

iStock #874810704
Offloading is key to preventing small concerns from becoming life-threatening, but adherence remains less than optimal
By Janice T. Radak
The not-so-secret truth: diabetes and its precursor, prediabetes, have reached epidemic status in the United States: More than 100 million Americans are living with the disease.1
Based on data from 2015, the US Centers for Disease Control and Prevention last year reported that 30.3 million Americans – 9.4% of the U.S. population – have diabetes.1 But not everyone who has diabetes has been diagnosed: nearly one-quarter of those who meet specified fasting glucose and hemoglobin A1c criteria have not been diagnosed, meaning they do not know they have diabetes and therefore, their healthcare providers do not know either.
Adding to the burden, another 84.1 million have prediabetes, a condition that if not treated often leads to type 2 diabetes within 5 years. Significantly, more than one-third of US adults have prediabetes and do not know it.1
What does this mean? Given that there is no cure for diabetes, it means there are more than 200 million diabetic feet in the United States today that require protection, and that number will only continue to grow. Once blood glucose metabolism goes awry, each foot of a person with diabetes becomes a unique risk factor for potentially life-threatening complications. Care of each foot requires daily maintenance that takes time and an attention to detail that adds to the burden of this disease—both for the individual and his or her healthcare providers—because protecting the diabetic foot is no easy feat.

Centers for Disease Control and Prevention. Available at
https://www.cdc.gov/media/releases/2017/p0718-diabetes-report.html
What diabetes does
The healthy—non-diabetic—human body is a pretty amazing machine that keeps itself functioning properly with a 24/7/365 process of maintenance and repair. Diabetes disrupts that homeostasis.
Diabetes mellitus (diabetes) is a group of diseases that negatively affect how the body produces and/or uses insulin, leading to the abnormal metabolism of carbohydrates; the result is hyperglycemia, or elevated levels of glucose in the blood and urine. Chronic hyperglycemia damages blood vessels (angiopathy), leading to well-known microvascular and macrovascular complications.2 Microvascular (small vessel) complications include retinopathy (eye disease), nephropathy (kidney disease), and neuropathy (neural damage that occurs throughout the body). Macrovascular (large vessel) complications can accelerate cardiovascular disease, leading to heart attacks at younger ages than the general population, and cause cerebrovascular events, such as strokes. And data show that complications in one area can exacerbate complications in other areas, such as hypertension exacerbating nephropathy.3 Furthermore, diabetes is associated with depression and dementia, which can impact an individual’s ability to perform needed self-care.
Key players in this discussion are peripheral vascular disease and diabetic neuropathy.
Peripheral Vascular Disease: Peripheral vascular disease (PVD; sometimes called peripheral arterial disease [PAD]), is a circulation disorder that causes narrowing, blockage, or spasms in veins, arteries or lymphatic vessels, compromising blood flow throughout the body, meaning organs and limbs may not receive the oxygen and nutrients they need to thrive. The narrowing is caused by increased plaque on vessel walls, believed to be a response to hyperglycemia, though it is also common in people without diabetes.
Diabetic Neuropathy: More than 65% of people with diabetes will develop some degree of peripheral neuropathy (PN), and its prevalence increases with both age and duration of disease.4 In a study published in Diabetes Care, Abbott et al reported a prevalence of painful neuropathy symptoms (neuropathic pain) in 34% of 15,692 UK patients.5 Although neuropathic pain can be excruciating for some patients, dramatically affecting their quality of life and productivity, PN is more commonly known for its theft of sensations of all types, from pain to temperature to proprioception, creating the insensate foot.4 Risk of developing a first foot ulcer is nearly 7-fold higher in those with an insensate foot than in patients with diabetes who do not have PN.
Thermographic Foot Patterns Differ Among Diabetes Complications
Common diabetic foot complications such as ischemia and neuropathy are known to have an effect on the temperature of the foot. In a recent study, Gatt et al1 postulated that changes in temperature of the foot may be indicative of the presence of such complications. They used thermography (medical infrared imaging) to visualize the temperature distribution of the feet of participants living with diabetes mellitus (DM) with or without complications versus healthy controls.
