
 By Lilly Khavari, DPM, DABPM, FACPM
By Lilly Khavari, DPM, DABPM, FACPM
Neuropathy can challenge both patients and clinicians; epidermal nerve fiber density testing provides an objective measure of disease progression and can help show therapeutic progress.
Peripheral neuropathy is something we see plenty of in our everyday practice settings and it can be very challenging to treat. We all know that the sooner we can get to an objective diagnosis, the sooner we can treat the patient, and the earlier we can start that treatment, the better it will be for the patient.
Topics we’ll cover here include what is small fiber neuropathy, how to perform epidermal nerve fiber density (ENFD) tests, and the advantages of doing it – plus I’ll add some pearls for actually performing the biopsy, and lastly, how to treat small fiber neuropathy.
Small Fiber Neuropathy

Figure 1
As all we know, there’s small fiber and large fiber neuropathy. Large fiber neuropathy is when the fibers from the neck or the back are degenerated and cause some neuropathy type issues. Small fiber neuropathy is more about sensory information, so pain, temperature, and strange or unusual sensations. We see that a lot in the feet, starting in the toes, where patients are complaining about pain or a burning sensation. What’s being affected is the myelinated, which are our delta fibers as well as unmyelinated C fibers. This form of neuropathy often involves peripheral nerves in a length-dependent pattern, meaning that the earliest and most severely affected nerves are located most distally – in that stocking/glove distribution.
What type of symptoms are we looking for? Most common are the “positive” sensory symptoms—what the patients are feeling, like pain, burning, prickling, shooting pain. The negative symptoms are what’s not there, numbness or coldness when their foot feels dry and tight. And of course, anhidrosis as well as hyperhidrosis–those are the autonomic sensory symptoms.
We always want to check for these when we’re getting the patient’s history: Do they have positive sensory symptoms or is it more negative symptoms? Or are we purely autonomic, which would lead you more into a large fiber neuropathy? If it’s only presented as an autonomic symptom, then you’re looking at large fiber neuropathy.
Common causes of small fiber neuropathy are listed in Figure 1. It’s not always frank diabetes. There are a lot of other reasons that a patient could have this type of neuropathy. For example, patients who are prediabetic with altered glucose could have this, and about 67% of the US population is prediabetic – so really anybody could have neuropathy-type symptoms.
