
 By Raquel Sugino, DPM, MS, FACFAS
By Raquel Sugino, DPM, MS, FACFAS
Navigating Minimally Invasive Foot & Ankle Surgery: Key Insights for Clinicians
Minimally Invasive Surgery (MIS) in foot and ankle continues to evolve, offering new avenues for patient care. This discussion delves into the nuances of MIS, particularly concerning bunion correction and common challenges.
Understanding the Learning Curve and Complication Rates
For those venturing into or deepening their expertise in MIS, understanding the learning curve is paramount. While historically mastering bunion correction required 60–70 cases in 2017, to 40 cases in 2022, advancements like third-generation bunion correction with 2 screws, stable fixation, and jigs have significantly reduced this learning. It is important to note that these learning curves are not directly correlated to complication. Clinicians should be reassured that taking more time or X-rays during an operation does not necessarily lead to higher complication rates.
Mastering Bunion Correction: Preventing Recurrence
Every procedure carries inherent risks. Bunion recurrence is a significant concern, with reported rates ranging from 0.9% to 1.8%. A colleague Dr. David Gordon boasts a remarkable 0.9% recurrence rate, performing thousands of bunions since 2013. Key factors influencing recurrence rates include:
- Hallux Valgus Angle (HVA): Incomplete deformity correction of the HVA and its loss at 6 months are high-risk factors for recurrence. Interoperatively, aim for a “straight as an arrow” HVA; consider an Akin or lateral release if necessary.
- Sesamoid Position: Recurrence is consistently correlated with sesamoid position across multiple studies. Loss of sesamoid reduction can lead to recurrence.
- Intermetatarsal Angle of the Proximal Fragment (IAPF): Increasing the first intermetatarsal angle of the proximal fragment by maximizing the shift helps lock up the first tarsometatarsal joint, particularly in cases of hypermobility, thereby lowering the risk of future recurrence.
Minimizing Nerve Injury
