
 By Dr. Hooman MIR, DPM, MSci, FAPWCA
By Dr. Hooman MIR, DPM, MSci, FAPWCA
The ankle is a complex and dynamic joint essential for load transfer, balance, and ambulation. This review presents a 360° exploration of ankle biomechanics by integrating structural anatomy, neuromuscular control, and the biomechanical principles that govern function and dysfunction. Recent data from detailed cadaveric, imaging, and biomechanical studies are incorporated to enhance understanding of ligament function, motion coupling, and injury mechanisms. Emphasis is placed on the anatomical and biomechanical principles necessary to guide clinical diagnosis, rehabilitation, and surgical planning for podiatric and orthopedic specialists.
Ankle biomechanics reflects a sophisticated interaction between osseous configuration, ligamentous restraints, muscular coordination, and sensorimotor feedback. These elements function in concert to permit the joint’s role in dynamic stability and force propagation. Disruptions–whether through trauma, degenerative changes, or congenital anomalies–result in significant mobility impairments. This review builds upon foundational anatomy and integrates clinical insights to present a comprehensive view of ankle biomechanics from normal to pathological states, with application to podiatric and foot/ankle surgical practice.
1. Osteology and Joint Configuration
 The ankle, or talocrural joint, is a synovial hinge joint formed by the distal tibia, fibula, and the superior dome of the talus. The mortise configuration permits dorsiflexion and plantarflexion, with transverse tibiotalar rotation accommodated through minimal fibular mobility. The talar trochlea is broader anteriorly, contributing to inherent joint stability in dorsiflexion.
The ankle, or talocrural joint, is a synovial hinge joint formed by the distal tibia, fibula, and the superior dome of the talus. The mortise configuration permits dorsiflexion and plantarflexion, with transverse tibiotalar rotation accommodated through minimal fibular mobility. The talar trochlea is broader anteriorly, contributing to inherent joint stability in dorsiflexion.
The subtalar joint, comprising the talus and calcaneus, is oblique in orientation and supports inversion-eversion and pronation-supination. The transverse tarsal joint (talonavicular and calcaneocuboid) complements subtalar motion to accommodate uneven surfaces. These articulations together enable triplanar motion essential to ambulation.
Clinical Insight: The talus, devoid of muscular attachments, depends on ligamentous and articular congruity for stability. Pathology affecting its alignment or integrity–eg, talar dome osteochondral lesions–disrupts both load transmission and proprioception.
2. Ligamentous Anatomy and Functional Roles
 Lateral Ligament Complex
Lateral Ligament Complex
The lateral ankle ligaments, anterior talofibular (ATFL), calcaneofibular (CFL), posterior talofibular (PTFL) are the primary static stabilizers against inversion.
- ATFL: Most commonly injured ligament. Biomechanically resists anterior talar displacement during plantarflexion. Often composed of 2 bands.
