

Ask any woman who’s been through it, and they’ll easily confirm: Pregnancy is a life-changing event with numerous hormonal, physiological, morphological, functional, and biomechanical adaptations. Here we summarize and excerpt a round-up of recent research findings that show the impact of pregnancy on tendons in the lower extremity, on foot loading and plantar pressures in gait, and on morphological and postural changes in the foot, as well as the benefits of compression stockings during this unique period.
Changing Tendons
As the need for physical activity, or at least non-sedentary behavior becomes more evidence-based for the general population, many clinicians find that encouraging pregnant women to be more active can be met with resistance as the specific evidence base is scant at best for this group. The ongoing weight gain of a healthy pregnancy leads to a constant change in one’s center of mass which requires a compensation in motor response—often altering foot and ankle biomechanics, making many women feel unstable and therefore unwilling to take what they perceive as any unnecessary risk. But times are changing and with the advent of published guidelines encouraging women to be physically active throughout their pregnancy, many of today’s women of child-bearing age are taking up—and maintaining during pregnancy—not only strength training but vigorous-intensity activities.1 While this trend is to be commended, the potential for increased musculoskeletal injury cannot be ignored.
While most would agree that physical activity can be healthy for the mother and fetus, it is also true that the many hormonal changes of pregnancy can affect the musculoskeletal system in ways that are only beginning to be studied. Writing in a recent case study in the Journal of Applied Physiology, Waugh and Scott1 note that such hormonal changes could increase the risk of soft tissue injury. They cite the known gender differences in injury rates for the anterior cruciate ligament (ACL), which have made it a target for research related to relaxin, estrogen, progesterone, and testosterone. In addition to pregnancy, these sex hormones are known to fluctuate during monthly menstrual cycles as well. For example, they note the elevated levels of estrogen (10- to 100-fold) during the preovulatory phase of the menstrual cycle are associated with reduced tissue stiffness and increased injury rates, such as increased ACL laxity causing knee displacement.
In their case study, they were able to collect connective tissue properties on load-bearing tendons from a single recreationally active individual during 2 successive pregnancies. Using a variety of techniques, they evaluated morphological, mechanical, and functional properties of the Achilles, ACL, and mid-patellar tendons, as well as gait kinematics and kinetics. Their findings show subtle changes in tendon organization and stiffness throughout the course of the pregnancy and into parturition. The authors conclude by calling for further study of musculoskeletal adaptations during pregnancy, particularly as they relate to both increasing physical activity and injury risk.
Biomechanics
Writing in the Journal of Functional Morphology and Kinesiology, Conder et al2 highlight the numerous biomechanical and hormonal changes of pregnancy as they relate to spinal curvature, balance, and gait patterns as well as quality of life (QOL) changes such as back pain and the increased risk of falls. In their systematic review of 50 research papers, they found that angles of lordosis and kyphosis are significantly—though not consistently—increased in pregnancy. Back pain is significantly increased in pregnant women, although this is not significantly correlated with spinal changes. Increased movements of center of pressure (COP) and increased stability indexes indicate postural control is reduced in pregnancy.
Specifically related to static stability and visual cues, the authors found that when women are asked to keep their eyes open, stability has been shown to improve and in conditions that require women to keep their eyes closed, path length of the COP is increased by pregnancy. It is reported that the condition of closing eyes affected both pregnant and non-pregnant women in the same way, and it is concluded that the destabilization is due to poor somatosensory processing rather than anatomical changes of pregnancy. This highlights the importance of visual cues for the maintenance of balance. Interestingly, in instances where the eyes are closed, sufficient balance has instead been maintained by spreading the feet apart. The idea here is that increasing the width of the stance increases the base of support and therefore is an attempt to improve stability and lateral balance.
