
 By Mathias B. Forrester, BS
By Mathias B. Forrester, BS
Background: Falls are a major public health concern, causing millions of injuries in the United States (US) each year. A portion of injuries caused by falls are likely to involve the lower extremity. The objective of this study was to describe lower extremity injuries caused by falls treated at US hospital emergency departments (EDs).
Methods: Data were obtained from the National Electronic Injury Surveillance System-All Injury Program (NESS-AIP). NEISS-AIP collects data on all types and causes of nonfatal injuries treated in a stratified random sample of 66 US hospital EDs. National estimates are calculated from database records according to the sample weight assigned to each case based on the inverse probability of the hospital being selected for the NEISS-AIP sample. Cases were all records during 2005–2022 where the precipitating cause of injury was a fall and primary body part affected was the lower extremity. For the selected variables, the distribution of the national injury estimates was determined.
Results: An estimated 30,591,246 lower injuries caused by falls were treated at US hospital EDs during 2005–2022 representing 20% of the estimated total injuries caused by falls. The injured body part was 34.5% knee, 28.6% ankle, 15% lower leg, 12.4% foot, 6.8% upper leg, and 2.8% toe. The diagnosis was 33.2% strain or sprain, 27.6% fracture, 24.3% contusion or abrasion, 5.9% laceration, and 8.9% all other. Patients age 65 years and older accounted for 21.2% of the injuries. The patients were 61.7% female and 38.3% male. The location of the incident was 39.6% home, 15.3% other public property, 6.2% place of recreation or sports, 3.4% school, 3% street or highway, 1% industrial place, 0.2% farm or ranch, and 31.3% unknown location.
Conclusion: An estimated 1.7 million lower extremity injuries caused by falls were treated at US hospital EDs annually during the last 18 years. The results of this study may be useful for creating strategies to prevent lower extremity injuries caused by falls.
Falls are a major public health concern. A US health survey in 2008 found that 11.9% of the community-dwelling adults who responded reported falling in the previous year, resulting in an estimated 80 million falls.1 A 1990 mail-back questionnaire involving adults age 20–87 years observed that 20% of respondents reported falling within the past 12 months, with 8% reported falling multiple times.2 In a 1996–2001 study in California involving individuals age 45 years or older, 23% reported falling in the past year.3
 Falls result in millions of injuries in the US each year. The Centers for Disease Control and Prevention (CDC) Vital and Health Statistics reported 9.8 million fall-related injuries among US adults in 2012.4 In the national health survey, 1% of community-dwelling adults reported a fall-related injury in the prior 3 months, translating to approximately 9.9 million fall-related injuries annually.1 In the mail-back questionnaire, 8% of the people who fell fractured a bone.2 As a consequence, annually millions of people in the US are treated in emergency departments (EDs) hundreds of thousands are hospitalized, and thousands die from unintentional falls.5–8
Falls result in millions of injuries in the US each year. The Centers for Disease Control and Prevention (CDC) Vital and Health Statistics reported 9.8 million fall-related injuries among US adults in 2012.4 In the national health survey, 1% of community-dwelling adults reported a fall-related injury in the prior 3 months, translating to approximately 9.9 million fall-related injuries annually.1 In the mail-back questionnaire, 8% of the people who fell fractured a bone.2 As a consequence, annually millions of people in the US are treated in emergency departments (EDs) hundreds of thousands are hospitalized, and thousands die from unintentional falls.5–8
A portion of injuries caused by falls are likely to involve the lower extremity. The objective of this study was to describe lower extremity injuries caused by falls treated at US hospital EDs.
Methods
This retrospective epidemiologic study used data from the NESS-AIP. The NEISS-AIP has previously been described in detail in Lower Extremity Review.9 To summarize, the NEISS-AIP collects data on all types and causes of nonfatal injuries treated in a stratified random sample of 66 US hospital EDs. National estimates are calculated from database records according to the sample weight assigned to each case based on the inverse probability of the hospital being selected for the NEISS sample.10,11 The data are publicly available and de-identified, so the study is exempt from institutional review board approval.
