
 By Patrick DeHeer, DPM FACFAS, FFPM RCPS (Glasg)
By Patrick DeHeer, DPM FACFAS, FFPM RCPS (Glasg)
The Lapidus bunionectomy, named after American orthopedic surgeon Paul Lapidus, has emerged as a highly popular surgical approach to correcting severe cases of hallux valgus, the deformity commonly known as a bunion. This procedure involves fusing the first tarsometatarsal joint to realign and stabilize the metatarsal bone, aiming to correct the deformity at its root and ideally prevent recurrence. A properly performed Lapidus procedure aims not only at straightening the metatarsal bone but also addressing any associated subluxation of the sesamoids to prevent recurrence. The Lapidus has gained traction among foot and ankle surgeons due to its potential to provide a long-lasting solution.
Despite its popularity, there are numerous misunderstandings surrounding the Lapidus bunionectomy. Key among them is the belief that the procedure guarantees a permanent solution without the possibility of recurrence. However, studies and clinical outcomes have shown variability, with recurrence rates reported in some reviews as high as 25%, though others present lower rates. This procedure is not a one-size-fits-all solution and does not guarantee long-term success and surgeons need to be honest about that. Success heavily depends on individual anatomical factors and the specific triplanar deformity, the surgeon’s skill and attention to adjustments in all planes, and post-operative care adherence.
Pathophysiology of Hallux Valgus
Understanding the development of hallux valgus is crucial for addressing and preventing complications effectively.
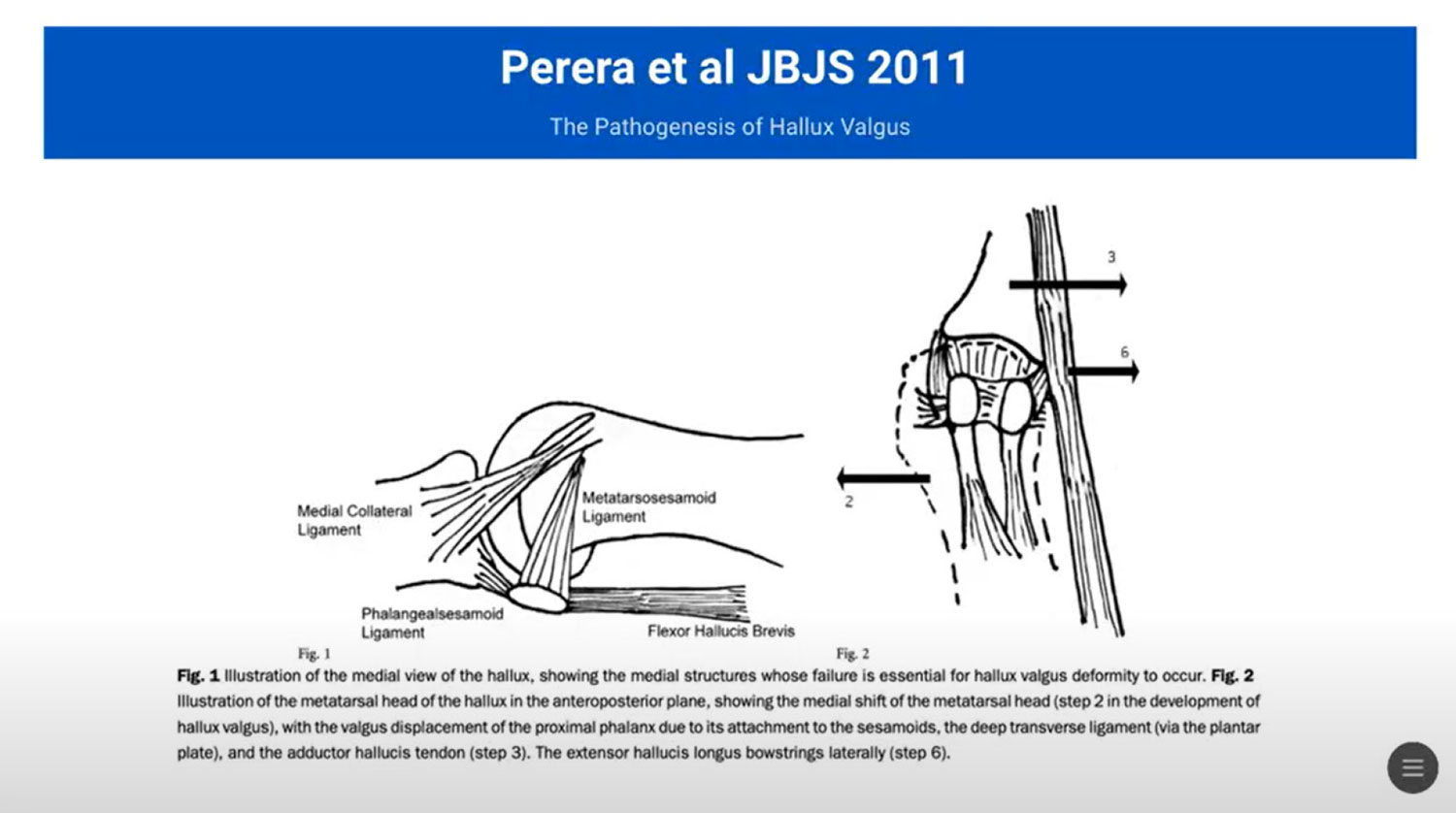
The development of hallux valgus can be described in a 10-step process initially outlined by Perera et al in 2011 (see figures on next page):
Step 1 involves the failure of the medial structures of the medial collateral ligament, the metatarsal-sesamoid ligament, the flange sesamoid ligament. The integrity of the medial collateral structures is instrumental in maintaining the alignment and function of the first metatarsophalangeal joint. Strengthening or supporting these medial structures can slow the progression of the deformity, providing a pivotal target for therapeutic intervention. Failure or weakening of these structures leads to movement at the joint level with the displacement of the metatarsal over the fixed sesamoids.
