
 By Brian Burgess, DPM with Brad Abicht, DPM, FACFAS and Jeff Dikis, DPM
By Brian Burgess, DPM with Brad Abicht, DPM, FACFAS and Jeff Dikis, DPM
This article synthesizes the key findings, surgical techniques, and clinical insights from a lerEXPO’s 2025 Gait Keepers Journal Club regarding the use of intramedullary fibular nails for distal fibula fractures. The primary focus is on a retrospective multi-center study published in the Journal of Foot & Ankle Surgery (JFAS) in 2023, which represents the largest cohort of its kind to date.
The transition from traditional Open Reduction Internal Fixation (ORIF) with plates and screws toward intramedullary fibular nailing represents a significant paradigm shift in ankle fracture management. While historically reserved for “train wreck” patients–those with compromised soft tissue, diabetes, or advanced age–current clinical evidence suggests that fibular nails are highly effective for simpler fracture patterns, such as stress-positive Weber B fractures.
 Critical Takeaways:
Critical Takeaways:

- Large-Scale Validation: The 2023 study reviewed 151 patients, confirming that third-generation fibular nails provide safe and effective fixation with low complication rates.
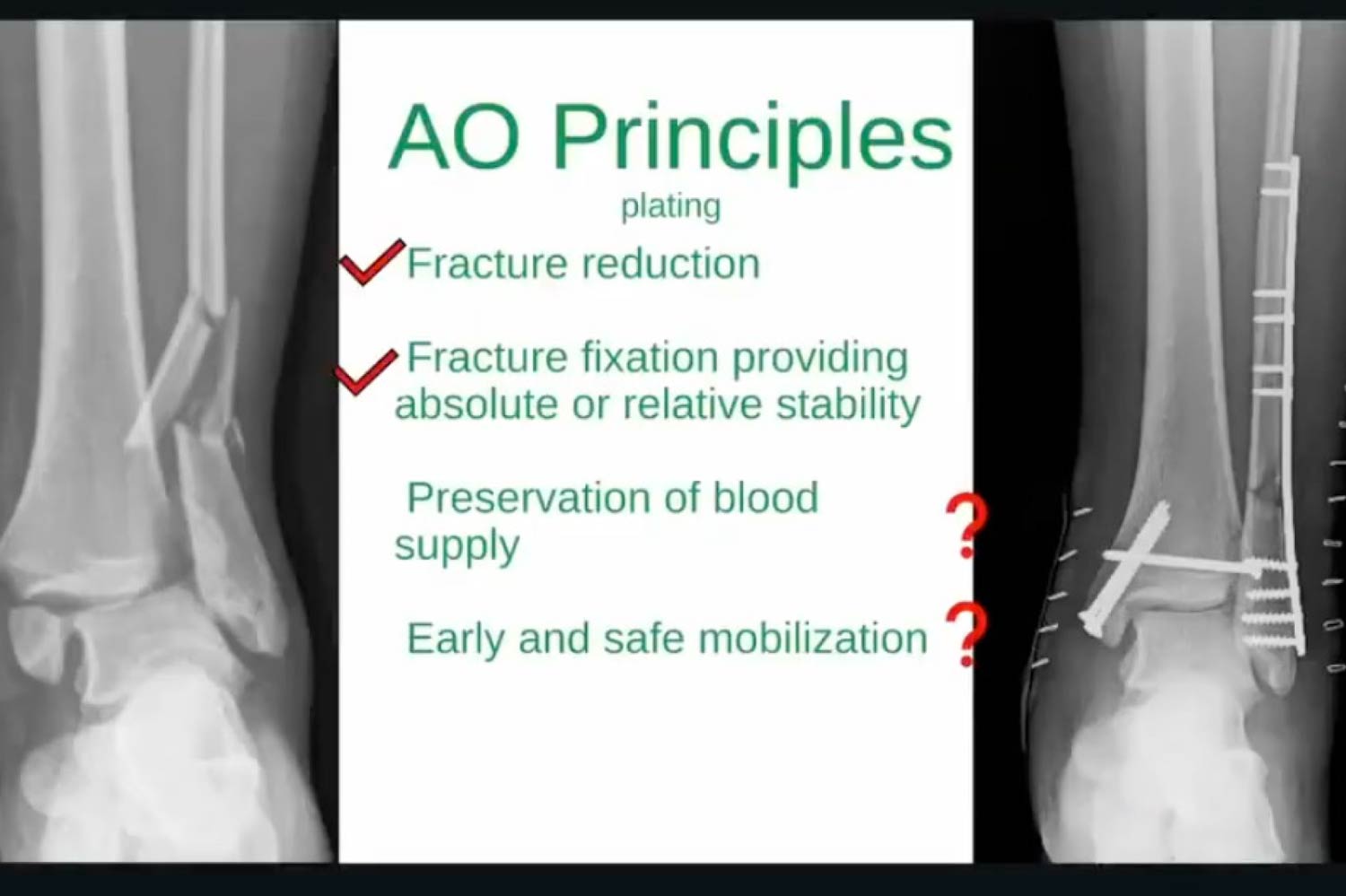
- AO Principle Alignment: Nailing better adheres to AO principles regarding the preservation of blood supply and early mobilization compared to traditional plating, which requires extensive periosteal stripping.