NEISS-AIP data were downloaded from the Inter-university Consortium for Political and Social Research (ICPSR) National Archive of Criminal Justice Data (NACJD) website:
www.icpsr.umich.edu/web/NACJD/search/studies?q=national%20electronic&
Cases were all records during 2005–2022 (the most recent year of available data) where the precipitating cause of injury was a fall (Field name PCAUSE_C with numeric value 6 [Fall]) and the primary body part affected was the lower extremity (Field name BDYPT with numeric values 35, 36, 37, 81, 83, 93).
The following variables were examined: primary body part affected, diagnosis (type of injury) associated with the body part, year and month of treatment, patient disposition, location of the incident, and patient age and sex. The NEISS-AIP database contains 2 sets of fields for documenting the diagnosis and associated body part; however, only 1 set of fields was used throughout the study period–DIAG and BDYPT. (The second set of fields–DIAG2 and BDYPT2 appears to have been added in 2018.) For consistency, the study was limited to the first set of fields.
Estimate = Weighted estimate (sum of the WEIGHTA numeric field in the National Electronic Injury Surveillance System-All Injury Program database). The numbers in the WEIGHTA field are not whole numbers but include decimals. As a result of rounding to whole numbers when performing analyses, the sum of the estimates for a given variable might not equal the total. The Consumer Product Safety Commission considers an estimate unstable and potentially unreliable when the estimate is <1,200.