- CFL: Spans talocrural and subtalar joints. Maintains tension throughout ankle range of motion (ROM), providing restraint to inversion in dorsiflexion.
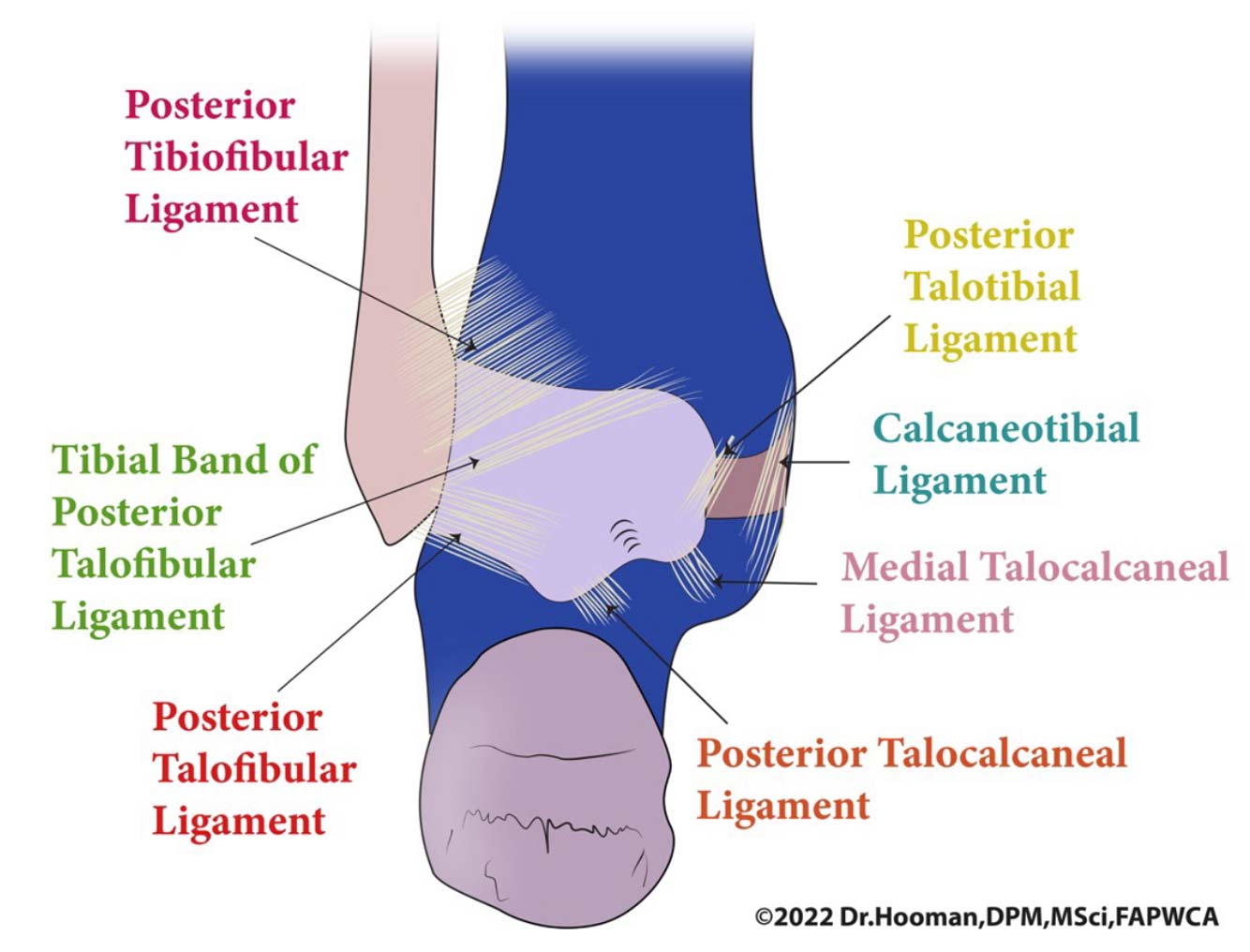
- PTFL: Rarely injured unless in dislocation. Supports talus in dorsiflexion.
Medial (Deltoid) Ligament Complex
Composed of superficial and deep fibers. Provides stability against eversion and external rotation. Bands include:
- Tibionavicular
- Tibiocalcaneal
- Posterior Tibiotalar (deep and superficial portions)
These ligaments are reinforced by the posterior tibial tendon sheath and span the talus, navicular, and calcaneus.
Syndesmotic Ligaments
The anterior inferior tibiofibular ligament (AITFL), posterior inferior tibiofibular ligament (PITFL), and interosseous membrane form a fibrous articulation stabilizing the distal tibia and fibula. Integrity of this complex is vital for mortise congruency and resisting diastasis.
Functional Insight: ATFL and CFL are sequentially injured during inversion sprains. Injury grading and MRI often reveal disruption patterns guiding management from conservative to surgical.
3. Muscular Coordination and Tendinous Stabilizers
Primary Ankle Movers:
- Dorsiflexors: Tibialis Anterior, Extensor digitorum Longus (EDL), Extensor Hallucis Longus (EHL)
- Plantarflexors: Gastrocnemius, Soleus, Tibialis Posterior, Flexor Digitorum Longus (FDL), Flexor Hallucis Longus (FHL)
Lateral stabilizers: Peroneus Longus and Brevis
Medial stabilizers: Tibialis Posterior
Peroneals are particularly critical in controlling inversion moments and preventing recurrent ankle instability.
Dynamic Stabilization
Tendon sheaths and retinacula (superior/inferior extensor and peroneal retinacula) prevent bowstringing and contribute to proprioceptive input. Reflexive muscle activation during gait prevents excessive motion and redistributes loading.
Clinical Relevance: Chronic Ankle Instability is often a combined result of ligamentous laxity and peroneal muscle dysfunction. EMG studies reveal delayed peroneal firing in such patients.
4. Neuromechanics and Proprioception
 Joint mechanoreceptors within ligaments and tendons contribute to afferent input critical for maintaining balance and adaptive movement. Disruption due to ligament injury (eg, ATFL tear) reduces joint position sense and increases reinjury risk.
Joint mechanoreceptors within ligaments and tendons contribute to afferent input critical for maintaining balance and adaptive movement. Disruption due to ligament injury (eg, ATFL tear) reduces joint position sense and increases reinjury risk.
Balance training and sensorimotor re-education are essential in rehabilitation to restore neuromuscular control.
5. Pathological Biomechanics: From Instability to Impingement
Chronic Ankle Instability (CAI)
Results from repetitive sprains with incomplete healing. Features include:
- Mechanical Laxity (Positive Anterior Drawer/Talar Tilt)
- Functional Instability (Subjective giving way)
Associated with peroneal weakness, impaired proprioception, altered gait kinetics. May require ligament reconstruction (Broström-Gould) in surgical cases.
Ankle Impingement Syndromes
Can be Anterior, Posterior, or Anterolateral.
- Anterior: Osteophyte formation impedes dorsiflexion.