- Accelerated Recovery: For isolated fibular fractures, immediate postoperative weightbearing is now a viable protocol, significantly improving patient independence and reducing risks associated with immobilization.
- Reduction Philosophy: Functional reduction (restoring length and rotation) in the extra-articular fibula is clinically sufficient, as functional outcomes remain excellent even when radiographic reduction is categorized as “fair.”
Study Overview: A Retrospective Analysis
The discussion centers on a Level III evidence study published in JFAS 2023, co-authored by Dr. Brian Burgess.
- Cohort Size: 151 patients (the largest published cohort to date).
- Timeline: January 2015 to July 2021.
- Demographics: The average patient age was 52 years, ranging down to 18 years, indicating that the technique is no longer limited solely to geriatric populations.
- Primary Findings: The study demonstrated excellent union rates and a significant reduction in wound complications compared to historical ORIF data.
Evolution of Fibular Nail Technology
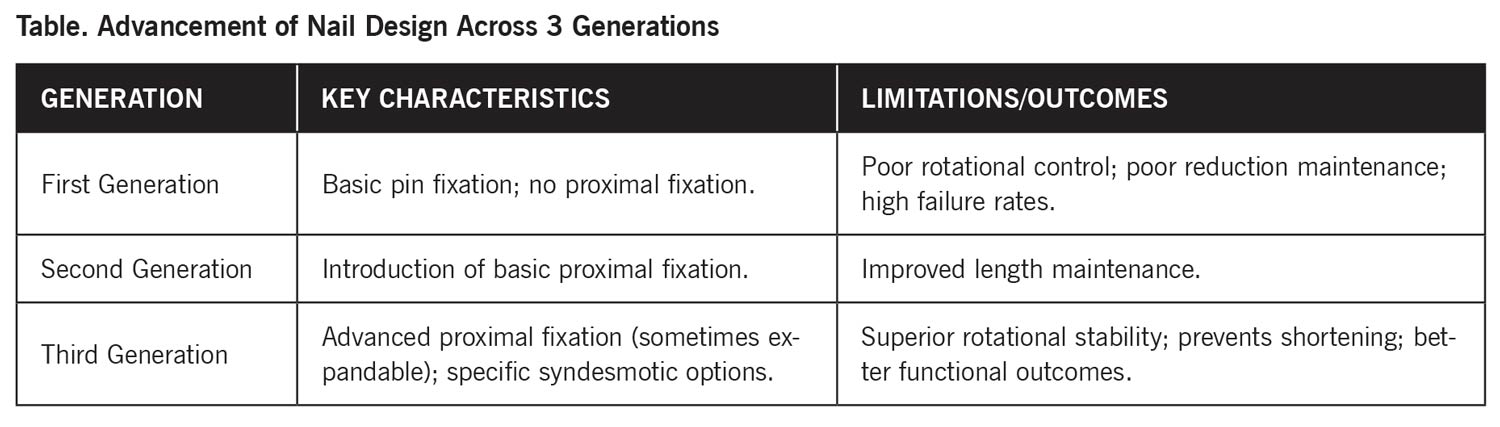
The clinical success of fibular nailing is largely attributed to the advancement of nail design across 3 generations (see Table).
