By Jay Segel, DPM; Sally Crawford, MS; and Jason Kraus, BS
Asking patients for a number to describe their pain provides the most minimal of information. These authors are calling for a comprehensive, cross-platform, multidisciplinary solution.
 A patient walks into a doctors’ office, shares their concerns, and the doctor asks, “How would you rate your pain on a scale of 1-10?” The patient replies, “Well, I could get up, so it isn’t a 10, but it hurts now and I couldn’t finish my tasks, so it’s got to be more than a 5, so I guess it’s a 7, but that is pretty arbitrary.” No joke, this really happened, and the question is what did we learn? Not much. So clearly a deeper dive and different assessment tools are needed. We believe that a comprehensive, cross-platform, multidisciplinary standardized solution is necessary to evaluate, communicate, and track pain to better understand our patients’ experiences. Are they sore? Are they stiff? Are they in overuse or underuse syndromes? Is there an alteration in the processing of their pain in the nervous system proper? A number between 1 and 10 doesn’t answer any of these pertinent questions.
A patient walks into a doctors’ office, shares their concerns, and the doctor asks, “How would you rate your pain on a scale of 1-10?” The patient replies, “Well, I could get up, so it isn’t a 10, but it hurts now and I couldn’t finish my tasks, so it’s got to be more than a 5, so I guess it’s a 7, but that is pretty arbitrary.” No joke, this really happened, and the question is what did we learn? Not much. So clearly a deeper dive and different assessment tools are needed. We believe that a comprehensive, cross-platform, multidisciplinary standardized solution is necessary to evaluate, communicate, and track pain to better understand our patients’ experiences. Are they sore? Are they stiff? Are they in overuse or underuse syndromes? Is there an alteration in the processing of their pain in the nervous system proper? A number between 1 and 10 doesn’t answer any of these pertinent questions.
We would suggest that understanding pain in a diagnostically meaningful manner relies on breaking it down into its “anatomical” components which we call the QDRIFT:
Q Quality
D Duration
R Region
I Intensity
F Frequency
T Timing
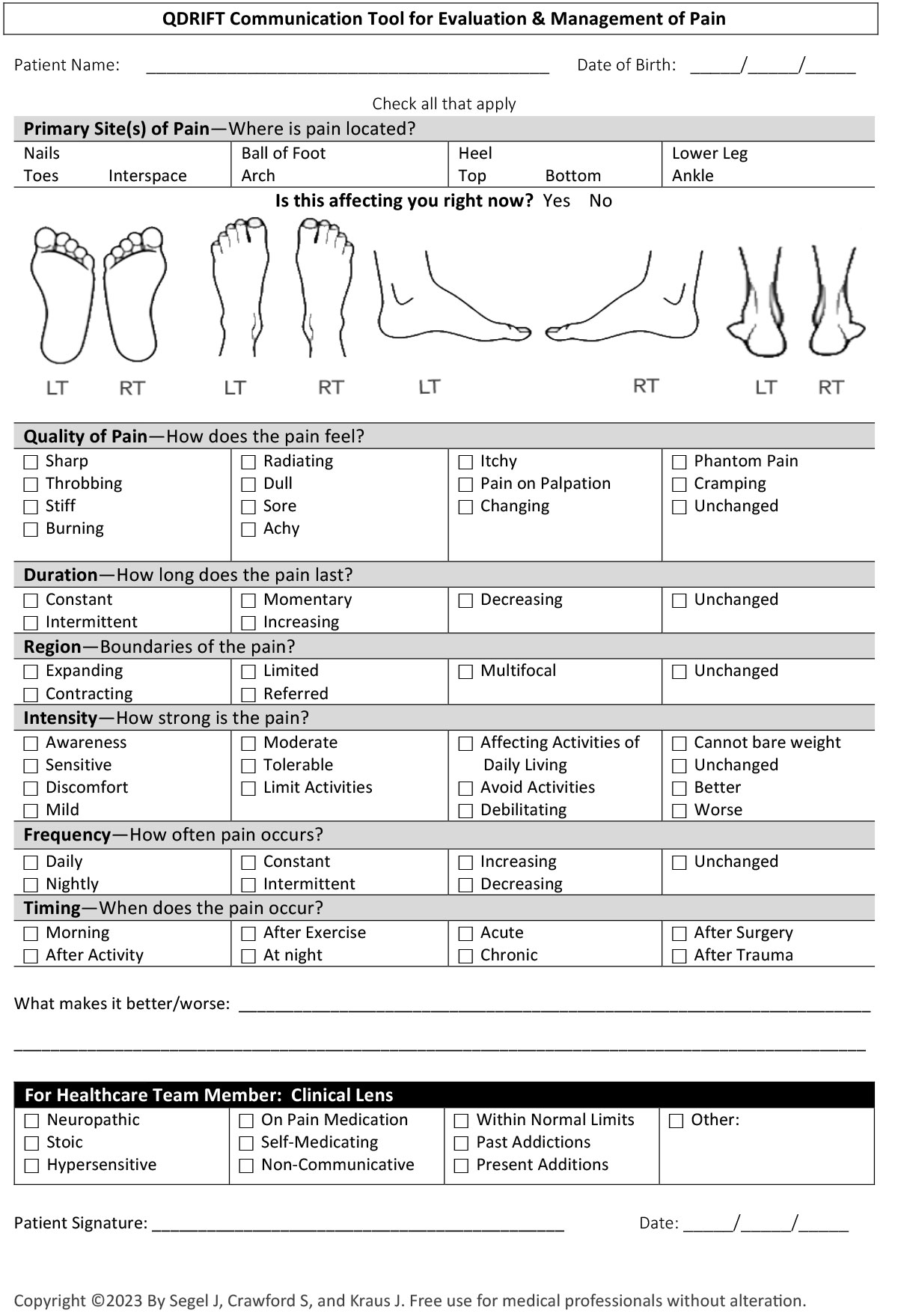
The QDRIFT Pain Evaluation and Management Tool (see page 31) begins with looking at the qualities of pain and exertion stemming from some of the more evidence-based and very standardized scales used through the ages.1-3 However, QDRIFT takes a more expanded and human approach to the experience of pain and its many details by standardizing and giving verbiage to the sensation the patient wants communicated. We use this tool with each of our patients on every visit, initially for diagnostic purposes, but then to track treatment progress.
Key components of the tool include:
Quality allows patients to describe their own pain.