Joint Kinematics: As for joint kinematics, some studies show that there are significant reductions in the peak hip flexion and peak hip extension in the sagittal plane during the second and third trimester of pregnancy compared to non-pregnant women. In the frontal plane, there is conflicting evidence whereby some studies report higher hip adduction in pregnant women during gait, whereas others report larger peak hip adduction angles in postpartum women. This may be due to comparing pregnant women to different sorts of controls, where some studies use non-pregnant women and others use postpartum measurements of the same women. Decreased thigh abduction is observed in the developing pregnancy and compared to non-pregnant women. In the transverse plane, peak external rotations (lateral and medial) of the hip are shown to be significantly higher in pregnant women, and these are at their highest in the third trimester. In an interesting study, Branco et al3 report that in terms of hip joint power, there are significant predictors in pregnant women. It was observed that thigh fat area is a significant predictor of hip joint power during the second trimester, while body weight is a significant predictor of hip joint power during pregnancy.
The knee joint shows increased maximum flexion sagittally in the developing pregnancy, while displaying significant reductions in maximum extension of the knee when compared to non-pregnant women.
Regarding the ankle, increased inversion and eversion are observed in both the developing pregnancy and when compared to controls in the frontal plane. This coincides with increased rotation of the foot during pregnancy, tending toward pronation. A significantly reduced plantar flexion is also observed during pregnancy. However, there are also studies that have found no significant changes to the ranges of motion in the ankle, knee, and hip, including no changes to ankle inversion/eversion and knee flexion/extension.
It is likely that these kinematic effects are connected in some way, especially since it is known that an increased pelvic tilt can reduce the flexion moment in the hip. The literature makes little reference to changes in the adduction of the knee joint. There is evidence suggesting that increased inversion and eversion in the ankle (observed in pregnancy) can result in reduced adduction of the knee. This should be explored further in relation to the effects of pregnancy
Body Mass: Body mass significantly increases with the developing pregnancy, while the trunk becomes longer and abdominal girth significantly increases. This increase in body mass is most significant in the third trimester. Increases can also be observed in the breadth of the thorax, girth of the gluteals, girth of the calves, and biceps and tricipital skinfolds during pregnancy. Furthermore, there is an increase of fat in the calves observed as well as a significant reduction in calf muscle. However, changes of this likeness are not observed in the thighs. In terms of the foot, pregnant women display a significantly reduced arch between the first and third trimesters, as well as a significant increase in the width of the foot. This results in an increased area of contact between the middle of the foot and the floor as well as the lateral heel. An increased pressure in the second metatarsal of the foot was also observed in the third trimester compared with both earlier pregnancy and postpartum. Findings also show that pregnant women have higher recorded Foot Posture Indices (FPI) in the third trimester. An increase in FPI describes the foot of a pregnant woman late in her pregnancy.
It is known that water retention is increased in pregnancy, particularly in the ankles, which is a likely explanation for the increase in foot width and contact with the floor. Also, higher relaxin levels may play a role in relaxing the plantar fascia, the ligament on the sole the foot that supports the arch. A weakened plantar fascia combined with increased weight from pregnancy pushing downward is a likely explanation for a reduced arch height, and thus an increase in foot contact with the floor. In terms of QOL, associations have been made between higher reported pain levels in women with flat feet in the general population.
Trunk range of motion, hip flexion, and extension are reduced, stride length and gait velocity are decreased, and step width increased; again, not consistently. It is likely that each woman adopts unique techniques to minimize the effects, for example increasing step width to improve balance. Further research should focus on how altered limb kinematics during gait might affect QOL by influencing the human body, as well as assessing parameters in all planes to develop a wider understanding of pregnant biomechanical alterations.