Rigid vs. Flexible Nails
- Rigid/Pre-bent Nails: These nails are designed for stability but operate on the assumption of uniform anatomy. In some cases, the rigidity can “kick out” a perfect reduction during insertion.
- Flexible Nails: These can contour to the patient’s specific anatomy.
- Proximal Purchase: Newer nails often feature expandable proximal fixation to ensure purchase in the wider proximal medullary canal, particularly when using longer nail lengths (eg, 180 mm).
 Clinical Indications and Patient Selection
Clinical Indications and Patient Selection
The consensus among practitioners has evolved regarding which patients benefit most from nailing:
- Historically Indicated Patients: High-risk “train wrecks” with poor soft tissue envelopes, smokers, diabetics, and the elderly.
- Modern Primary Indications: Simple, stress-positive Weber B fibular fractures. These patients benefit from minimally invasive surgery (MIS), zero hardware prominence, and small incisions.
- Relative Contraindications: Weber C fractures can be more challenging to reduce with a nail. Highly unstable dislocations in young patients may still require traditional ORIF.
- Anatomical Constraints: Surgeons must evaluate the fibular isthmus preoperatively. Younger, petite, athletic females may have medullary canals too narrow for even a guide wire.
Surgical Technique and Reduction Strategies
A common misconception is that the nail itself achieves the reduction. Experts emphasize that the surgeon must reduce the fracture before or during nail insertion.
Percutaneous Reduction Tips
- Manual Restoration: Use thumbs to push the distal fragment anteriorly and pull it out to length by manipulating the peroneals.
- Clamping: Utilize a large, pointed reduction clamp from the medial malleolus to the distal fibula to close the medial clear space. A second percutaneous clamp can be used anterior-to-posterior (A-to-P) to close the fracture site.
- Maintaining Reduction: It is recommended to keep the reduction clamp in place while inserting the nail to prevent the hardware from displacing the fracture or causing shortening.
 Medial Malleolus and Syndesmosis
Medial Malleolus and Syndesmosis
- Fix Medial First: If a medial malleolus fracture is present, reduce and fix it first to provide an anatomical “anchor” for the rest of the ankle.
- Open the Medial Side: Even if the fibula is treated percutaneously, the medial malleolus should often be opened via a mini-incision (1–2 cm) to extract interposing periosteum or tissue that could cause a non-union.
- Syndesmotic Fixation: There is a low threshold for adding syndesmotic stabilization (eg, suture buttons). This acts as an “indirect deltoid repair” by sucking down the medial clear space.
Weightbearing and Recovery Outcomes
One of the most significant advantages of fibular nailing is the ability to accelerate weightbearing protocols.
Average Time to Weightbearing (Study Data)
- Isolated Fibular Fractures: 3.9 weeks
- Bimalleolar Fractures: 3.3 weeks
- Trimalleolar Fractures: 5.1 weeks
- Pilon Fractures: 6.8 weeks
Current Clinical Practice: For isolated fibular fractures fixed with a nail, some surgeons now permit immediate postoperative weightbearing in a CAM boot. This is rarely possible with traditional plating due to the size of the incision and the increased risk of wound dehiscence with early mobilization.
 Radiographic vs. Functional Outcomes
Radiographic vs. Functional Outcomes
The study utilized the McLennan and Ungersma guidelines to qualify reductions as “good,” “fair,” or “poor.”
- Reduction Accuracy: 97% of cases were reduced to length; 100% achieved closure of the medial clear space.
- Acceptable Displacement: Approximately 9% of cases showed “fair” reduction, often involving a 1–2 mm posterior displacement. This is frequently due to the syndesmotic screw/button passing through the fracture site.
- Clinical Relevance: There is no documented clinical difference in functional outcomes between “good” and “fair” radiographic reductions. Because the fibula is largely extra-articular, a “functional reduction” (restoring gross anatomy, length, and rotation) is sufficient for patient satisfaction and long-term success.