Analyses were performed using Microsoft 365 Access and Excel (Microsoft Corporation, Redmond, Washington). For the selected variables, the distribution of the national injury estimates was determined. National injury estimates were calculated by summing up the values in the WEIGHTA numeric field in the NEISS-AIP database. The US Consumer Product Safety Commission (CPSC), which operates the NEISS-AIP, considers an estimate unstable and potentially unreliable when the estimate is <1,200.12
Results
An estimated 30,591,246 lower injuries caused by falls were treated at US hospital EDs during 2005–2022, or an estimated average of 1,699,514 lower extremity injuries per year. This represents 20% of the estimated 152,634,485 total injuries caused by falls. Also, of the 23 different primary cause of injury grouping in the NEISS-AIP database, the highest proportion (30%) of the estimated 101,930,949 total lower extremity injuries treated at US hospital EDs during 2005–2022 were caused by falls.
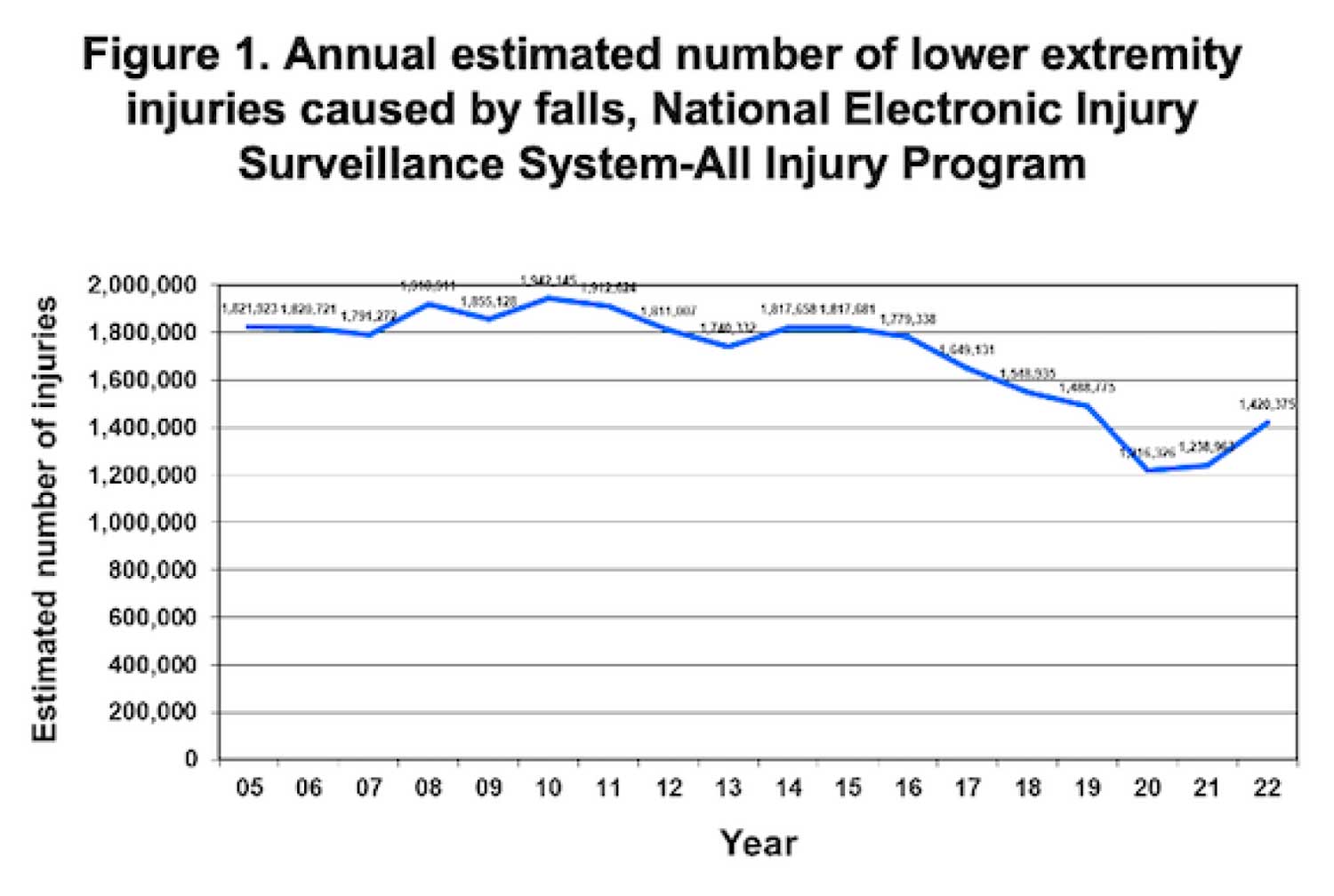
Figure 1 shows the annual estimated number of lower extremity injuries caused by falls. The estimated number of injuries increased 6.6% between 2005 and 2010 before declining 37.4% between 2010 and 2020 before increasing 16.8% between 2020 and 2022. The largest percent decline between 2 consecutive years was an 18.3% decline between 2019 and 2020. The largest percent increase between 2 consecutive years was a 14.6% increase between 2021 and 2022. There were an estimated 7,477,317 (24.4%) lower extremity injuries treated in January–March, 7,798,652 (25.5%) in April–June, 8,038,167 (26.3%) in July–September, and 7,277,111 (23.8%) in October–December.
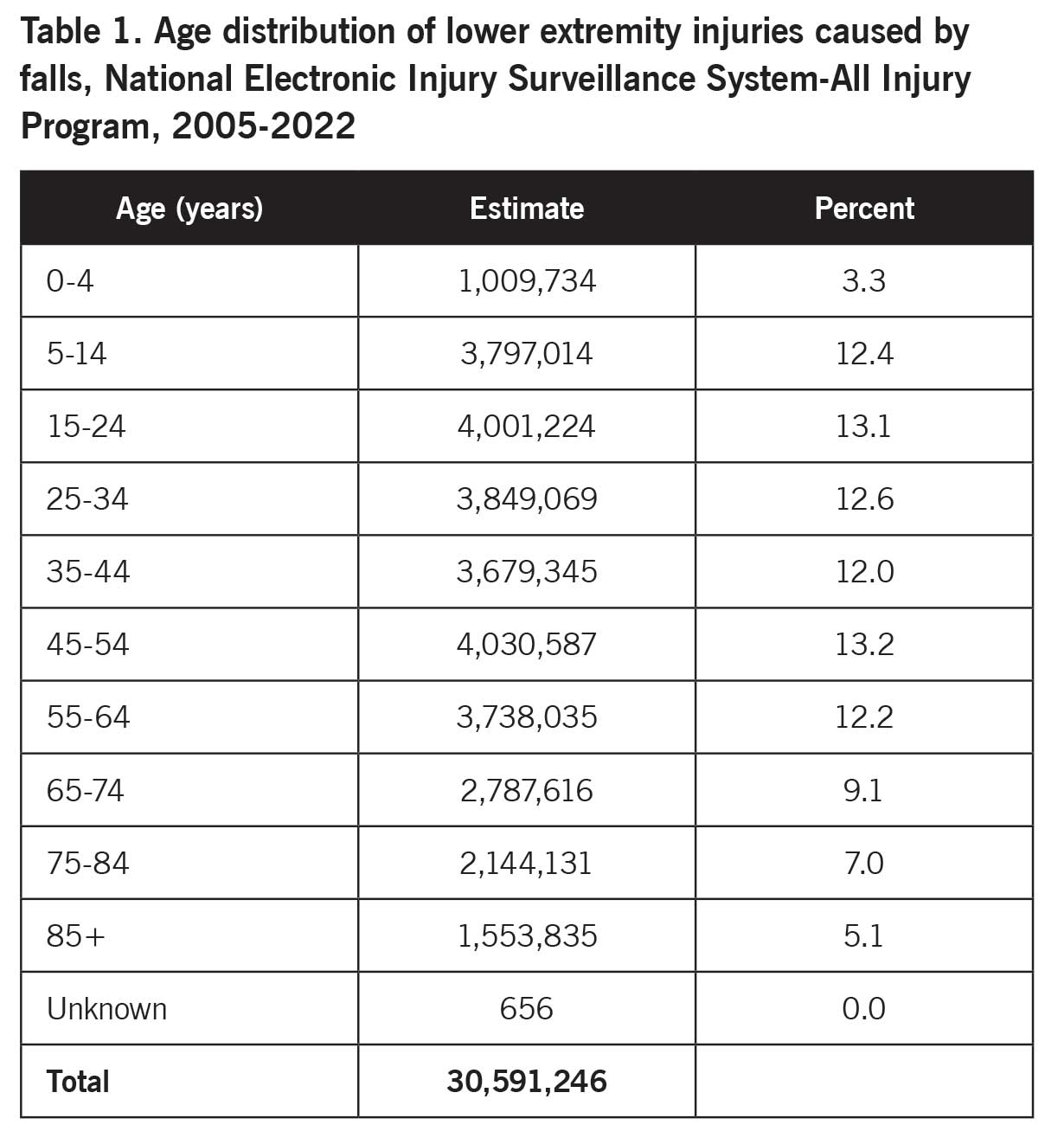