Quality is an essential place to start as the type of pain is often pathognomonic of the primary affected system and diagnosis. The pain described by a person with a dry arterial ulcer is very different than the pain experience one relates who has comminuted heel fracture. Their intensity may be very similar, but the quality leads us down a different diagnostic, treatment, and assessment path. Consider how often a burning or radiating pain will lead to a neurological diagnosis such as peripheral neuropathy or Morton’s Neuroma.
Though pain crosses into other body systems, the origin of the pain likely began in one and bled into others. Take for instance the aforementioned dry arterial ulcer which certainly indicates a problem stemming from the peripheral vascular blood flow. In many cases, however, the initial sore was caused by direct trauma, such as pressure or picking at the area. That, in turn, may lead to an infective process governed by an overwhelmed or compromised immune system, perhaps winding up with a musculoskeletal consequential event such as amputation. Getting it right from the start is life changing, and maybe even lifesaving.
Duration is an important consideration when evaluating treatment plan efficacy. Comparing the duration of a pain episode as documented in the initial encounter versus the duration of said pain experience as related in the follow up can give both the practitioner and patient better clarity and insights to the efficacy of the treatment plan and suggest next steps in pain management. It is not an unusual response, when asked how they are doing, for a patient to say “I’m about the same,” which may make the treating physician rethink their approach. But when queried more specifically about frequency, intensity, and duration, patients relate, “well, the intensity is still the same, but it doesn’t come as often and it doesn’t last as long,” which gives us more to work with and helps the patient better understand that pain management is a process.

Duration tracks the length of a pain episode or its chronicity.
Region is a more recent addition to this new way of evaluating pain. It is considered an important consideration as it helps to identify an area – eg, right above the knee or just ahead of the cuboid – and consider that specific anatomy. On follow up, assessing expansion or contraction of our identified problematic region may not be possible without defining “where.” There is a relationship between regions, pain, and activities of daily living. The regions also allow us to view “pains” in the context of function, bringing in elements such as stiffness, soreness, or over- and underuse syndromes. Also to be considered is the phenomenon of referred pain, as may originate in one area but be felt in a different area within or outside the same region or system. This referred pain is often associated with “nerve pain” but is not uncommonly seen in malignancies and musculoskeletal maladies.
