
 By Mathias B. Forrester, BS
By Mathias B. Forrester, BS
Background: Kickboxing is a popular full-contact sport that allows both punching and kicking from a standing position. Kickboxing may be performed in sports competitions or as a form of exercise. Injuries, including to the lower extremity, may occur in relation to kickboxing. The objective of this study was to describe kickboxing-related lower extremity injuries treated at United States (US) hospital emergency departments (EDs).
Methods: Kickboxing-related lower extremity injuries during 2000-2022 were identified using the National Electronic Injury Surveillance System (NEISS), a database of consumer product-related injuries treated at a representative sample of US hospital EDs. Cases reported to the NEISS can be used to calculate national injury estimates. The distribution of kickboxing-related lower extremity injuries was determined for patient demographics, injury circumstances, and management.
Results: Of an estimated 69,832 total kickboxing-related injuries, 34,922 (50.0%) involved the lower extremity. Of these lower extremity injuries, the affected body part was 31.6% foot, 21.8% ankle, 21.2% knee, 12.6% lower leg, 11.2% toe, and 1.6% upper leg. The most common injuries were 42.0% strain or sprain, 22.9% contusion or abrasion, and 14.3% fracture. The age distribution was 3.6% 0-12 years, 16.2% 13-19 years, 35.7% 20-29 years, 24.7% 30-39 years, 12.0% 40-49 years, and 7.7% 50 years or older; 51.9% of the patients were male and 48.1% female.
Conclusion: Half of all kickboxing-related injuries involved the lower extremity. The majority of patients with lower extremity injuries were age 20-39 years and evenly divided between males and females. The most commonly reported lower extremity injuries were strain or sprain, contusion or abrasion, and fracture, and the most frequently affected parts of the lower extremity were the foot, ankle, and knee.
 Kickboxing, a full-contact sport, is a type of boxing that allows both punching and kicking from a standing position. Participants of the sport may use mouth guards, hand wraps, boxing gloves, groin guards, and shin pads; the feet may be covered in kick boots (foot pads) or left bare. Kickboxing may be practiced for competition, general exercise, or self-defense. There are a variety of styles of kickboxing which differ in rules and in which actions are allowed or prohibited.1-3 It has been reported that 6.69 million people participated in cardio kickboxing in 2017, with the number of participants increasing over time.4
Kickboxing, a full-contact sport, is a type of boxing that allows both punching and kicking from a standing position. Participants of the sport may use mouth guards, hand wraps, boxing gloves, groin guards, and shin pads; the feet may be covered in kick boots (foot pads) or left bare. Kickboxing may be practiced for competition, general exercise, or self-defense. There are a variety of styles of kickboxing which differ in rules and in which actions are allowed or prohibited.1-3 It has been reported that 6.69 million people participated in cardio kickboxing in 2017, with the number of participants increasing over time.4
Injuries may occur in relation to kickboxing during competition as well as during general exercise. All parts of the body may be injured, including the lower extremity. Commonly reported kickboxing injuries include lacerations, contusions, fractures, strains and sprains, and concussions.1-3,5-8 The intent of this study was to describe kickboxing-related lower extremity injuries reported to United States (US) hospital emergency departments (EDs).
Methods
The data source for this retrospective epidemiologic study was the National Electronic Injury Surveillance System (NEISS) website (https://www.cpsc.gov/cgibin/NEISSQuery/home.aspx). Operated by the US Consumer Product Safety Commission (CPSC), the NEISS collects data on consumer product-related injuries from the EDs of a stratified random sample of 100 hospitals from the more than 5,000 hospitals in the US. The random sample is stratified by hospital size, geographic location, and hospital type (general and pediatric hospitals). Professional NEISS coders view the medical charts at participating hospitals and, for patients with injuries that meet NEISS inclusion criteria, collect and code information such as treatment date; patient age, sex, and race; injury diagnosis and body part injured; discharge disposition; consumer product(s) involved in the injury; location where the incident occurred; and a brief narrative describing the incident.9,10 Data are publicly available and de-identified; thus, the study is exempt from institutional review board approval.