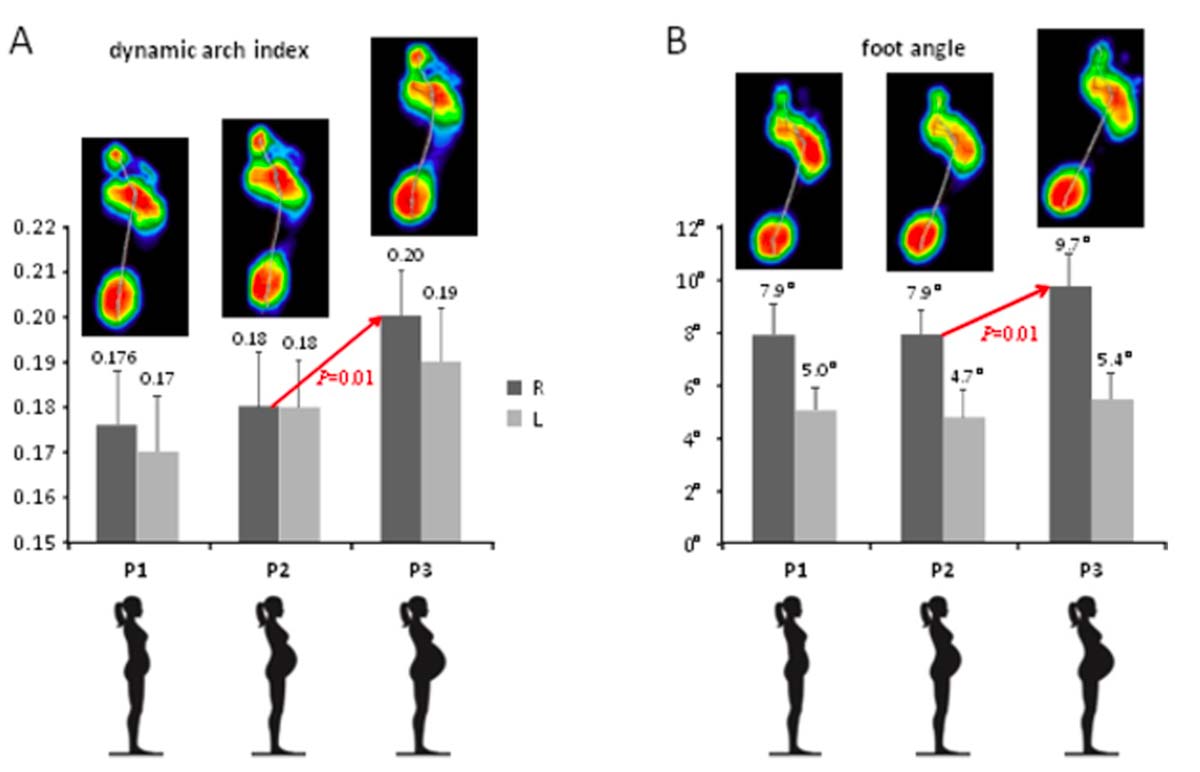
Figure. Foot loading characteristics in the 1st (P1), 2nd (P2) and 3rd (P3) trimesters of gestation. A–dynamic arch index (mean±SD). B–foot angle (mean±SD). Upper color footprints in A and B illustrate examples of averaged right foot pressure distribution patterns of individual subjects in the 1st, 2nd and 3rd trimesters of gestation.
Plantar Pressures, Flattening Arches
In a recent study out of Poland that was published in PLoS One, Maslon et al4 sought to understand how pregnancy affects foot loading patterns in gait and if it is related to the body’s adjustments to the growing fetus over the course of the pregnancy. They looked at 30 women in 3 sessions, 1 in each trimester of pregnancy (P1, P2, P3). They took anthropometric measures of body mass and waist circumference, and the women did walking trials at a self-selected speed along a ~6m walkway, with vertical pressures recorded via a force plate in the middle of the walkway.
In what appears to be the first longitudinal study in which the relation between abdominal size and plantar pressure distribution pattern was analyzed, their findings show that the correlation of individual foot loading parameters across different trimesters was relatively high, more noticeably for dynamic longitudinal arch index (DAI) and foot angle (r~0.9) and less for the medial lateral index, and forefoot-rearfoot index measurements (r~0.5–0.8). Nevertheless, there were also changes depending on the phase of pregnancy. Plantar pressure alterations that occur during pregnancy may be related to both biomechanical factors and gait adaptations.