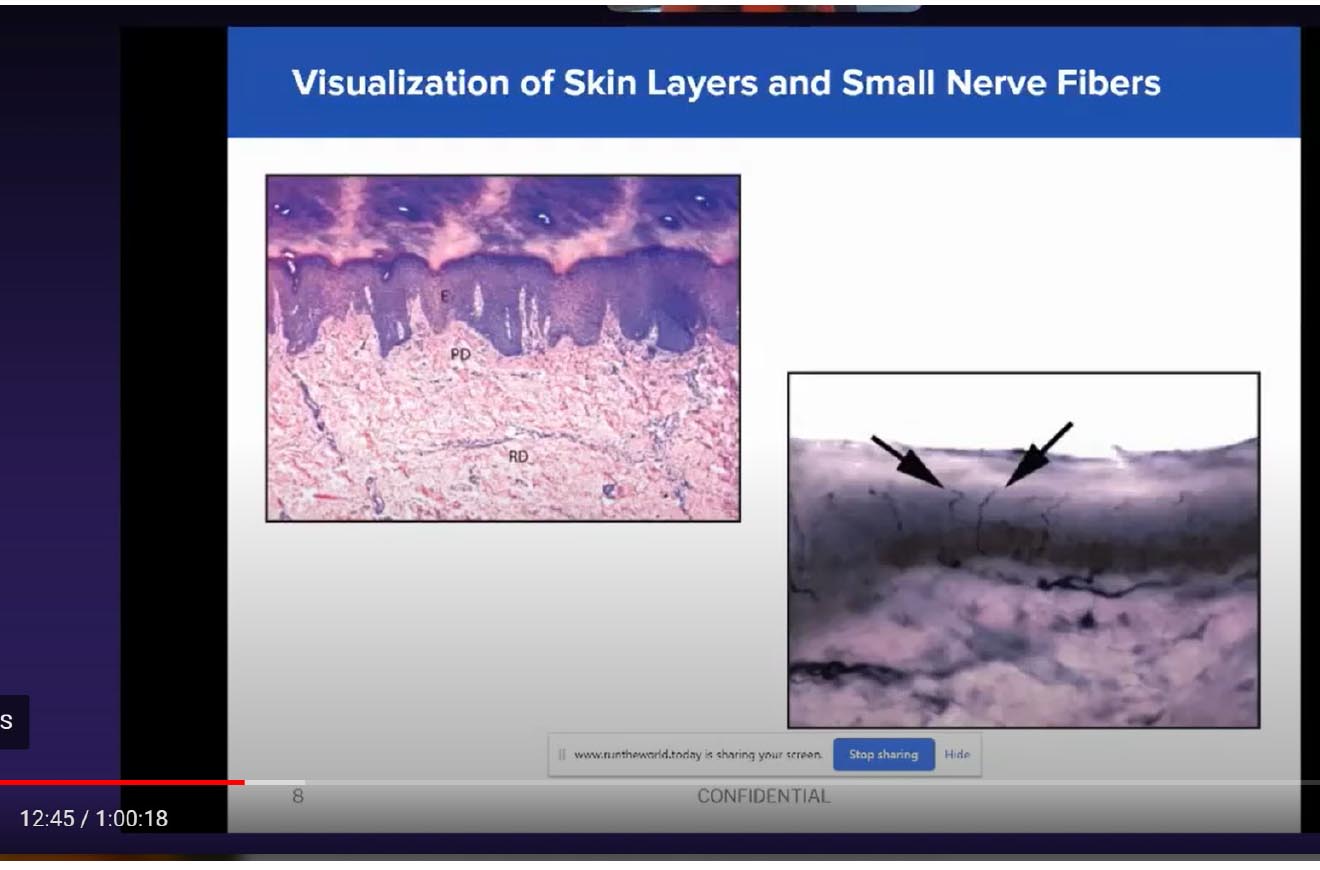
Figure 2
I see a lot of chemotherapy-induced neuropathy in my practice coming from a big oncology center across the street. It is amazing how much these chemo patients start to experience – not only are they losing their toenails and fingernails, but they’re also getting pretty severe neuropathy type symptoms. And there are patients 20-years’ post-chemo who are still having symptoms that have never been addressed. Doing a test like ENFD on these patients can help prevent progressively worsening nerve degeneration. Because chemo is typically a temporary thing for them, if we address them in a timely manner, we are able to reverse their symptoms and make it much more tolerable for them. You’re doing these patients a huge favor and they will appreciate you for diagnosing them early and giving them a way to do their daily walks and live their life without that burning pain, or numbness in their feet.
Epidermal Nerve Fiber Density Testing
Epidermal nerve fiber density testing has been widely used since the 1990s. It qualifies and quantifies small fiber neuropathy by looking at the number of healthy nerves that a patient has. It provides a definitive diagnosis of small fiber peripheral neuropathy that’s objective. Doing a Semmes Weinstein test or taking a clinical history is not enough to diagnose the degree of severity of a patient’s neuropathy. You can’t tell if they have mild, moderate, borderline, or severe neuropathy by just doing a vibratory test or by doing a monofilament test. Having these test results available helps you determine the degree of severity so if you want to go back 6 months or a year later and redo the test, you have something objective to compare it to, whereas you can’t base your follow-ups on a Semmes Weinstein.

Figure 3
The ENFD test is highly sensitive and very specific for small fiber neuropathy. As far as sensitivity of this skin, it is about 88% versus just 54% for clinical examination. And it’s highly specific–about 95% to 97% specific. So, with this test, not only are you diagnosing them properly, but you know that’s the only diagnosis and you’re able to determine the course and what degree of disease is present.
Figure 2 is a diagram of what the test looks at. On top left, you can see the layers of skin: the dark purple layer on top is the epidermal layer, which is the layer that we are testing to look for those nerves, followed by the papillary dermis, immediately below. And lastly, on the bottom is our reticular dermis. So we’re not really getting that far into the dermis when we’re doing the test. We’re mostly looking at that epidermal layer to check those nerve endings.