Pronation of the first metatarsal and altered sesamoid position are significant contributors to Step 2. Studies have shown that there is notable pronation in affected individuals, which disrupts the normal biomechanical alignment and increases stress on the metatarsophalangeal joint. The sesamoids, which are supposed to protect and enhance tendon efficiency under the first metatarsal, when misaligned, exacerbate the malposition of the toe.
As the condition progresses, other changes including the valgus positioning of the phalanx (Step 3), erosion of the metatarsal head (Step 4), and formation of a bursa over the first metatarsal head (Step 5) occur.
Critical, yet underappreciated is Step 6, which involves the long extensor and flexor tendons. Under normal circumstances, these tendons help maintain the sagittal plane alignment of the first ray. However, in Step 6, we see the lateral translation of the long flexor and extensor tendons, which serves to further exacerbate the biomechanical deformity.
Step 7 is the hot topic everybody is currently focused on: the pronation of the first metatarsal head.
The deformity culminates with metatarsal head rotation, causing instability and elevation, and ultimately resulting in lateral transfer pressure.
Surgical Techniques and Outcomes
 Choosing the right corrective procedure for a Lapidus Bunionectomy involves understanding the specific anatomic deformities present in each case. Surgeons must consider the severity of the bunion deformity, the intrinsic stability of the foot within the context of the patient’s lifestyle, and the presence of any co-existing conditions that might affect healing. The goal is to realign the metatarsal and phalangeal bones while restoring normal foot function, requiring a tailored approach for each patient.
Choosing the right corrective procedure for a Lapidus Bunionectomy involves understanding the specific anatomic deformities present in each case. Surgeons must consider the severity of the bunion deformity, the intrinsic stability of the foot within the context of the patient’s lifestyle, and the presence of any co-existing conditions that might affect healing. The goal is to realign the metatarsal and phalangeal bones while restoring normal foot function, requiring a tailored approach for each patient.
Triplanar Correction: Achieving triplanar correction addresses deformities in all three anatomical planes: transverse, frontal, and sagittal. This comprehensive approach ensures that the correction is functional and durable. It involves meticulous surgical planning and execution, precise bone cuts, adequate management of soft tissues, and sometimes, supplemental procedures like lateral releases or tendon balancing to support the realigned structures.