Lower limb arthritis may affect the entire kinetic chain. It can also be joint centric, whereas the region of pain associated with worsening tendinopathy may begin with targeted sensitivity at the origin or insertion and quickly expand through the tendon to the myotendinous junction and beyond. The understanding of the region, given pain ratings translated by a patient, provides great insight to far more.
Intensity is often the most difficult pain attribute to quantify or pin down as it is highly variable based on individual tolerance, timing, and circumstance. Rather than using numbers, other than 0 being equivalent to a finding of “no pain,” verbiage is likely a better choice. Pain perhaps begins with awareness. A lack of awareness in an anatomically defined area relative to an adjacent area would equate to our old scale 0 and a general awareness would be a 1. A more specific awareness or sensitivity would translate as a 2 and a 3 would be discomfort. Patients will often use the range of 3-5 to describe a pain between mild and moderate, while 6-7 often indicates the beginning of an interruption of activities of daily living. An 8-9 seems to indicate an avoidance to at least some, if not many, activities of daily living, leaving 10 as intolerable and unworkable. If we can use numbers, why break it out into words of patients experience? The answer is standardization, communication, and precision. Simply put, it is easier for patients to share their experiences of pain than it is to grade it!

Region provides a better understanding of whether pain is contained (at say just these highlighted spots) or expanding into broader anatomy (say up the calf or above the hip).
Frequency is another hallmark of pain and may be the most maddening of the pain descriptors from the patient perspective. “Doc, the pain just won’t leave me alone,” or “it’s driving me crazy, just when I think it’s gone, it comes back.” Again, a numbered scale is just not descriptive enough. As we tell our kids, “use your words,” we must ask our patients to do the same and be specific. For example, define infrequent pain: once a day, once a week, only when running, just the first few steps in the morning? We need to know these answers for both diagnosis and management. Here’s where using the QDRIFT Pain Evaluation and Management Tool at each visit truly pays off. It helps organize and track pain-related items for both the medical team and patient, a clear tool for one-stop evaluation and communication specific to what likely brought any particular patient into your office asking for help.
Timing has three components: “WHEN pain happens”, “HOW LONG has the pain been going on” and its relation to an event. These key points let us really dial in perspective. Timing triggers for pain, such as the first few steps in the morning or after lifting a heavy object, are important clues to diagnosis and the origins of said pain. It is also a necessary element used when crafting the treatment plan for pain mitigation. For example, activity pain like a 20-minute walk after a long period of inactivity may require proper stretching and muscle warming, whereas pain due to diagnoses like sprains, fractures, and overuse syndromes, requires rest.
Current Practice

Intensity of pain is highly subjective and using words, instead of numbers, to describe it allows patients more room to share their experiences. This young woman survived a boat explosion but lost the right leg to amputation and broke the left—who’s to say which is the more intense pain?
Through these valiant efforts to quantify something that is so subjective as an individuals’ pain, it is helpful to have a set of clinical filtered lenses to sharpen this picture. One of the first things we do during the history and physical exam is to look at “Constitution.” For example, is the patient oriented to person, place, time, and other such questions? How a person relates his or her experience of pain is often colored by their “pain constitution.” Consider the patient who presents with the throbbing pain of an infected toe versus the way a drug seeker or hypochondriac will represent pain. And then there are the stoics, who are usually in your office because a loved one threatened them, they are really scared, or they have a body part in their hand in need of reattachment! In such relaxed or excited states, it still stands true that the way you ask a question is not enough.