Table 1 shows the age distribution of lower extremity injuries caused by falls. Patients age 65 years and older accounted for 21.2% of the injuries. The patients were 18,879,055 (61.7%) female, 11,711,226 (38.3%) male, and 965 (0%) unknown sex. The location of the incident was 12,112,607 (39.6%) home (including manufactured or mobile home), 4,685,289 (15.3%) other public property, 1,906,146 (6.2%) place of recreation or sports, 1,043,531 (3.4%) school, 928,282 (3%) street or highway, 293,707 (1%) industrial place, 55,524 (0.2%) farm or ranch, and 9,566,160 (31.3%) unknown location.
The injured body part was 10,556,758 (34.5%) knee, 8,741,031 (28.6%) ankle, 4,575,965 (15%) lower leg, 3,793,115 (12.4%) foot, 2,072,803 (6.8%) upper leg, and 851,574 (2.8%) toe. The diagnosis was 10,148,359 (33.2%) strain or sprain, 8,455,680 (27.6%) fracture, 7,437,891 (24.3%) contusion or abrasion, 1,818,364 (5.9%) laceration, and 2,730,952 (8.9%) all other. The patient disposition was 26,986,909 (88.2%) treated or examined and released from the ED, 2,961,062 (9.7%) treated and admitted for hospitalization (within same facility), 344,981 (1.1%) transferred to another hospital and released, 121,035 (0.4%) held for observation (includes admitted for observation), 176,520 (0.6%) left without being seen or left against medical advice, and 740 (0%) unknown.
Discussion
Falls caused an estimated 30 million lower extremity injuries treated at US hospital EDs during 2005–2022. Furthermore, 20% of all injuries caused by falls involved the lower extremity, and 30% of all lower extremity injuries were caused by falls. Taken together, this indicates that falls are a major cause of lower extremity injuries.
