Dirty Truth #3: What We Can’t See Is Key

What We Can’t See Is Key: Many biomechanical characteristics can be seen by the naked eye but are better visualized and quantified with computers, which can capture the unseen.
By Jay Segel, DPM; Sally Crawford, MS
In the last 2 installments, we talked about our problematic foot anatomy and what happens to the structure during weightbearing and activity. Much like how a mousetrap precisely captures its target, analyzed computer-aided gait analysis (CAGA) reports accurately “mousetrap” and track the unseeable, providing valuable insights and objective data.
Consider the common biomechanical and structural foot problem, equinus. Many sources describe equinus in gait terms by noting an early heel off, such as a heel leaving the support surface at 55% of the gait cycle. Through visual gait observation, we may note that the heel indeed leaves the ground early, but we cannot assign a quantitative percent value, thus deciding the severity of the equinus deformity without CAGA: mild, moderate, and severe.
Delving further into diagnostic nuances, early metatarsal onset times also point to dropfoot. So, how do we differentiate between these 2 conditions? CAGA offers the precision required to distinguish Dropfoot and Equinus as an example. Near-instantaneous start times suggest dropfoot, while times falling between near-instantaneous and normative values lean toward an equinus diagnosis (Figure 1).
The ability to monitor and document baselines and progress objectively is an obvious advantage of CAGA. However, the greatest value may be in leveraging the data as treatment planning (Figure 2). In the clinical setting, CAGA is our main tool in creating comprehensive treatment plans. Let’s examine another serious issue: the diabetic ulcer. Without a precise solution, diabetic ulcer recurrence can range upwards of 71.2% as determined in a recent study.1
In podiatric care clinics like Johns Hopkins, the use of CAGA extends beyond identifying at-risk areas and designing precise offloading solutions like custom orthotics to prevent or treat diabetic ulcers and even ulcer recurrence. CAGA brings to light device efficacy and guides adjustments for improved care. Additionally, CAGA empowers patients with a deeper understanding of their progress, and in turn, this enhanced comprehension fosters greater adherence and compliance with plans.