Their findings, displayed in Figures 1 and 2, show significant differences in the mean temperatures amongst the 5 groups (Healthy Adults; DM healthy [with diabetes but no significant medical comorbidities and/or complications]; peripheral arterial disease [PAD] [ABPI < 0.6 and monophasic Doppler spectral waveforms at the ankles, but no neuropathy]; Neuropathic only [positive 10-gram monofilament at any one of 10 tested sites and/or reduced vibration perception threshold as measured with a tuning fork and an ABPI between 0.9 and 1.3]; and Neuroischemic [ABPI < 0.9 and neuropathy]).
Using the Turkey test, which clusters the 5 groups into 2 groups, participants in the PAD, Neuropathic only, and Neuroischemic groups had significantly higher mean temperatures of the feet when compared to the Healthy and DM healthy groups. Using logistic regression analyses, neither toe location nor plantar location was found to be a significant predictor; but in both cases, temperature was. For toe temperature, the odds ratio that a participant has neuropathy, neuroischemia, or PAD increases 24.7% for every 1°C increase in toe temperature (range, 19.8% to 29.7%). For plantar forefoot temperature, the odds ratio that a participant has neuropathy, neuroischemia, or PAD increases 28.9% for every 1°C increase in plantar temperature (range 19.8% to 29.7%).
The authors note that should a rise in temperature be detected in the diabetic foot, there is a higher likelihood that diabetic foot complications have set in, reinforcing the findings by Sun6 who reported that thermographic patterns may change as early as one week prior to ulceration. Sun also reported that clinical examination and nerve conduction studies may not be adequate for screening at-risk diabetic feet at an early stage.
The authors conclude that their study confirmed that the mean temperatures of the toes and forefeet of participants in the complications groups exhibit significantly higher temperatures than those of healthy participants including those with diabetes who had no complications. These results, they argue, indicated that thermography demonstrated potential as a screening or clinical investigation tool, although more research is warranted.
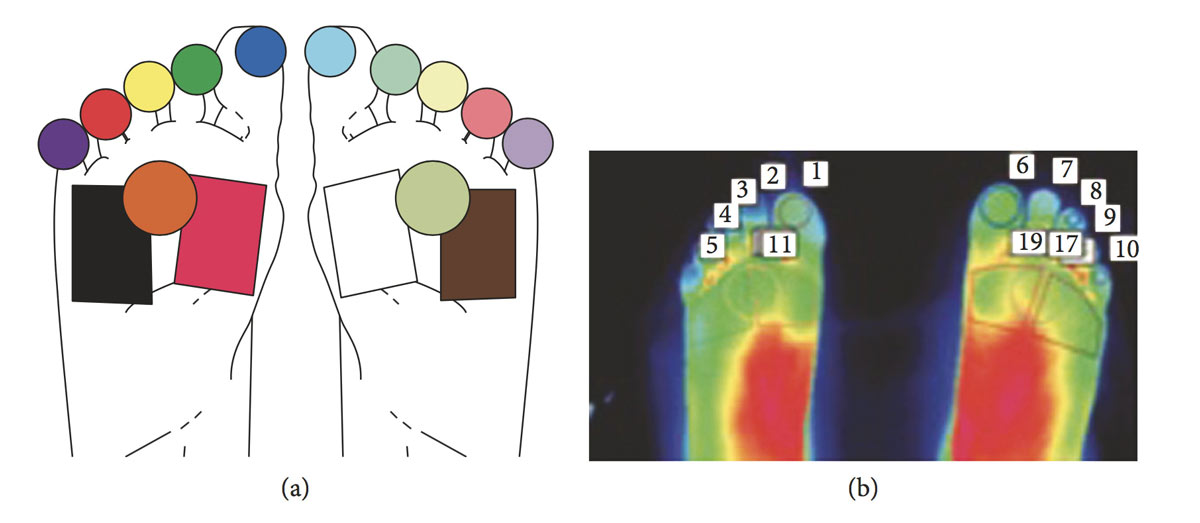
Figure 1: (a) Diagram showing the foot regions considered for temperature extraction. (b) An actual thermal image and the corresponding regions of interest. The temperatures from the toe regions and forefoot regions were considered for further analysis.