Arch Flattening: Foot arch flattening during gait was evaluated by measuring the DAI parameter, which correlated with the body mass in all trimesters, consistent with the influence of individual biomechanical factors (eg, internal loads related to the anatomical structure of the body) on foot loading. An increased body mass generally evokes changes in the height of the foot arch during posture; the higher the weight, the more significant changes can be observed, resulting in the increase in midfoot contact area and midfoot plantar pressure in late pregnancy. Body mass in pregnant women increases significantly during a relatively short period of time, by an average of 11 to 16 kg [24 to 35 pounds]. In the presented sample of participants, the mass gain was about 11 kg. As for the longitudinal changes during gait, the results showed a tendency of longitudinal foot arch flattening for both feet (increasing values of DAI); however, the observed changes were statistically significant (P = 0.01) only for the right foot when comparing P2 and P3 (see figure).
Not only mass gain but also body mass distribution can be linked to plantar pressure changes. About half of body mass gained during pregnancy is situated in the abdominal area (anterior part of the trunk), which leads to changes in the center of gravity and greater oscillations of the COP. The compensations, which are believed to follow the center of gravity deviation, include increased lumbar lordosis, sagittal pelvic tilt, and a more posterior upper body tilt. Also, forward shift of plantar loading has been reported.
One of the study’s objectives was to examine how the anthropometric characteristics may influence the foot loading pattern depending on the phase of pregnancy. In particular, they found that while foot arch flattening correlated with the body mass in all trimesters (as mentioned above), the medial-lateral loading index correlated only in the first and second trimesters. The forefoot-rearfoot loading index was not influenced by the body mass. Waist circumference changes significantly influenced dynamic arch flattening but only in the late pregnancy (P2 and P3). In the third trimester of pregnancy, a small though significant increase in the right foot angle was also observed (Figure 2B). Their findings also revealed a slight ‘asymmetrical’ adaptation of foot placement characteristics in the sample of right-leg dominant women (greater DAI in P3 for the right foot, Figure 2A, and greater right foot angles, Figure 2B). While these changes were relatively small, they might be functional constituting body adaptation to remain stable besides pregnancy-related anthropometric changes. Functional asymmetry has been defined as a consistent task discrepancy between the 2 lower limbs. Within the concept of the limb dominance, the non-dominant lower limb contributes more to support, while the dominant lower limb contributes more to forward propulsion. For instance, other examples are known of subtle but functional asymmetries during stepping, or when gait asymmetries, not evident during normal walking, appear during more challenging walking tasks.
Mass and Gravity: Mass gain and the ventrally driven center of gravity induce gait disturbances in a pregnant woman. Adaptations throughout pregnancy are recognized to provide safety and stability. The most important features identified by the authors are as follows: reduced walking velocity as a result of lower frequency and smaller length of the steps, longer stance time, and increased stance width compensated by the mediolateral component of ground reaction force. Additionally, considering the lower limbs adjustments, the most affected by the continuous overloads in the course of pregnancy occurred to be a hip joint, as being closer to the body region with greater anatomical and morphological changes. As mentioned, to improve gait stability, pregnant women walk with a wider support base, which is especially visible in the third trimester. The base of support can be wider due to both increased distance between the ankles and as a result of a greater foot angle. In a prior longitudinal study, these authors found that the angle of the foot tends to increase with the advancement of pregnancy, though changes in the foot angle were significant only for the right foot.

Their findings showed that individual anthropometric characteristics affect plantar pressure distribution in pregnant women. However, they also revealed modifications or adaptations that depend on the period of pregnancy, eg, significant correlations of MLI—the ratio of medial and lateral foot loading—in the first and second trimesters but not in late pregnancy. Plantar pressure distribution changes may play a role in improving gait stability in the stance phase. For instance, Mei et al suggest that flattening of the medial longitudinal arch can result in a decreased stability during pregnancy; therefore, the observed increase in the foot angle on the same side as medial arch collapse may constitute the adaptation to keep gait stability despite medial arch collapse. This might be especially important since P3 is the time of pregnancy when the incidence of falls resulting in hospitalization is the largest and concerns almost 80% of pregnant women.
Compression & Edema
Saliba-Junior et al5 observed that pregnancy is a leading cause of varicose veins, which can lead to venous insufficiency and leg edema.