On the bottom right, these arrows point to healthy nerve endings. And as you can see, this is a healthy nerve. We don’t have any kind of swelling; the nerve is nice and thin and it’s very fine – exactly what we’re looking for.
We’re looking for about 10 of these nerves in about a millimeter of biopsy. The more the patient has, the healthier the nerves are. The less the pathologist sees on the test, however, the more severe the patient’s disease. If there is swelling, that would mean degeneration of the nerves, so even if the number of nerves is good, if they are swollen or very thinned out, these are degenerated nerves. Not only are we looking at the number of nerves present, but also the health of the nerves and what condition they’re in to determine what type of disease and what degree of disease the patient has.
Advantages
Advantages of performing this test include:
- It’s a confirmatory diagnostic tool
- It can be both prospective and predictive
- It can serve as a baseline against which to measure therapy.
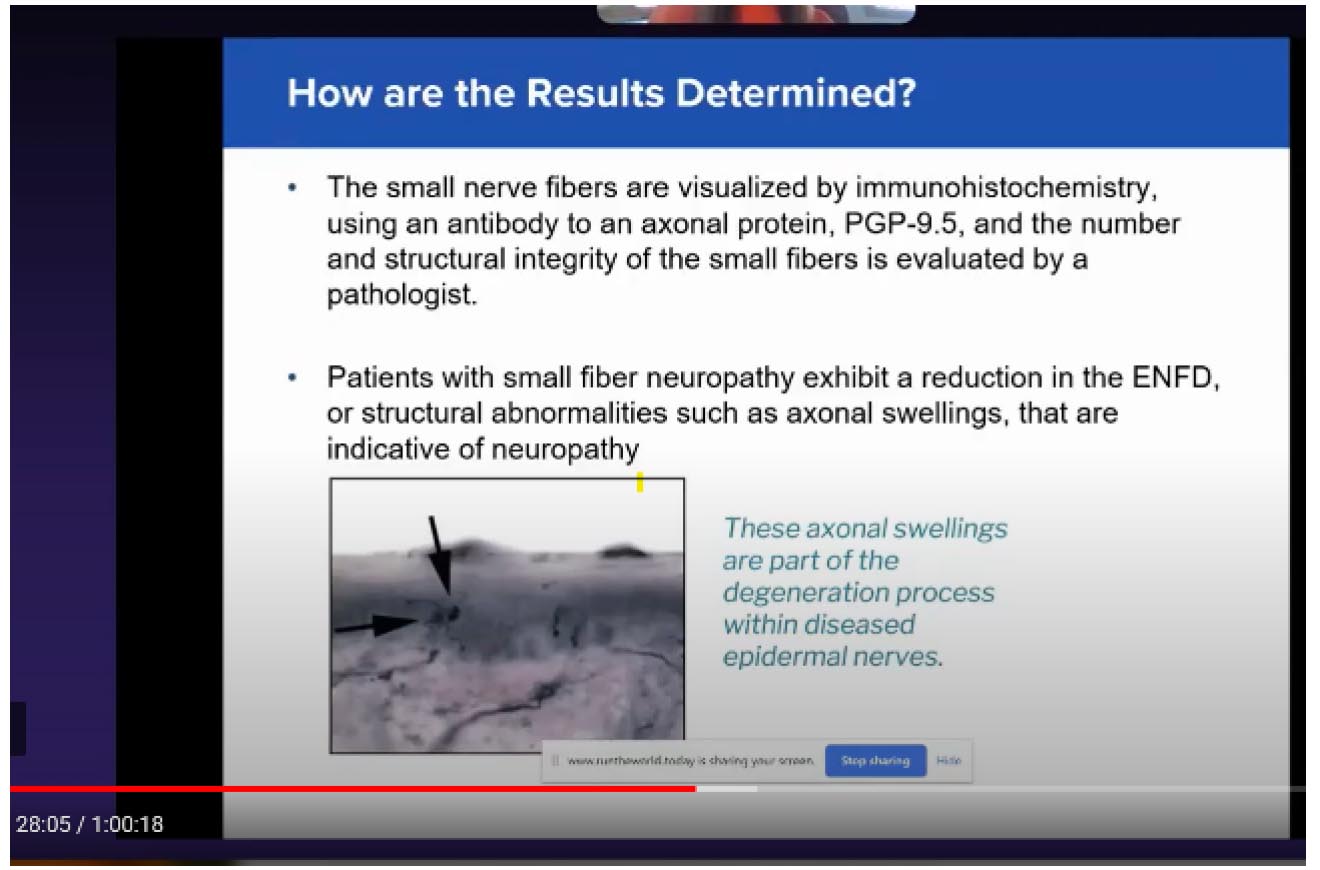
Figure 4
If it’s performed right. You’re going to have great results every time.
