and throughout the 3-month intervention in sedentary, inactive adults with metabolic syndrome. Baseline indicates daily mean (95 % CI) of a continuous 1-month screening accelerometer measurement, and value at 3 months indicates daily mean (95 % CI) of continuous accelerometer measurement throughout the 3-month intervention. Solid line represents the intervention group and dashed line the control group. **= Tukey’s P < 0.01; *** = Tukey’s P < 0.001.
Valid accelerometer data from the intervention period is available for 50 participants (78%; n = 25 in both groups); missing data is due to data transfer issues between the accelerometers and the cloud system. The median of valid accelerometer days was 61 (Q1 37, Q3 73, range 7–99), and the accelerometers were worn for 15.11 (SD 0.75) h/day during the intervention. Wear time was ~35min/day longer during the intervention compared to the screening in both groups. In SB, LPA, MVPA, standing time and steps/day the mean changes from baseline to 3 months were significantly different between groups (Fig. 1). In more detail, INT reduced SB by ~50 min/day (95 % CI: 24, 73; 8% of daily baseline SB) primarily by increasing LPA (19 [8, 30] min/day) and MVPA (24 [14, 34] min/day). CON did not significantly change SB, LPA, or MVPA. Standing time increased slightly and not statistically significantly in INT (6 [−11, 23] min/day) and decreased in CON (−13 [−30, 5] min/day). Both groups increased steps/day, but the increase was greater in INT compared to CON: 3800 (2685, 4195) vs. 1918 (801, 3036) steps/day. Breaks in SB did not significantly change in either group.
Significant intervention effects favoring INT occurred in fasting insulin (INT: 83.4 [68.7, 101.2] vs. CON: 102.0 [83.3, 125.0] pmol/l at 3 months), insulin resistance (HOMA-IR; 3.2 [2.6, 3.9] vs. 4.0 [3.2, 4.9]), HbA1c (37 [36, 38] vs. 38 [37, 39]mmol/mol), and liver enzyme alanine aminotransferase (ALT; 28 [24, 33] vs. 33 [28, 38] U/l). The effects mainly occurred due to increases from baseline to 3 months in CON that exceeded any changes in INT. In triglycerides and heart rate, within-group changes were non-significant despite significant overall intervention effects.
Waist circumference (WC), body fat %, fat mass, systolic blood pressure, and diastolic blood pressure decreased slightly during the intervention with no difference between groups. Fasting glucose; fat free mass (FFM); total, LDL- and HDL-cholesterol; aspartate aminotransferase (AST); and γ-glutamyltransferase (GGT) increased similarly in both groups. Weight or BMI did not change in either group.
Changes in standing time were inversely correlated with weight and BMI changes, and changes in the number of steps/day correlated inversely with WC changes. Changes in MVPA correlated positively with HDL changes. Changes in weight and BMI correlated positively with changes in triglycerides and BP, and changes in WC also correlated positively with changes in BP. Changes in FFM correlated inversely with changes in fasting glucose.
Discussion
Our results indicate benefits in several cardiometabolic outcomes with reduced SB in sedentary adults with MetS. A 50min/day reduction in SB and subsequent increases in LPA and MVPA (consisting mainly of moderate-intensity PA) had beneficial effects on fasting insulin, HOMA-IR, HbA1c and ALT, but it was not able to prevent worsening in all biomarkers. Reducing daily SB may be helpful in cardiometabolic disease prevention in risk populations, but a more substantial SB reduction and/or higher volume and intensity of PA is likely needed for sedentary individuals to achieve greater health benefits. To our knowledge, this is the first study to measure SB and PA with accelerometers continuously throughout the 3-month intervention, and to investigate the health effects of SB reduction in sedentary and inactive, middle-aged adults with MetS. Compared to a population-based sample of Finnish adults of similar age, our participants spent 1.5 h more sedentary and had ~1 h less LPA and ~30 min less MVPA daily.
The effects of free-living SB interventions on cardiometabolic health have been recently synthesized in two meta-analyses. Hadgraft et al (2021) reported improvements in anthropometrics, BP, insulin, and lipids in healthy populations, but SB changes were not analyzed. In clinical populations (overweight/obesity; type 2 diabetes; cardiovascular, neurological/cognitive and musculoskeletal diseases) ~1-hour SB reduction improved HbA1c, body fat % and WC. Similar to our findings, others have also reported benefits in HbA1c, fasting insulin and HOMA-IR following SB interventions. SB reduction may also improve fasting glucose, total cholesterol, body fat %, WC, and clustered cardiometabolic risk score. On the other hand, not all interventions have been effective in reducing SB, or improving cardiometabolic outcomes despite SB reductions.
Our study complements and extends this limited and inconsistent evidence. It seems that sitting less may be beneficial particularly from type 2 diabetes prevention perspective, as we found benefits in markers of glucose metabolism and diabetes risk (i.e., fasting insulin, HOMA-IR, HbA1c), in line with previous findings. In addition to the traditional cardiometabolic biomarkers, the intervention effect favoring INT on liver enzyme ALT is a novel finding that, to our knowledge, has not been reported previously. The intervention effects on liver enzymes AST and GGT also were near-significant (group × time P = 0.057 and P = 0.071, respectively). These enzymes are markers of liver dysfunction or injury, and are most often elevated due to non-alcoholic fatty liver disease, which is considered the hepatic expression of MetS. SB has been associated with fatty liver, but SB interventions have not studied effects on liver health markers. Elevated ALT and AST are associated with obesity and dyslipidemia, and they independently predict type 2 diabetes. It may have an important impact on public health and disease prevention in risk populations if benefits in several diabetes risk markers can be achieved with SB reductions.
Although the intervention aimed to reduce SB primarily by increasing standing and LPA, both LPA and MVPA increased. Standing time also increased slightly (6 min/day), but non-significantly. A recent meta- analysis of free-living interventions in clinical populations by Nieste et al (2021) reported a comparable ~60 min/day SB reduction, but in contrast to our study SB was mainly replaced by standing and low-intensity walking, with no change in MVPA. It is noteworthy, however, that the MVPA amount is dependent on analysis methods. In our study, the total MVPA amount also includes short and sporadic MVPA bouts as we analyzed the accelerometer data in only 6-second epochs. Steps increased in our study as well, and the increase correlated with the MVPA increase, suggesting that the participants may have found it easier to reduce SB by walking at a moderate pace than by standing and incorporating LPA into daily activities. Reallocating SB to different behaviors, and the composition of behaviors across the 24-h day, affects health outcomes differently. Replacing SB with standing has been shown to improve glycemic outcomes and fat mass, while reallocating SB to LPA or MVPA appears beneficial for glycemic outcomes, lipids and WC. Although replacing SB with any intensity PA is beneficial, the greatest benefits are achieved with the reallocation of SB to MVPA.
Conclusion
Reducing daily SB by 50 min and increasing LPA and MVPA resulted in beneficial effects in several cardiometabolic risk markers in adults with MetS in 3 months, but it was not enough to prevent increases in all biomarkers. More substantial reduction in SB and/or structured exercise may be needed for sedentary individuals to achieve greater health benefits. However, sitting less may provide an additional approach to aid in chronic disease prevention in high-risk populations.
This article has been excepted from “Effects of reduced sedentary time on cardiometabolic health in adults with metabolic syndrome: A 3-month randomized controlled trial,” by the authors noted above, which was published online on April 7, 2022, in Journal of Science and Medicine in Sport; 2022;25(7):579-585. doi: 10.1016/j.jsams.2022.04.002. Editing has occurred, including the renumbering of tables, and references have been removed for brevity. Use is per CC BY 4.0.