In this Brazilian study published in v, they sought to evaluate the effect of compression stockings on lower limb edema in pregnant women and their perceptions of wearing them.
This was a randomized, controlled, prospective, parallel, blinded clinical trial conducted with 60 pregnant women randomly distributed into 2 groups: an intervention group (n = 30) wearing compression stockings and a control group (n = 30). Standardized ankle and calf measurements were taken of all 120 lower limbs using a tape measure. At the end of the study, a questionnaire was administered to identify perceived difficulties and advantages related to wearing compression stockings.
Their results showed that pregnant women in the intervention group had a significantly smaller increase (P < 0.05) in calf and ankle diameters compared to those in the control group. The mean differences from the beginning to the end of gestation in the diameters of the right calf, left calf, right ankle, and left ankle, respectively, were 0.30 cm, 0.30 cm, 0.15 cm, and 0.15 cm in the intervention group and 1.95 cm, 1.95 cm, 1.73 cm, and 1.87 cm in the control group. Most of the pregnant women had no difficulty wearing the compression stockings and all reported that they felt a difference in leg symptoms and would wear stockings again.
In their discussion, the authors wrote that the intervention group members’ perceptions of using compression stockings demonstrate the ease of use of this prophylactic and therapeutic measure. All of the pregnant women reported that they felt a difference in leg symptoms and that they would wear compression stockings again. The findings of this study are in agreement with a study about acceptance of compression stockings conducted by Allegra et al6, who found that leg symptoms and pain were reduced in pregnant women who wore compression stockings. Allegra et al also observed that improvement of symptoms was associated with regularity of wearing stockings, demonstrating the importance of wearing them continuously to improve the QOL of pregnant women. Saliba-Junior et al also noted studies that demonstrate that multiparous women are at greater risk of developing varicose veins over time, irrespective of weight gain associated with pregnancy. These changes are present in approximately 13% of primiparous women, 30% of those in their second gestation, and up to 57% of multiparous women. There is also evidence that multiparity (≥ 4 deliveries) constitutes a relevant risk factor for occurrence of venous thromboembolism during pregnancy.
In their conclusion, Saliba-Junior et al wrote that compression stockings were effective for preventing lower limb edema in pregnant women who had a positive perception of wearing them.
Editor’s Note: All 4 of the articles excerpted here are available open access and readers are encouraged to use the doi numbers in the reference list to find and read them fully.
- Waugh CM, Scott A. Case Studies in Physiology: Adaptation of load-bearing tendons during pregnancy. J Appl Physiol (1985). 2022 May 1;132(5):1280-1289. doi: 10.1152/japplphysiol.00555.2021. Use is per CC BY.
- Conder R, Zamani R, Akrami M. The biomechanics of pregnancy: a systematic review. J Funct Morphol Kinesiol. 2019;4(4):72. doi: 10.3390/jfmk4040072. Use is per CC BY.
- Branco M, Santos-Rocha R, Vieira F, Silva M-R, Aguiar L, Veloso AP. Influence of body composition on gait kinetics throughout pregnancy and postpartum period. Scientifica. 2016;12: 3921536.
doi.org/10.1155/2016/3921536 - Masłoń A, Suder A, Curyło M, Frączek B, Salamaga M, Ivanenko Y, Forczek-Karkosz W. Influence of pregnancy related anthropometric changes on plantar pressure distribution during gait-A follow-up study. PLoS One. 2022 Mar 11;17(3):e0264939. doi: 10.1371/journal.pone.0264939. Use is per CC BY.
- Saliba-Júnior OA, Rollo HA, Saliba O, Sobreira ML. Positive perception and efficacy of compression stockings for prevention of lower limb edema in pregnant women. J Vasc Bras. 2022 Jan 31;21:e20210101. doi: 10.1590/1677-5449.210101. Use is per CC BY.
- Allegra C, Antignani PL, Will K, Allaert F. Acceptance, compliance and effects of compression stockings on venous functional symptoms and quality of life of Italian pregnant women. Int Angiol. 2014;33(4):357-64. PMid:25056167.