You can follow up with patients in 6 months to a year. They don’t always need a rekit test because you go with how they’re feeling, how their symptoms are doing. But if you see that you’re not having the improvement that you want, you can always go back and redo the test in a 6-month period to see if your treatment is changing the number of nerve endings that are showing up on the path report.
The ENFD test is a great tool to be able to compare over time and use it to discuss progress with patients—especially when symptoms aren’t decreasing as quickly as they would like. This test allows you to show that the treatment plan is working.
It’s an in-office procedure that takes less than 5 minutes to do per site, given that you have a protocol, and everything is ready to go. It’s not a big production, you don’t need an hour to just do a biopsy. If patients are in and out for their regular appointment, you can have a protocol that allows you to do these as part of a patient’s established appointment and have your results within 2 weeks and then you can start their treatment. It’s a very easy test for the physician to perform and patients have no downtime. They can immediately return to work. They can go back to their physical activity. They don’t have any pain or limitation. They have a small dressing–a Band-Aid on the biopsy site–that’s another great thing that patients love–there’s no downtime.

This test is covered by Medicare (Avg $90-100 per site) and private insurance using your average skin biopsy CPT code. We use 11104 for the first biopsy site, and if you’re doing bilateral testing, which I always advise, then for the second site, use 11105. Of course, you want to have proper documentation in the patient’s chart. Those materials are necessary to be able to get this covered in case the carriers request any kind of a documentation. Having a consent and proper diagnosis and showing that you explained why we’re doing this test should be adequate to get the test covered by insurance.
How to Do the Biopsy
The best site for biopsy – by far the most studied anatomic location – is 10 centimeters proximal to the lateral malleolus, that spot has the most nerve endings (Figure 3).
Symmetrical testing is advised. I always do symmetrical testing because most people have symmetrical symptoms. But even if they only have unilateral symptoms, It’s good to have the other side for comparison, to be able to see what their “normal” is and what we’re trying to achieve.

Figure 5
I always advise having your NFT kits from your lab ready to use. Your medical assistant has already opened it, laid everything out, and all you’re doing is going in, numbing them up, and performing the biopsy. You’ll want to familiarize yourself with the type of fixative that your lab uses. Some require you to send it after washing the sample. Some don’t have that requirement, so you want to familiarize yourself so that once you have done the biopsy, your specimen is staying viable and getting to the lab in a timely manner–most labs want the samples overnighted. They don’t want it to be in the fixative, but sometimes when you do that wash process it does allow your specimen to survive for a while longer, so you definitely want to familiarize yourself with what your lab requires.
I like to excise with 1% lidocaine and epinephrine just to control bleeding. This is proximal enough where you’re not worrying about vasoconstriction or causing any kind of an issue with that site. Doing this controls the bleeding, especially after the procedure when they get up and drive away.
Also, you want to be gentle with this specimen. Remember, all of those nerve endings are in that superficial epidermal layer. So when you’re using the pickups, it’s important not to press that epidermal layer so you don’t crush those nerve endings. So you always want to pick up the specimen from below the epidermal layer. (There is a video of the procedure within the talk on lerEXPO.com)
There are different kinds of punches available, 2 or 3 millimeters works fine. I found that using one with a plunger really helps. It’s not absolutely necessary, but it does help when that specimen gets stuck in the punch. You’re not trying to pull it out and crushing the specimen. Having that plunger helps better preserve the specimen. So remember to handle the tissue at the subcutaneous level to avoid pressing the epidermis with your pickups which will crush the epidermal layers and cause false lab results.