Notable Quotes on Clinical Philosophy
“I really think fibular nailing kind of conforms to the AO principles better than plating… Number 3 is preservation of blood supply. Number 4 is early and safe mobilization. You can’t tell me you’re putting a big plate on a patient… [and] preserving the blood supply. You’re not. You’re stripping the periosteum.”–Dr. Brian Burgess
“If I’m going to use the nail, I want to use it on an elderly patient with a very simple Weber B fracture that doesn’t require a lot of reduction and then just throw that up there minimally invasive… and then just get them walking right away.”–Dr. Jeff Dikis
“One thing that kind of annoys me is when surgeons arrogantly say, ‘I don’t need fibular nails because I don’t have wound complications.’ …If you’re doing a fair amount of these, these patients, they’re not all young and healthy… there’s just no scenario where you’re opening every single ankle fracture… and you’re not getting wound issues.”–Dr. Brian Burgess
Dr. Brian Burgess is a board-certified podiatric surgeon who specializes in foot and ankle surgery. His treatment philosophy stresses conservative management and an evidence-based approach to surgical intervention when indicated. Prior to surgery, Dr. Burgess uses a variety of conservative techniques including injections, bracing, orthotics and physical therapy. With an emphasis on minimally invasive techniques, he frequently returns his patients to an active lifestyle in a quick and safe manner.
Dr. Burgess is well-trained in all aspects of the foot and ankle and has a special interest in minimally invasive bunion correction, minimally invasive fracture repair, Achilles tendon disorders, acute and chronic ankle sprains, ankle arthroscopy, heel pain treatment, orthotic therapy, sports-related injuries and trauma/fractures of the foot and ankle.
Dr. Burgess received his podiatry degree from the Dr. William M. Scholl College of Podiatric Medicine in 2009 and his bachelor’s degree, with honors, from the University of Illinois at Urbana-Champaign. Dr. Burgess completed a 3-year podiatric surgical residency in trauma and reconstructive surgery of the foot and ankle at Mercy Hospital and Medical Center in Chicago.
In addition to his clinical practice, Dr. Burgess is actively involved with medical education. He is the Fellowship Director of Hinsdale Orthopaedics (IBJI) Foot and Ankle Fellowship. He is actively involved within The College of Foot and Ankle Surgeons where he dedicates considerable time training medical students, residents and experienced surgeons. He frequently lectures nationwide and is an invited faculty at advanced ankle arthroscopy courses and annual scientific conferences.
Bradley P. Abicht, DPM, FACFAS, is the Department Chair of Podiatric Medicine and Surgery at emplify Health by Gundersen in La Crosse, Wisconsin. He is a leader in minimally invasive (MIS) and percutaneous foot and ankle surgical procedures as well as foot and ankle reconstructive surgery, foot and ankle arthroscopy, and foot and ankle sports injuries. An educator to residents and medical students, he is frequently published in peer reviewed journals. A renown national and international speaker and founder of the annual Western WI Foot & Ankle. He also serves as the Medical Director of lerEXPO, Associate Editor of FASTRAC and hosts GaitKeepers Journal Club.
Jeffrey Dikis, DPM currently practices as a partner with McFarland Clinic, Iowa’s largest physician-owned multispecialty clinic. After residency at the University of Pittsburgh Medical Center, he worked at an orthopedic group in Tennessee before moving home to Iowa. He is certified in foot surgery and reconstructive foot and ankle surgery by the American Board of Foot and Ankle Surgery. He serves as clinical faculty with the Des Moines University College of Podiatric Medicine and Surgery. Dr. Dikis has extensive training in Arthroscopy, Trauma, Sports Medicine and Reconstructive Surgery, and has taught and lectured at national educational conferences and courses.
He is the host and creator of the popular Pod Patrol podcast, an entertainment and educational podcast, covering topics of the foot and ankle with both podiatric and orthopedic colleagues. He is one-half of the instagram tandem FootDocDuo, producing educational content. He has authored research papers in both The Foot and Foot & Ankle International.
He is married to his wife, Ashley, also a podiatric surgeon, and has 2 young boys. He enjoys music and plays the piano and drums. He is an avid Iowa Hawkeye fan and enjoys coaching his kids’ soccer and basketball teams.
This article summarizes the presentation by Dr. Brian Burgess with Dr. Abicht and Dr. Dikis titled, “Fibular Nails–Fad or New Standard?” from Gaitkeepers Journal Club February 25, 2025. To view the full presentation with audience questions and answers–and to see the complete agenda for the program–visit https://gaitkeepers.lerexpo.com/. Continuing education credits are available for this and many other lerEXPO programs.