The estimated number of lower extremity injuries caused by falls declined over a large portion of the study period–2010–2020. This decline may be due to efforts to reduce the risk of falls. Alternatively, individuals who were injured due to falls may have become more likely to seek treatment at facilities other than hospital EDs.
Of note, the greatest percent change from 1 year to the next was a 18.3% decline between 2019 and 2020. This large decline may be due to the COVID-19 pandemic declared in March 2020 and the societal disruptions associated with the COVID-19 pandemic.13 Numerous studies have reported changes in the number of illnesses and injuries because of the COVID-19 pandemic.14–18 The risk of injuries due to falls might have declined because of the changes associated with the COVID-19 pandemic. Another potential explanation is that the number of injuries due to falls might not have changed greatly but people might have been reluctant to seek treatment at hospital EDs over concern of contracting COVID-19. The increase in the estimated number of lower extremity injuries caused by falls during 2021 and 2022 suggests that, as people increasingly returned to pre-COVID-19 pandemic behaviors, their risk of injury due to falls–or tendency to visit a hospital ED to seek treatment for such injuries–was returning to normal. Still, the annual estimated number of lower extremity injuries caused by falls in 2022 was still lower than that in 2019.
Older adults (age 65 years and older) are at increased risk of falls and fall-related injuries.1,7,19 This study did not examine the rate of lower extremity injuries caused by falls among the general population. The study did find that patients age 65 years and older accounted for only 21% of the total estimated falls. Most of the patients were female. Previous studies likewise found falls to be more common among females.1,2,4,19 These observations suggest that fall prevention strategies should include all age groups and that these strategies may need to provide extra focus on females.
Most of the lower extremity injuries caused by falls with a known location of the incident occurred at home. However, the next highest proportion occurred at other public property followed by a place of recreation or sports. This suggests that, while prevention strategies may focus on the home, the strategies should also include other locations where falls are next most likely to occur.
Strains or sprains accounted for one-third of the diagnoses, with fractures and contusions or abrasions each accounting for an additional one-fourth. In general, these types of injuries might not be considered to require extensive hospital intervention. This study found that 88% of the patients were treated or evaluated and released from the ED. However, an additional 11% of the patients were either admitted to the hospital or transferred to another hospital.
This study has limitations. For most of the study period, only a single diagnosis and affected body part were documented in the NEISS-AIP database. For consistency, the study was restricted to these fields. However, a fall may result in multiple types of injuries affecting 1 or more body parts. Thus, the number of falls that caused lower extremity injuries and were included in this study should be considered a lower estimate. Second diagnosis and body part fields were added in 2018. Even if lower extremity injuries documented in these fields were included in the study, the number of lower extremity injuries would probably still be underestimated.
Furthermore, the NEISS-AIP database only includes data on injuries treated at hospital EDs. Injuries treated elsewhere, such as at home, a physician’s office, or an other healthcare facility, would not be included. Injuries treated at these other facilities would provide a clearer picture of lower extremity injuries caused by falls.
In conclusion, the estimated number of lower extremity injuries caused by falls that were treated at US hospital EDs has declined over the last 18 years. Although patients age 65 years and older are considered at increased risk of fall-related injuries, only 21% of the patients in the study were in this age group. Most of the patients were female. While most of the injuries with a known location of the incident occurred at home, the next-highest proportion occurred at other public property followed by a place of recreation or sports. The information in this study may be useful for creating strategies to prevent lower extremity injuries caused by falls.
Mathias B. Forrester, BS, is an independent researcher in Austin, Texas. Now retired, he has performed public health research for various universities, government programs, and other organizations for 40 years.
- Verma SK, Willetts JL, Corns HL, Marucci-Wellman HR, Lombardi DA, Courtney TK. Falls and fall-related injuries among community-dwelling adults in the United States. PLoS One. 2016;11(3):e0150939.
- Mertz KJ, Lee DC, Sui X, Powell KE, Blair SN. Falls among adults: the association of cardiorespiratory fitness and physical activity with walking-related falls. Am J Prev Med. 2010;39(1):15-24.