Nerve injury, though rare (0.9%), underscores the need for meticulous technique. The dorsal lateral digital nerve is particularly vulnerable, located at the 2 o’clock or 10 o’clock position depending on the foot. When performing minimally invasive lateral releases or inserting a burr for medial neck osteotomies, always know your anatomy. Pivot your hand with the wrist through the small incision (2–3mm) rather than moving your arm up and down to avoid enlarging the incision and damaging surrounding anatomy. For burr insertion, the approach should be medial, not dorsal medial, or through well padded tissue.
Optimizing DMMOs
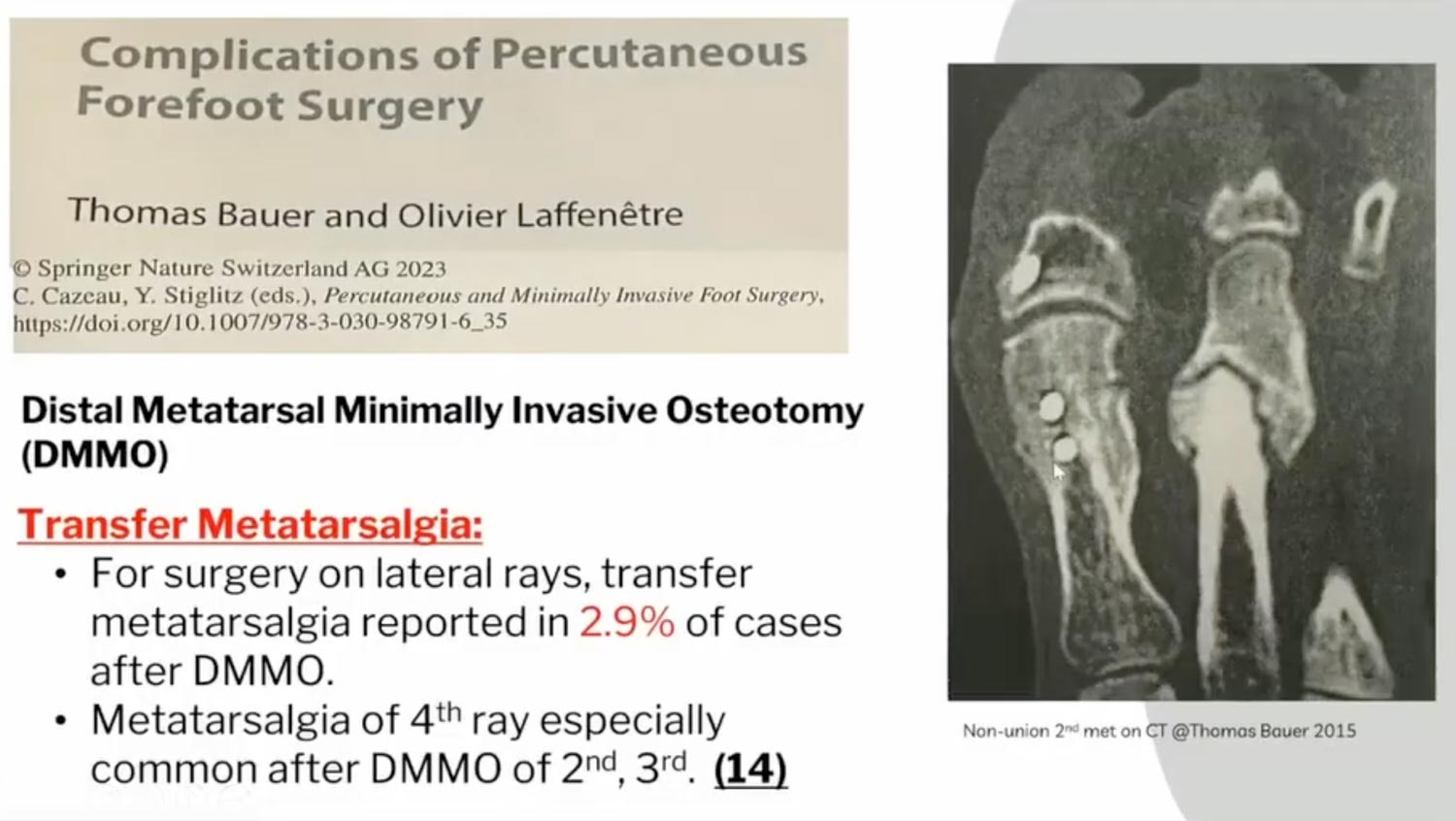
Distal Metatarsal Osteotomies (DMMOs) aim to elevate and proximally translate the metatarsal head. However, transmetatarsal transfer, where un-osteotomized lesser rays become more prominent, is a risk (2.9%). To mitigate this, consider these surgical tenets:
- Osteotomy Technique: A 45-degree cut with a 13×2 mm burr, performing a dorsal distal to proximal plantar osteotomy, and maintaining an extracapsular approach are crucial for proper healing.
- Addressing Multiple Rays: For pain under the second and third metatarsals, consider cutting the second, third, and fourth metatarsals simultaneously. The intermetatarsal ligaments connect these rays, allowing them to move better as a unit and preventing transfer metatarsalgia. This principle can also apply to offloading diabetic ulcers.
- Managing Shortening: While a 2 mm burr can cause an average shortening of 5.1 mm and a plantar translation of 2.8 mm (as the head tends to dive down) when a MICA is utilized to the first metatarsal, increasing the cut angle by 10 degrees more distally can prevent excessive shortening of the first ray.
Crucial Post-Operative Care and Preventing Complications
Post-operative management is as critical as the surgery itself.
- Dressings: For lesser metatarsal osteotomies, dressings are paramount for stabilization, unlike bunions with internal fixation. A post-operative X-ray after dressing application ensures proper toe and metatarsal alignment and also allows for any adjustments to alignment as needed for up to 3 weeks.
- Hematoma Management: Some surgeons utilize sterile strips instead of sutures for portal closures, allowing for hematoma drainage, which is generally reduced by the absence of a tourniquet.