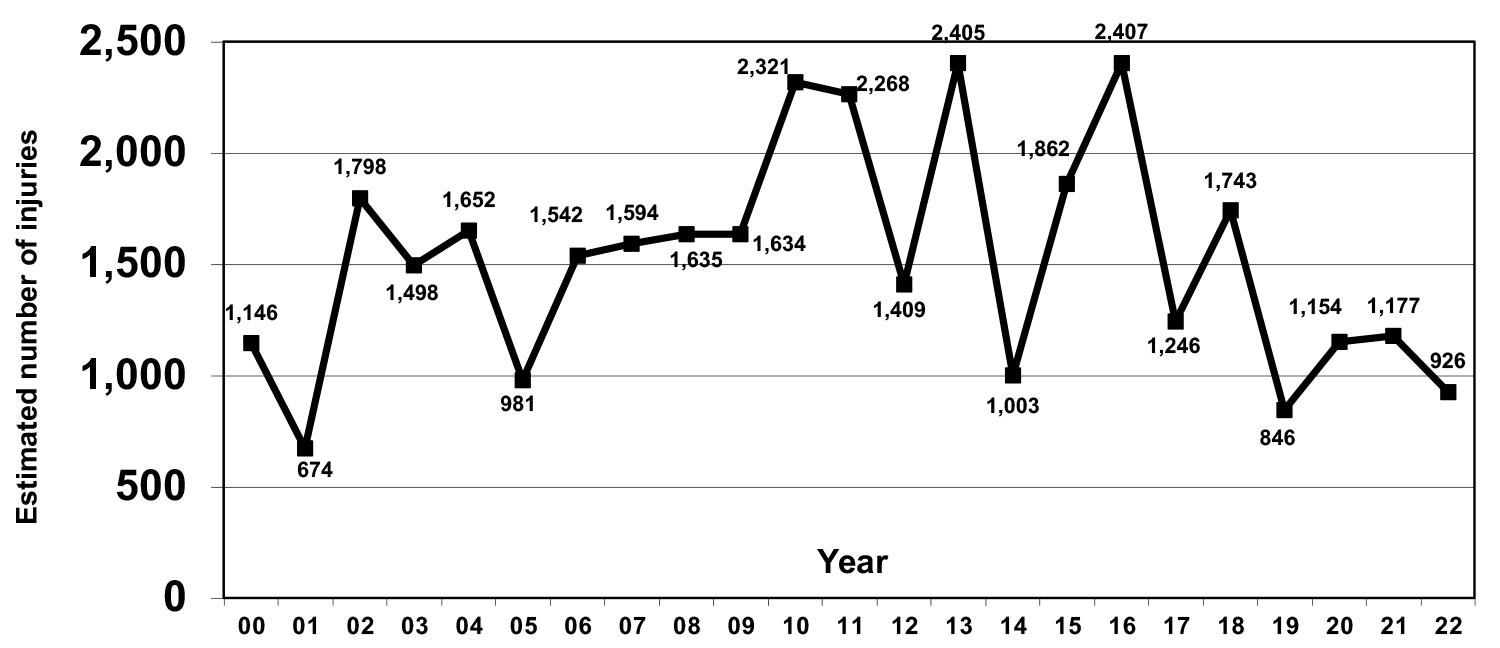
Figure 1: Annual estimated number of kickboxing-related lower extremity injuries reported to the National Electronic Injury Surveillance System, 2000-2022*
Cases were kickboxing-related lower extremity injuries reported to the NEISS database during 2000-2022. The publicly available NEISS database contains three numeric fields for coding the product involved in the injury (Product_1, Product_2, Product_3). Kickboxing may be assigned either product code 1207 [boxing (activity, apparel or equipment)] or 3257 [martial arts (activity, apparel or equipment)]. However, these product codes are not specific to kickboxing but may be used for other activities as well. The NEISS database contains a text field (field name Narrative) that provides a brief summary of the circumstances of the injury. The NEISS database was searched for all records that included the letter groups “kic” and “box” or “kik” and “box” in the Narrative field. The Narrative fields of the resulting records were individually examined, and any records that involved a kickboxing-related injury were included in the study. That the injury involved a lower extremity was based on the Body_Part numeric field (a field that documents the injured body part) containing codes for a lower extremity (upper leg, knee, lower leg, ankle, foot, toe). The NEISS database contains another numeric field for documenting whether a second body part was injured (Body_Part_2); however, this field was only added in 2018,10 although this field does not appear to have been used until 2019. For consistency over the entire study period, the Body_Part field alone was examined. (Only 5 cases had a lower extremity coded in the Body_Part_2 field but not in the Body_Part field during 2019-2022.)