- Li W, Keegan TH, Sternfeld B, Sidney S, Quesenberry CP Jr, Kelsey JL. Outdoor falls among middle-aged and older adults: a neglected public health problem. Am J Public Health. 2006;96(7):1192–1200.
- Adams PF, Kirzinger WK, Martinez ME. Summary health statistics for the U.S. population: National Health Interview Survey, 2012. Vital Health Stat 10. 2012;(255):1-110.
- Centers for Disease Control and Prevention (CDC). 10 leading causes of injury deaths by age group highlighting unintentional injury deaths, United States– 2010. Centers for Disease Control and Prevention. 2010. Available at http://web.archive.org/web/20140911181934/http://www.cdc.gov/injury/wisqars/pdf/10LCID_Unintentional_Deaths_2010-a.pdf.
- Bergen G, Chen L, Warner M, Fingerhut L. Injuries in the U.S.: 2007 Chartbook. Hyattsville, MD: National Center for Health Statistics; 2008.
- Kung HC, Hoyert DL, Xu J, Murphy SL. Deaths: final data for 2005. Natl Vital Stat Rep. 2008;56(10):1–120.
- Centers for Disease Control and Prevention. Accidents or unintentional injuries. July 26, 2024. Available at https://www.cdc.gov/nchs/fastats/accidental-injury.htm . Accessed October 1, 2025.
- Forrester MB. Dog bites of the lower extremity treated at hospital emergency departments. Lower Extremity Review. 2022;14(9):47-55.
- United States Department of Health and Human Services. Centers for Disease Control and Prevention. National Center for Injury Prevention and Control, and U.S. Consumer Product Safety Commission. National Electronic Injury Surveillance System All Injury Program, 2019. Inter-university Consortium for Political and Social Research [distributor], December 15, 2021.
- Ehlman DC, Haileyesus T, Lee R, Ballesteros MF, Yard E. Evaluation of the National Electronic Injury Surveillance System – All injury program’s self-directed violence data, United States, 2018. J Safety Res. 2021;76:327-331.
- United States Consumer Product Safety Commission. National Electronic Injury Surveillance System (NEISS). Available at https://www.cpsc.gov/Research–Statistics/NEISS-Injury-Data/Explanation-Of-NEISS-Estimates-Obtained-Through-The-CPSC-Website . Accessed October 1, 2025.
- Muccari R, Chow D, Murphy J. Coronavirus timeline: Tracking the critical moments of Covid-19. NBC News. December 29, 2020. Available at https://www.nbcnews.com/health/health-news/coronavirus-timeline-tracking-critical-moments-covid-19-n1154341. Accessed October 1, 2025.
- Forrester MB. Changes in product-related lower extremity injuries treated at emergency departments during the COVID-19 pandemic. Lower Extremity Review. 2021;13(8):23-31.
- Sabbagh RS, Shah NS, Kanhere AP, Hoge CG, Thomson CG, Grawe BM. Effect of the COVID-19 pandemic on sports-related injuries evaluated in US emergency departments. Orthop J Sports Med. 2022;10(2):23259671221075373.
- Nabavizadeh B, Hakam N, Abbasi B, Shaw NM, Breyer BN. Impact of the COVID-19 pandemic on emergency department visits for genitourinary trauma. BMC Urol. 2022;22(1):83.
- Maeng D, Li Y, Lawrence M, Keane S, Cross W, Conner KR, Lee HB. Impact of mandatory COVID-19 shelter-in-place order on controlled substance use among rural versus urban communities in the United States. J Rural Health. 2023;39(1):21-29.
- Albright JA, Testa EJ, Testa JW, Marcaccio S, Meghani O, Owens BD. Trends in lower extremity injuries presenting to emergency departments during the COVID-19 pandemic. J Emerg Med. 2022;63(2):169-177.
- Centers for Disease Control and Prevention (CDC). Public health and aging: nonfatal injuries among older adults treated in hospital emergency departments – United States, 2001. MMWR Morb Mortal Wkly Rep. 2003;52(42):1019–1022.