- Float Toe: This common complication can be effectively mitigated with a P1 osteotomy. This quick hammertoe procedure involves a plantar approach, creating a small wedge at the base of the proximal phalanx (or middle phalanx), and reducing the bone to plantarflex the toe at this bone level. It avoids the need for tendon transfers or large incisions.
- Non-Union & Weightbearing: Non-union rates are low (0.4%). The importance of immediate post-operative weightbearing (Wolff’s Law). Stress on bone encourages bone formation, and delayed union often stems from insufficient weightbearing. For asymptomatic non-unions of lesser rays (rare at 0.1%), revision is not recommended before 18 months.
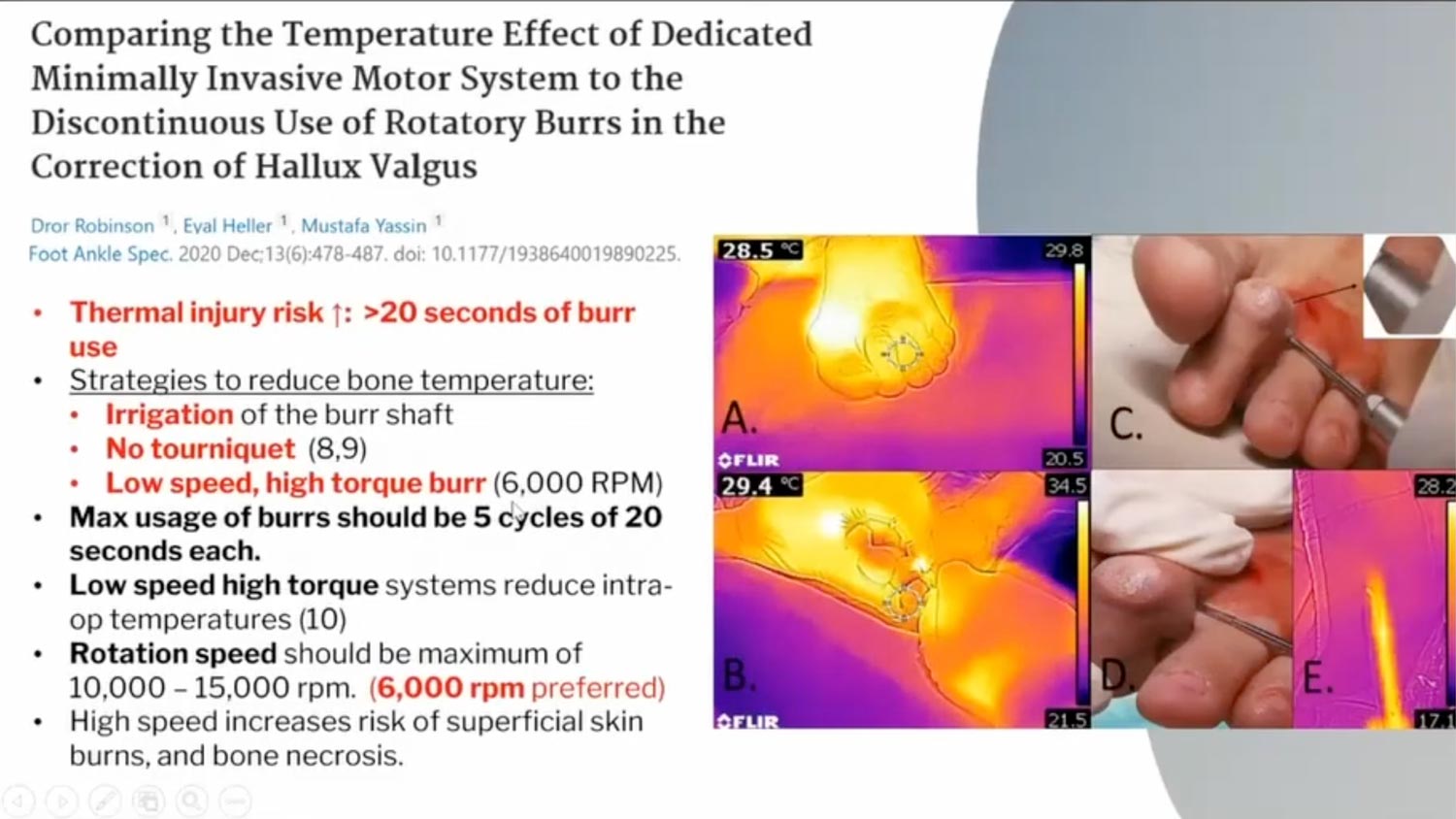
- Burr Temperature Management: Burrs can get hot enough (50 degrees Celsius for over a minute) to permanently burn bone. Strategies to prevent this include:
- Taking a 2-second break every 20 seconds to cool the burr.