 The variables examined were treatment year, month (grouped into three-month periods), and day of week; patient age, sex, and race; location where the incident occurred; type of injury (diagnosis); affected body part; and disposition.
The variables examined were treatment year, month (grouped into three-month periods), and day of week; patient age, sex, and race; location where the incident occurred; type of injury (diagnosis); affected body part; and disposition.
Analyses were performed using Microsoft 365 Access and Excel (Microsoft Corporation, Redmond, Washington, US). For all kickboxing-related lower extremity injuries, the distribution of cases and national injury estimates were determined for the variables. National injury estimates were calculated by summing the values in the Weight numeric field in the publicly available NEISS database, and 95% confidence intervals (CIs) were calculated for the estimates. The CPSC considers an estimate unstable and potentially unreliable when the number of records used is <20 or the estimate is <1,200.9 For those variable subgroups where the estimate was <1,200, 95% CIs were not calculated.
Results
During 2000-2022, 825 kickboxing-related lower extremity injuries were treated at a sample of US hospital EDs, resulting in a national estimate of 34,922 (95% CI 27,735- 42,109) kickboxing-related lower extremity injuries. This represents 50.0% of the 69,832 total kickboxing-related injuries affecting any body part. The foot was the most frequently affected part of the lower extremity, followed by the ankle and knee (Table 1). The most common types of injury were strain or sprain, contusion or abrasion, and fracture (Table 1).