Figure 1: CAGA as diagnostic tool. When evaluating the “unseen” aspects of this equinus deformity case, the interplay between heel-strike and mid-stance gait phases is noteworthy. Consequently, we can view “early Mets on” as an additional element in CAGA. The onset timing of pressure under the metatarsal heads (early Mets on) serves as a dependable marker for this deformity, though one might observe the trait without quantifying it precisely.
As one can imagine, with over 255 temporal-spatial parameters and graphs, combined with the period of foot disorders, we could go on all day, but there is one last point to highlight in this “dirty truth”: symmetry and normality. You can’t create a good plan without the CAGA data and the normative data comparison and asymmetry scores (Figure 3, page 22).
An ideal analogy to the understanding and cost of asymmetry between limbs is that of car axles and tires. Car tire-wear is not even from left to right or from inside and outside in a specific tire. Left untreated, that asymmetric wear will not only cause problems with the rubber tires, but with the axles and eventually the whole car structure, not to mention drivability. We experience the same types of wear and tear, but unfortunately, we can’t just change our feet as we can the tires of the car. Instead, we must be particularly focused on asymmetry wear and tear, which leads to heat, fatigue, inflammation, arthritis, deformation, and eventually pain coupled with limitation of ambulation. Fortunately, we have a tool that allows us to catch asymmetry in the earlier stages and intervene with a targeted treatment protocol to arrest this erosive problem: yes, it’s CAGA analysis. These detailed reports lay bare to the trained eye, medial-to-lateral and left-to-right asymmetries for treatment consideration. A useful adage to consider when thinking about intervention is, “Change your orthotics, not your joints.” So, we think it’s clear that what we can’t see is key, or maybe what we should say is, what we can see with CAGA is key.
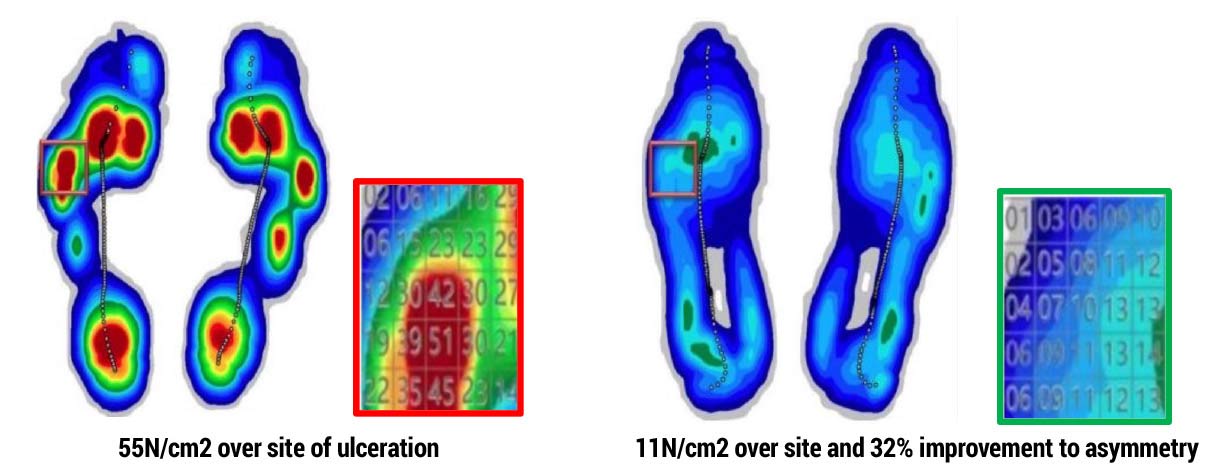
Figure 2: CAGA as treatment planning tool. Identify areas at risk with specificity and design offload mechanisms, such as those built into an orthotic, to protect these areas of concern. After creating such solutions, we can also objectively judge their efficacy and make any corrections needed to the device (78.43% reduction in pressure achieved with 32% improvement in asymmetry).1
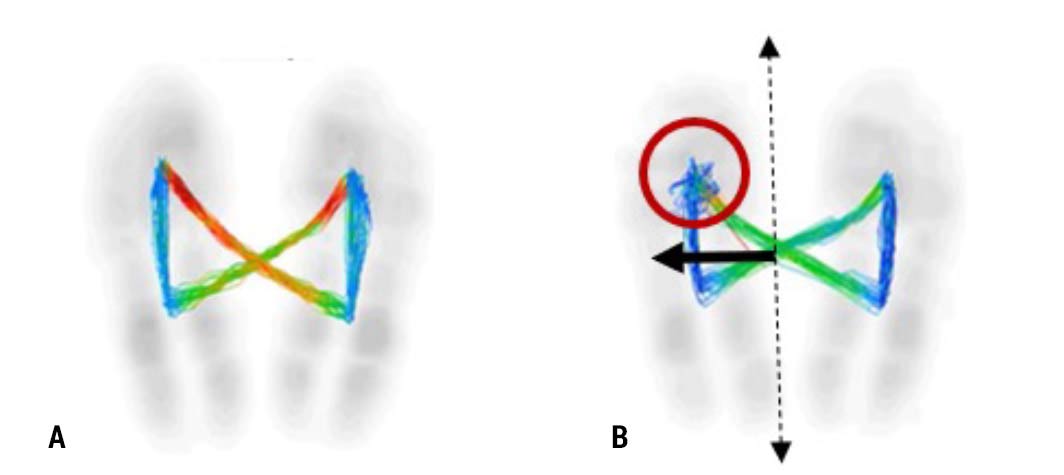
Figure 3: Comparison of A) Balanced single support phase center of pressure with Lateral Shifting at 0mm, perfect alignment, versus B) Unbalanced single support phase center of pressure intersection with variability and >8mm lateral shifting and malalignment.
- Kochar K, Priesand S, Yosef M, Schmidt BM. Diabetic foot infection severity as a predictor of re-ulceration following partial forefoot amputation. J Foot Ankle Surg. 2025;64(3):238-242. doi: 10.1053/j.jfas.2024.10.012.






Thank you for this study. My initial viewing of this single-phase support stance had me thinking of a few things. Was there a Leg length discrepancy? Were any other medical diagnoses given, such as the beginning of Charcot, or was any hip or stiff ankle present? Was subtalar neutral used when creating the mold for the orthotic device to be used? Does the CAGA also indicate if shoe modifications may be needed to help with severe pes cavus or planus feet? Does Medicare or any insurance cover this type of diagnostic intervention with the supporting orthotic device? what style of shoe is used to accommodate this device to offload the ground reaction forces? Is the patient obese or high BMI? Does this CAGA also help in all moments of gate showing before and after with the device created? Was the casting of the feet for an orthotic done sitting or semi-weight bearing? Were any rigid materials used in the creation of this device to offload the pressure points created at midstance? If a partial foot amputation is present, could a previous device that has been used be modified, or is a new device always indicated?
These are some of the things I would look for when creating a device for a diabetic client with or without partial foot amputation.
Is there a mistake in figure 1? The table is not labelled with what the numbers represent but I assume they are percentage of the gait cycle. On the right table for equinus, why then is 1st metatarsal contact at 59.5% of the gait cycle when this is for an equinus foot? 59.5% would be for a foot that is remaining too long on the heel with delayed forefoot contact. Perhaps this is supposed to be labelled the heel off timing rather than 1st met contact?