- Thorough irrigation, even with a saline bulb, during bone work. (Chilled saline is not significantly better than room temperature saline).
- Using a low-speed, high-torque setting (eg, 6,000 RPM).
- Regularly cleaning burr flutes from bone debris to maintain sharpness of burr and effective cutting.
- If skin burn occurs intraoperatively, reapproximate good skin to good skin by excising burned tissue to prevent dehiscence.
- Arterial Flow: The arterial supply to the metatarsal head is planter lateral. Avoid scooping inferiorly to the metatarsal neck during bone cuts to protect these vital neurovascular structures.
- Infection Rates: MIS procedures generally have lower infection rates (0–1.6%) than open surgery, often presenting as superficial infections requiring oral antibiotics.
A Case Study in Resilience and Revision
A challenging case highlighting the importance of patient adherence features a patient who 2 weeks post-op from a successful MIS bunion correction, wore 2-inch heels for a high school reunion, resulting in 63% increased forefoot pressure. This may have led to an avascular non-union and gapping. Despite the patient being asymptomatic, swelling indicated a long-term issue. A revision was performed using a posterior-superior lateral wall calcaneal autograft to address the bone loss, reinforced with dual dorsal and medial plating, and enforced strict non-weightbearing for 3 months. This meticulous approach led to solid fusion, resolution of pain, and preserved range of motion to the first metatarsal phalangeal joint.
Key Takeaways for the MIS Clinician
A comprehensive overview underscores several crucial principles for clinicians embracing MIS:
- Know Your Anatomy: It is the foundation of safe and effective surgery.
- Master Open Surgery Too: Not all cases are amenable to MIS; proficiency in open techniques is essential.
- Practice Relentlessly: Utilize saw bones, cadaver labs, and seek opportunities for peer-to-peer visits. Industry support can provide invaluable, free learning opportunities.
- Believe in the Process: Trust Wolff’s Law and your surgical principles to achieve optimal outcomes.
MIS offers significant benefits to patients, but demands continuous learning, meticulous technique, and a deep understanding of potential complications and their management. By integrating these insights, clinicians can enhance their practice and improve patient outcomes in the evolving landscape of foot and ankle surgery.
Dr. Sugino is a fellowship-trained foot and ankle surgeon specializing in comprehensive reconstruction of the foot and ankle. She is board certified in foot and reconstructive rearfoot/ankle surgery by the American Board of Foot and Ankle Surgery (ABFAS).
She has been very active in research throughout her training, and she has multiple awards for her work. She is a speaker at many conferences around the country, and she is an active member of the American College of Foot and Ankle Surgeons (ACFAS) and the American Microsurgical Orthoplastic Society (AMOS).
This article is a summary of Dr. Sugino’s presentation, “Failed Forefoot MIS Surgery: What can you do to prevent this from happening?” from the 2025 APMA Surgical Complications Virtual Seminar on January 18, 2025. To view the full presentation with questions and answers—and see the agenda for the program, visit https://apmasurgical.lerexpo.com . Continuing education credits are available for this and many of the lerEXPO programs.