The annual estimated number of lower extremity injuries varied greatly over the 23-year period (Figure 1). The mean annual estimated number of injuries was 1,292 during 2000-2005, 1,832 during 2006-2011, 1,722 during 2012-2017, and 1,169 during 2018-2022. The estimated number of injuries was 8,257 (23.6%) during December-February, 8,361 (23.9%) during March-May, 9,396 (26.9%) during June-August, and 8,908 (25.5%) during September-November. The estimated number of injuries was 22,057 (63.2%) during Tuesday-Friday and 12,864 (36.8%) during Saturday-Monday.
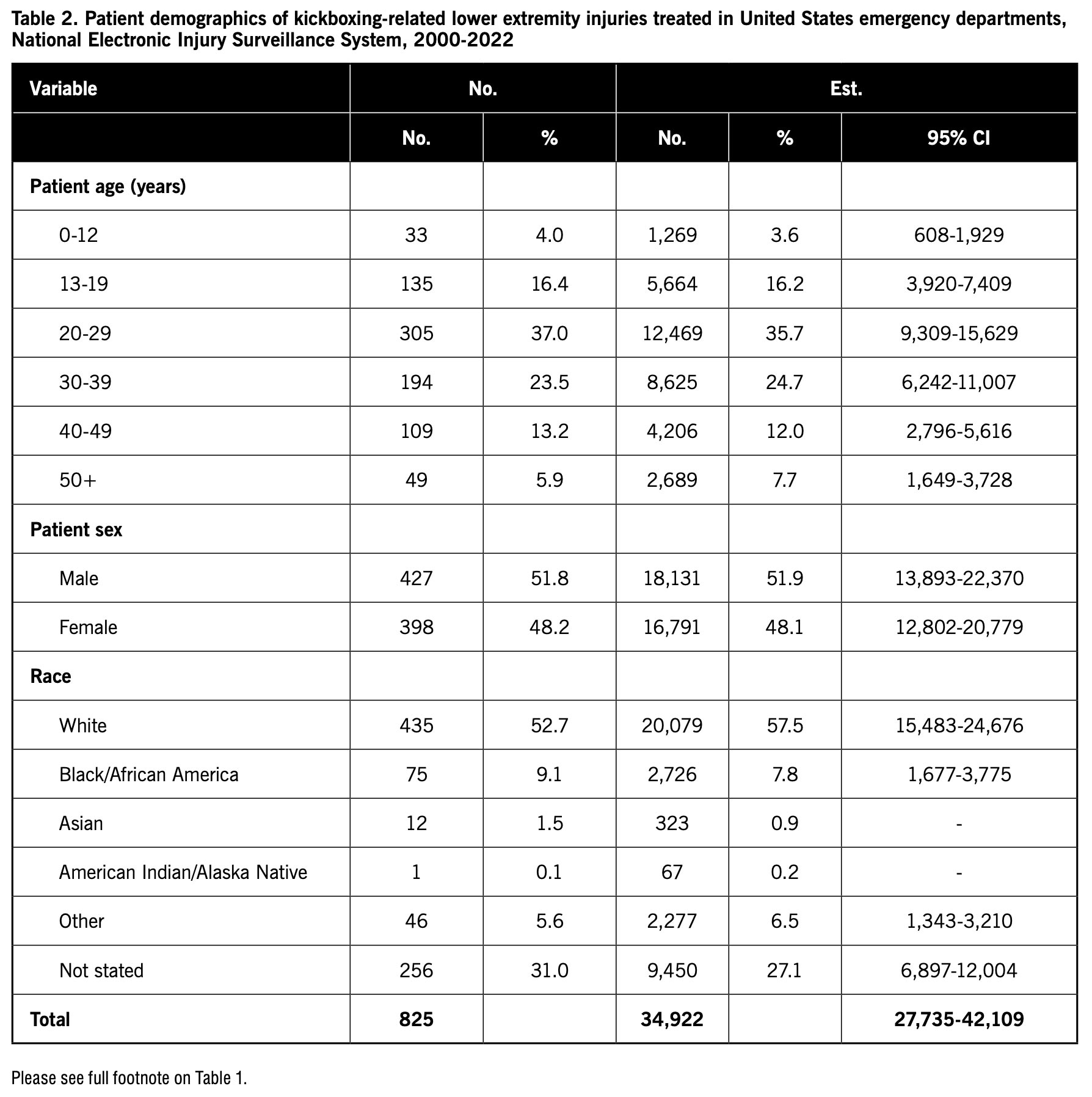
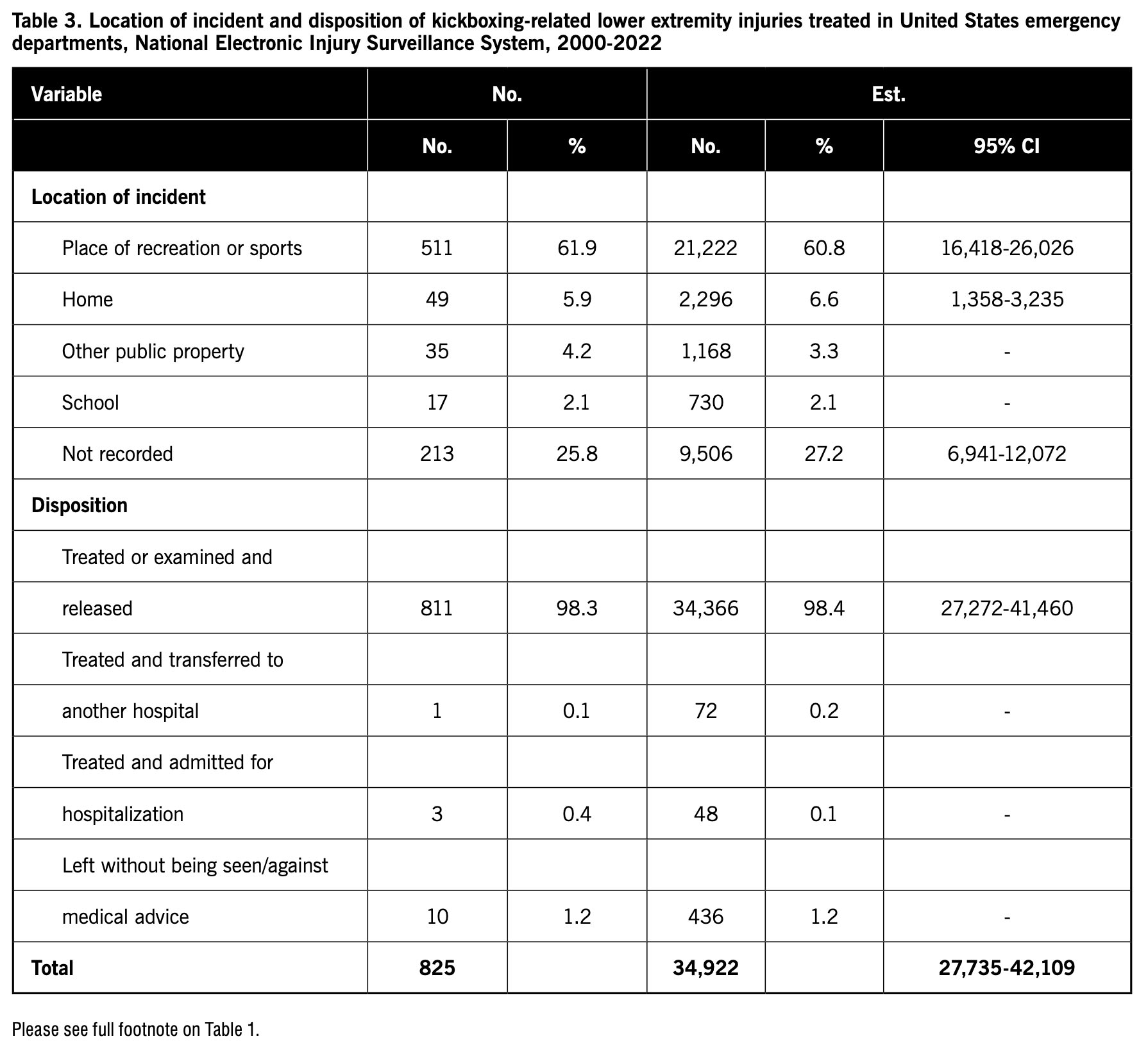 Table 2 shows the patient demographics of kickboxing-related lower extremity injuries. The highest proportion of patients were age 20-29 years followed by 30-39 years. Roughly equal proportion of patients were male and female. Most patients were White. Table 3 provides the distribution of injuries by location of the incident and patient disposition. The majority of injuries occurred at a place of recreation or sports, and most of the patients were treated or evaluated at the ED and released.
Table 2 shows the patient demographics of kickboxing-related lower extremity injuries. The highest proportion of patients were age 20-29 years followed by 30-39 years. Roughly equal proportion of patients were male and female. Most patients were White. Table 3 provides the distribution of injuries by location of the incident and patient disposition. The majority of injuries occurred at a place of recreation or sports, and most of the patients were treated or evaluated at the ED and released.
Discussion
This study characterized kickboxing-related lower extremity injuries treated at US hospital EDs. This information is important because this study found that half of all kickboxing-related injuries involved the lower extremity. Healthcare providers can use the information in this study to allocate resources to help manage these injuries. In addition, injury prevention programs can tailor the information they provide to target particular populations.
Almost one-third of the lower extremity injuries involved the foot with the next most frequently injured body parts being the ankle and knee. The most common types of injury were strain or sprain, contusion or abrasion, and fracture. These types of injuries typically are not expected to require extensive medical intervention. This is consistent with the observation that the majority of patients with kickboxing-related lower extremity injuries were treated or examined and released from the ED.
Kickboxing-related lower extremity injuries varied from year to year with no clear trend. However, the estimated number of injuries tended to be lower in the most recent years when compared to previous years. This may reflect a decline in the number of people participating in kickboxing, the number of people being injured when participating in kickboxing, the number of injured people seeking treatment at a hospital ED, or a combination of these.