I do like doing these procedures first thing in the morning because we like to get them out before noon so that it gets there overnight and our specimen is viable.
Results and Treatments
The small nerve fibers are visualized by immunohistochemistry using an antibody to an external protein called PGP 9.5. This picks up the structure of the nerves and allows us to see the degree of disease severity. Patients with small fiber neuropathy show a reduction in the number of nerves or structural abnormalities, such as external swellings, that are indicative of neuropathy. In Figure 4, you can a degenerated nerve. Compared to Figure 2, where you saw healthy nerves that were very linear and the same width across the whole nerve, here you can see swollen nerve endings and axonal swellings in that epidermal layer, which show degeneration and can cause symptoms.
Contrary to what many believe, we have lots of treatment options available Figure 5. First and foremost, if a patient is pre diabetic or already has diabetes, we want to incorporate blood sugar level management, diet, and lifestyle modifications, so getting them exercising, having a healthy diet. Plus, there are certain vitamins that are important for health of the nerve: alpha lipoic acid, benfotiamine, and vitamins B6, and B12. The next level of treatment is topical creams or compounded creams/medications, and lidocaine patches. Those are, of course, always an option for daily pain management. The next level is opioid management, ideally on a temporary basis as it can lead to dependence. And then finally, MLS laser therapy combined with nutritional management. As a last resort, nerve stimulators where you’re referring patients out to a pain specialist. Once you get the patient’s results, you can see how much you need to do based on the severity of their disease and the results.
Figure 6
One question I often get is, who do you choose to test? I reserve this for patients who are newly diagnosed with diabetes and are starting to have symptoms. Or patients like we talked about, post-chemo patients or patients that come in and they have no idea what’s happening – those patients where you can’t find a reason like idiopathic, HIV, or alcohol abuse. These are the patients you want to test. You don’t want to do it on a patient with diabetes whose had neuropathy for over 20 years, because you’re not going to be able to reverse any of those nerves or make them healthier. But, if it’s a patient with newly diagnosed diabetes who’s starting to have symptoms and anybody with new onset of neuropathy is a fantastic candidate for this. That way you can prevent disease progression and limit their symptoms so that they’re more comfortable living a daily life and don’t have the risk of things worsening to where they’ll need opioid management That’s really the goal: You want to prevent the nerves from progressively getting worse.
First line of treatment for me at the office (Figure 6), when it’s a mild to moderate small fiber neuropathy, is to start with vitamins as discussed earlier: alpha lipoic acid, benfotiamine, vitamins B6 and B12. Make sure that they’re not already taking B12; if they are, you need to tell them not to take any more. And the reason is B12’s toxicity. If they’re taking too much B12, it can actually worsen neuropathy symptoms. The supplement that I have at the office suggests 1 tablet twice daily for optimal nerve health. There are many supplements out there that can be office dispensed, so just make sure you’re looking at the dosage as well as all the ingredients. I found that the alpha lipoic acid and benfotiamine make a huge difference. Even my patients who have been on the supplement for months and months and decide to do something over-the-counter, as long as we keep them on the alpha lipoic acid and benfotiamine, their symptoms are well managed and they’re well controlled.
Lilly Khavari, DPM, DABPM, FACPM, is a board certified, surgically trained foot & ankle specialist focusing on pediatric and diabetic foot care, sports injuries, as well as acute and chronic conditions of the foot and ankle. She owns the Carrollton (Texas) Foot Center. She is also a consultant for Bako Diagnostics.
lerEXPO.com is currently hosting “Special Considerations in Peripheral Neuropathy.” During the first session of the 3-hour CEU program, Lilly Khavari, DPM, DABPM, FACPM, from the Carrollton Foot Center in Texas gave a presentation titled, The Foundations of Peripheral Neuropathy and its Diagnosis. This edited transcript is an excerpt of that talk. To hear the entire lecture with case studies and view the video she mentions plus other speakers from the event, check out lerEXPO.com/past-events/.