- Posterior: Posterior talofibular or intermalleolar ligament impingement, often in ballet or soccer athletes.
Insight from Cadaveric Studies: Golanó et al. emphasize the Anatomical variations and multifascicular nature of the posterior intermalleolar ligament, implicated in posterior impingement.
Post-Traumatic OA and Malalignment
Repetitive microtrauma and malreduction after fracture can alter ankle load distribution. Talocrural cartilage has a lower tolerance to shear; incongruity quickly leads to degenerative changes.
6. Advances in Surgical Biomechanics
Surgical planning now integrates 3D imaging, motion analysis, and anatomical reconstruction techniques. procedures like anatomic lateral ligament reconstruction or syndesmotic repair rely on detailed knowledge of ligament insertion points and tensioning angles.
- Reconstruction Orientation must match the normal strain path of ligaments.
- Arthroscopy enables direct visualization of subtle lesions, including capsuloligamentous and posterior Impingement sources.
Future Direction: Use of AI in preoperative simulations and robotic assistance is emerging to optimize tensioning and placement.
7. Educational Implications for Foot and Ankle Specialists
 A precise understanding of anatomy-informed biomechanics is foundational to:
A precise understanding of anatomy-informed biomechanics is foundational to:
- Interpreting radiographic and MRI findings
- Performing accurate surgical reconstructions
- Designing rehabilitation protocols
Teaching methods should incorporate cadaveric dissections, motion capture, and immersive simulations such as Anatomage® and HoloLens® technologies used at UTRGV, School of Podiatric Medicine.
Integration of Visual Learning with functional load scenarios enhances retention among podiatric medical students.
Conclusion
The ankle is more than a hinge–it is a dynamically stabilized joint reliant on precise anatomical, ligamentous, neuromuscular, and proprioceptive interactions. A full 360° understanding of its biomechanics–grounded in anatomical detail–is essential for foot and ankle specialists aiming to diagnose, treat, and rehabilitate both acute and chronic conditions.
With ligament morphology more variable than traditionally assumed, and functional pathology often hidden until late stages, integrating clinical imaging with deep anatomical knowledge becomes indispensable. the application of advanced imaging, surgical planning software, and educational technologies will further refine how clinicians understand and approach this critical joint.
Dr. Hooman Mir, DPM, MSci, FAPWCA, is a Tenure-Track Assistant Professor of Medicine and Faculty Senator at UTRGV School of Podiatric Medicine. Dr. Mir is an alumnus of Temple University School of Podiatric Medicine and completed his surgical internship at Mount Sinai Hospital in New York. Dr. Mir’s commitment to podiatric academic medicine is defined by a series of distinctive firsts: the first Doctor of Podiatric Medicine (DPM) to receive full NIH tuition reimbursement for a Master of Science in Clinical Investigation at UT Health San Antonio; the first DPM to graduate from Harvard Medical School’s prestigious T2T Program; the first DPM and only faculty member in the UTRGV Health System inducted into the historic Harvard Club of Boston; and the first DPM at UTRGV Health System ever to be accepted into the School of Medicine’s PhD program in Human Genetics–focused on Precision Medicine in Diabetes–now embarking on his second year of doctoral study.
- Golanó P, et al. Anatomy of the ankle ligaments: a pictorial essay. Knee Surg Sports Traumatol Arthrosc. 2010;18(5):557–569.
- de Asla RJ, et al. Functional anatomy of the foot and ankle. J Bone Joint Surg Am. 2006;88(Suppl 1 Pt 2):1–9.
- Vega J, et al. Ankle impingement syndromes. Foot Ankle Clin. 2006;11(2):375–389.
- Ferran NA, et al. Clinical review: The biomechanics of lateral ankle instability. Br J Sports Med. 2009;43(4):293–297.
- Hintermann B, et al. Biomechanics of the unstable ankle. Clin Sports Med. 2002;21(3):615–627.
- van Dijk CN, et al. The posterior ankle: anatomy and function. Arthroscopy. 2000;16(6):674–679.
- Bonnin M, et al. Biomechanics of the foot and ankle. Foot Ankle Surg. 2020;26(4):285–294.
- Karlsson J, et al. Surgical treatment of chronic lateral instability of the ankle joint: a new technique. Am J Sports Med. 1989;17(2):268–273.
- Siegler S, et al. The mechanical characteristics of the ankle joint. Foot Ankle. 1988;8(2):75–81.
- Sammarco GJ, et al. Biomechanics of the ankle joint complex. J Am Acad Orthop Surg. 2004;12(4):227–236.
- Tourné Y, et al. The ligaments of the ankle. Surg Radiol Anat. 2010;32(8):653–665.
- Kelikian AS, Sarrafian SK. Sarrafian’s Anatomy of the Foot and Ankle. 3rd ed. Lippincott Williams & Wilkins; 2011.






This article offered substantial insight and was highly beneficial in enhancing my medical understanding.
🙏🙏🙏🙏