Lateral Release Techniques: Lateral release techniques are pivotal in the correction of hallux valgus during a Lapidus Bunionectomy. Complications arise when these techniques are either inadequately executed or omitted. Historically, experts noted recurrence of deformity when lateral structures weren’t adequately released. Modern approaches now often include lateral release to ensure comprehensive correction of the toe’s alignment, but this must be done judiciously to avoid destabilizing the toe and causing other complications such as reduced toe mobility.
Long-term Effects: Surgical choices in any surgery can significantly impact patient outcomes. Therefore, long-term follow-up studies emphasize the importance of selecting surgical techniques that do not only correct the deformity but also mitigate the risks of recurrence. Strategies include ensuring stable fixation, respecting the inherent biomechanics of the foot, and preventing complications such as metatarsalgia and joint stiffness. By focusing on these elements, surgeons can enhance the procedure’s success rate and improve patient satisfaction over the long run.
Complications and Their Management
Recurrence Rates: Literature on hallux valgus surgery shows a wide range of recurrence rates, from as low as less than 1% to more than 46%. This variability could stem from differences in surgical methods, definitions of recurrence, and lengths of follow-up. Recognizing these discrepancies is vital for the surgical community to address and improve the long-term outcomes of bunion surgeries.
Torsional Adjustments: The Lapidus Bunionectomy, like any surgical procedure, has potential complications that need addressing through precise surgical techniques. One significant challenge involves torsional adjustments of the first metatarsal. Experts suggest that ignoring the innate torsion from base to head of the metatarsal during a bunionectomy can lead to suboptimal outcomes, including recurrence. Managing this torsion effectively ensures the correction remains stable long-term, hence emphasizing the need for meticulous structural realignment during surgery.
 Managing Metatarsalgia: Metatarsalgia, or pain in the ball of the foot, can emerge as a troublesome postoperative complication. Its management is crucial for patient satisfaction and functional recovery. The key lies in respecting the anatomical architecture of the foot, particularly the metatarsal parabola. Surgeons must avoid excessive shortening of the metatarsals, which could shift the load distribution unfavorably, leading to increased pressure and pain under the lesser metatarsals. Post-surgery, careful monitoring and relevant adjustments in foot orthotics might be required to manage or mitigate this complication.
Managing Metatarsalgia: Metatarsalgia, or pain in the ball of the foot, can emerge as a troublesome postoperative complication. Its management is crucial for patient satisfaction and functional recovery. The key lies in respecting the anatomical architecture of the foot, particularly the metatarsal parabola. Surgeons must avoid excessive shortening of the metatarsals, which could shift the load distribution unfavorably, leading to increased pressure and pain under the lesser metatarsals. Post-surgery, careful monitoring and relevant adjustments in foot orthotics might be required to manage or mitigate this complication.

Future Perspectives on Lapidus Bunionectomy
As surgical techniques and technologies evolve, the Lapidus Bunionectomy will continue to be refined to improve outcomes and reduce complications. Future advancements may include more precise diagnostic tools like weight-bearing CT scans to assess foot biomechanics and deformities more accurately. Additionally, the development of enhanced surgical instruments and fixation devices could allow for more accurate bone cuts and stability, potentially decreasing the recurrence rate. Innovations in postoperative care and rehabilitation protocols could further enhance recovery times and long-term function of the foot. Emphasis on comprehensive preoperative planning and patient education will remain crucial in the successful management of hallux valgus deformities using the Lapidus technique.
To learn more about “Facts, Fictions, and Fallacies of the Lapidus Bunionectomy,” see Patrick DeHeer’s full lecture from the 38th Annual No-Nonsense Seminar, available at https://nononsense2024.lerexpo.com/.
Patrick DeHeer, DPM FACFAS, FFPM RCPS (Glasg) is now Medical Director at Upperline – Indiana and Podiatric Residency Director at Ascension St. Vincent Hospital in Indianapolis.