Current self-report scales include:
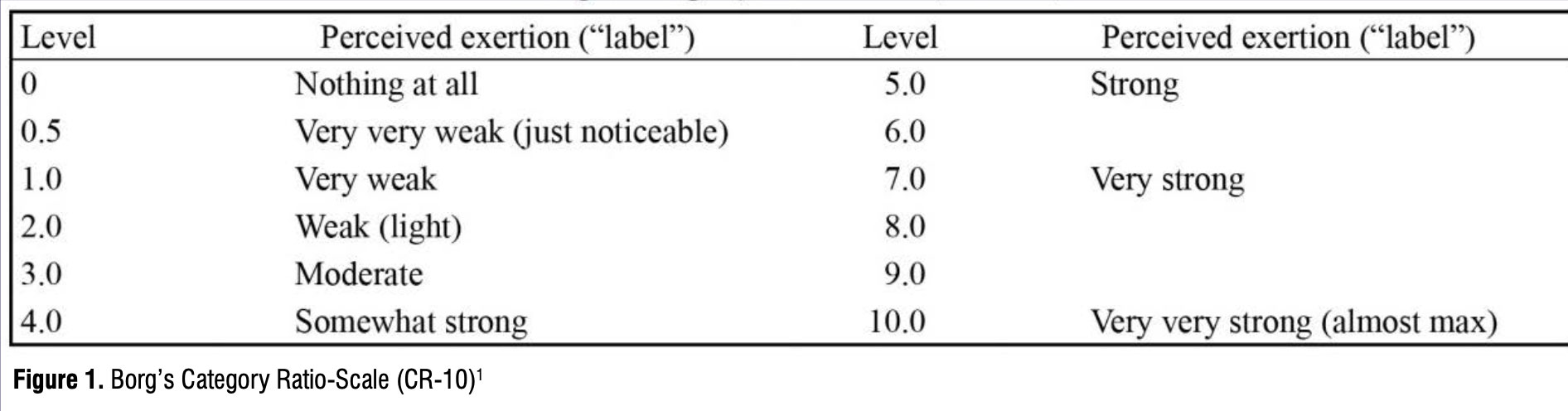
- Numerical rating scales (NRS) use numbers to rate pain (see Figure 1, but note that this is a self-report tool meant to measure the perceived intensity of pain but is not relatable or cohesive with other QDRIFT considerations). 1
- Visual analog scales (VAS) typically ask a patient to mark a place on a scale that aligns with their level of pain (see Figure 2). 4,5
- Categorical scales use words as the primary communication tool and may also incorporate numbers, colors, or relative location to communicate pain.
When used for pain, these standardized scales all provide discrete documentation but without enough context or focus on communication.6 On any scale, or from any clinical perspective, if pain is problematic, then the lack of pain can be catastrophic. Consider the patients who present with peripheral neuropathy which is often associated with loss of protective sensation (LOPS). Wounds are allowed to go undetected until perhaps the patient sees blood on their sock. By then, especially in cases with diabetes and peripheral arterial disease, tissues are undermined, infected, and covered with bioburden, and the need for surgical intervention or a limb salvage procedure may be a short time away but leave you teetering atop a very slippery slope. Catching these patients early and dosing them with effective counseling often makes the difference between loss of limb segment and more walks on the beach.
A Word About Peripheral Neuropathy
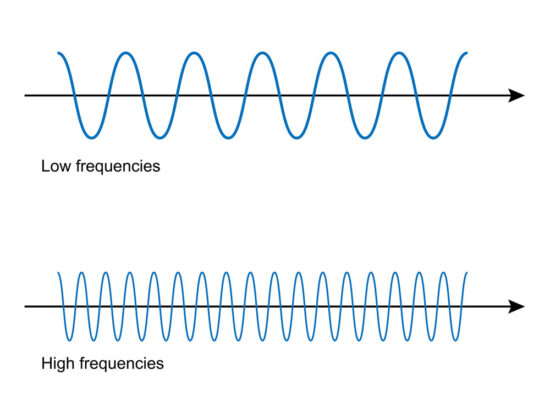
Frequency allows both patients and the medical team to track how often pain occurs.
Indeed, the world of peripheral neuropathy (PN) is a concerning and mercurial place to reside, filled with missteps and misinformation. PN often begins at our most distal regions with segmental numbness, burning and/or tingling, yet the patient’s physical exam could appear within normal limits. As the condition worsens, the symptoms become more noticeable and extend to the larger, more proximal foot regions. They also take on more curious components such as dysethesias. These are not a lack of sensation, but rather, inaccurate or “abnormal sensations” reported to the brain, such as feet feeling “ice cold” when they are warm to the touch or feeling like there is a “wad of sock” under the distal metatarsal heads as well as countless others. Phantom pain is a similar type of dysethesia, characterized by an unpleasant sensation radiating from an amputated body part.

The larger point to this pathological phenomenon is that messages from this body cannot be trusted and that regular examinations, by both patient and doctor are not just recommended, but strongly advised. One might also include imaging studies and targeted lines of inquiry like a Fall Risk Assessment. These patients often have, or progress to an abnormal and unsteady gait stemming from a lack of foot awareness and positioning referred to as proprioception. Textured orthoses and ankle-foot-orthosis bracing may be a wise choice to protect these neurologically impaired patients.