 The treatment of kickboxing-related lower extremity injuries was slightly lower during Saturday-Monday than during Tuesday-Thursday. It may be that more people are taking kickboxing classes for exercise during the workweek than on weekends.
The treatment of kickboxing-related lower extremity injuries was slightly lower during Saturday-Monday than during Tuesday-Thursday. It may be that more people are taking kickboxing classes for exercise during the workweek than on weekends.

Sixty percent of the patients were 20-39 age years. This may be due to people in this age range being more likely to participate in kickboxing. The number of injuries were evenly distributed between males and females, suggesting that both sexes participate in the activity to a similar degree.
There are ways to reduce the risk of kickboxing-related injuries. Participants should warm up and stretch before kickboxing. Participants can wear proper protective equipment, which, in the case of preventing lower extremity injuries, would include shin pads and kick boots (foot pads).
There are limitations to the study. Kickboxing-related injury cases were initially identified by selecting those records with the letter groups “kic” and “box” or “kik” and “box” in the Narrative field. If these letter combinations were not used in instances of kickboxing-related injuries, then these cases would not have been included in the study. In addition, temporal changes in kickboxing may reflect changes in the documentation of kickboxing in the Narrative field over time. Furthermore, details, such as whether the injury occurred during a kickboxing competition or during kickboxing practice or exercise, were not available for many records and thus could not be examined. The study only included injuries treated at hospital EDs. Information on injuries treated elsewhere might provide a more complete perspective of kickboxing-related injuries.
In conclusion, half of all kickboxing-related injuries treated at US hospital EDs involved the lower extremity. The majority of patients with lower extremity injuries were age 20-39 years, and patients were evenly divided between males and females. The most commonly reported injuries were strain or sprain, contusion or abrasion, and fracture, and the most frequently affected parts of the lower extremity were the foot, ankle, and knee. Most of the patients were treated or evaluated at the ED and released.
Mathias B. Forrester, BS, is an independent researcher in Austin, Texas. Now retired, he previously performed public health research for various university and government programs for 38 years.
- Lystad RP. Injuries to professional and amateur kickboxing contestants: A 15-year retrospective cohort study. Orthop J Sports Med. 2015;3(11):2325967115612416.
- Gartland S, Malik MH, Lovell M. A prospective study of injuries sustained during competitive Muay Thai kickboxing. Clin J Sport Med. 2005;15(1):34-36.
- Zazryn TR, Finch CF, McCrory P. A 16 year study of injuries to professional kickboxers in the state of Victoria, Australia. Br J Sports Med. 2003;37(5):448-451.
- Amni H. Unlocking the potential of the U.S. kickboxing on the sports industry. The Ritz Herald. March 10, 2023. Available at https://ritzherald.com/hamid-amni-unlocking-the-potential-of-the-u-s-kickboxing/. Accessed May 18, 2023.
- Slimani M, Chaabene H, Miarka B, Franchini E, Chamari K, Cheour F. Kickboxing review: anthropometric, psychophysiological and activity profiles and injury epidemiology. Biol Sport. 2017;34(2):185-196.
- Buse GJ, Wood RM. Safety profile of amateur kickboxing among military and civilian competitors. Mil Med. 2006;171(5):443-447.
- Romaine LJ, Davis SE, Casebolt K, Harrison KA. Incidence of injury in kickboxing participation. J Strength Cond Res. 200317(3):580-586.
- Gartland S, Malik M, Lovell M. Injury and injury rates in Muay Thai kickboxing. Br J Sports Med. 2001;35(5):308-313.
- United States Consumer Product Safety Commission. National Electronic Injury Surveillance System (NEISS). Available at https://www.cpsc.gov/Research–Statistics/NEISS-Injury-Data/Explanation-Of-NEISS-Estimates-Obtained-Through-The-CPSC-Website. Accessed March 20, 2023.
- United States Consumer Product Safety Commission. NEISS Coding Manual. January 2021. Available at https://www.cpsc.gov/s3fs-public/January-2021-NT-CPSC-only-NEISS-Coding-Manual.pdf?xa_nMM1kB4SGpuSMOwf0NHkkkIqNcn8F. Accessed March 20, 2023.