Why Use QDRIFT?

Timing addresses when pain occurs, providing relevant context.
The QDRIFT tool improves evaluation and management, allowing your patients to help you gain context and facilitate actionable and accurate care. The new data enables you to boost accountability. You enable entry into more precision care, with a more holistic approach.
The narrative your patient hears about QDRIFT will be imperative to make the tool work. Thus, using a standardized form to address each area of QDRIFT may save time and improve care. As a care provider, you are able to address progress and treatment success or failure more directly. With speedier accuracy in your care or treatment actions or recommendations, results may seem more immediate. A patient can not only feel but see their progress in their QDRIFT results over the course of the care plan. QDRIFT is a pain scale that facilitates understanding of goals and expected outcomes.
Why change the current, unstandardized, non-specific, and cookie-cutter style of recording pain, which is usually an afterthought? Because it is deficient in so many areas. QDRIFT is a more comprehensive tool that takes into account all qualifiers that allow for understanding, diagnosing, and assessing treatment and ultimately, improving patient outcomes.
Jay Segel, DPM, has been a private practice podiatrist in Martha’s Vineyard, MA, where he has seen patients for nearly 40 years.
Sally Crawford, MS, has been working in biomechanics and precision medicine fields specializing in technology and data driven models of care for 15 years.
Jason Kraus, BS, has been in the medical device industry for more than 40 years and is co-founder of Orthotica Labs, which was established in 2022.
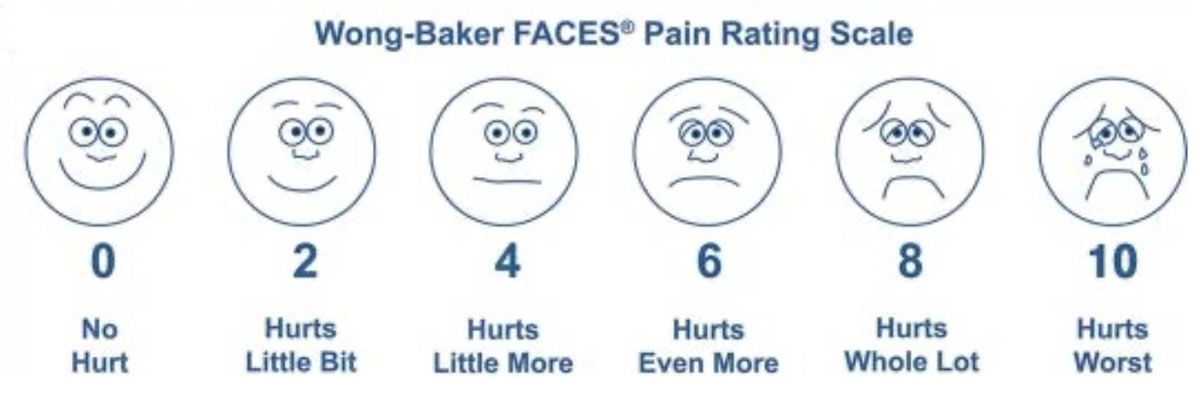
Figure 2. Example of more visual correlation to address the reflection issues of such scales.4
- Borg G. A category scale with ratio properties for intermodal and interindividual comparisons. In H.-G. Geissler & P. Petzold (Eds.), Psychophysical Judgment and the Process of Perception. VEB Deutscher Verlag der Wissenschaften; 1982: 25–34
- Borg G. Perceived exertion as an indicator of somatic stress. Scan J Rehab Med. 1970;2:92-98.
- Borg G. Borg´s Perceived Exertion and Pain Scales. Human Kinetics; 1998.
- Garra G, Singer AJ, Domingo A, Thode HC Jr. The Wong-Baker pain FACES scale measures pain, not fear. Pediatr Emerg Care. 2013;29(1):17-20.
- Karcioglu O, Topacoglu H, Dikme O, Dikme O. A systematic review of the pain scales in adults: Which to use? Am J Emerg Med. 2018;36(4):707-714.
- Hämäläinen J, Kvist T, Kankkunen P. Acute pain assessment inadequacy in the Emergency Department: Patients’ Perspective. J Patient Exp. 2022;9:23743735211049677.