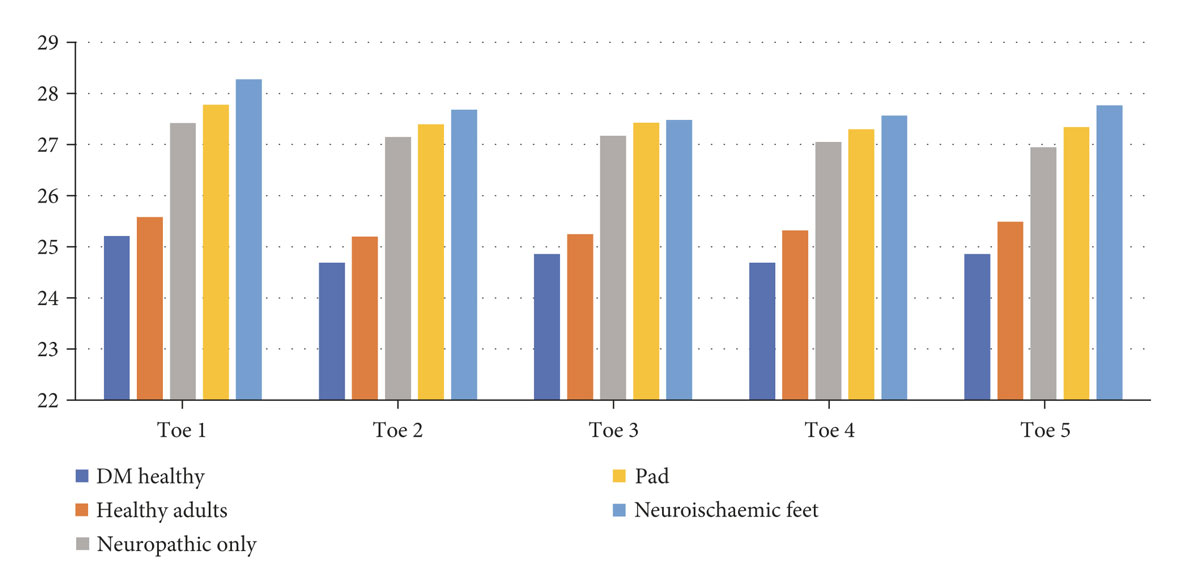
Figure 2: Toe temperature distribution.
- Excerpted and summarized from Gatt A, Falzon O, Cassar K, et al. Establishing Difference in Thermographic Patterns between the Various Complications in Diabetic Foot Disease. Int J Endocrin. 2018:9808295.
While PN gets the lion’s share of attention, autonomic neuropathy plays a critical role in creating the diabetic foot as well.4 It leads to abnormal thermoregulatory changes that act to reduce sweating, particularly in the feet, resulting in dry skin. Untreated dryness can cause skin to fissure and crack, creating entry points for bacteria and subsequent infections. Further, in the absence of PVD, these thermoregulatory changes can result in increased blood flow, leading to a warm foot. Using clinical, nerve conduction, and autonomic evaluations, Sun and colleagues looked at the relationship of plantar skin temperatures to DN in 25 healthy controls and 69 participants with diabetes.6 The diabetes cohort included 29 participants with a sympathetic skin response (SSR+ group) that was similar to controls; 22 participants who had no SSR in both feet (SSR- group), and 18 participants who had no SSR in both feet and presented with preulcerative skin lesions (at-risk group). Foot temperatures were significantly higher in the at-risk group (30.2°C) compared to the control group (26.8°C), the SSR+ group (27.1°C ) and the SSR- group (27.9°C ). The authors noted that the at-risk group showed more abnormalities in nerve conduction than either the SSR- or SSR+ groups (55% vs 23% or 14%, respectively; p < 0.02). They concluded that these increased foot temperatures signified early sympathetic damage in diabetic feet and may be present up to a week before ulceration. The authors also noted screening diabetic at-risk feet at early stages may require more than clinical examination or nerve conduction. (See page 21, “Thermographic Foot Patterns Differ Among Diabetes Complications.”)
How much do these conditions contribute to the dreaded lower extremity amputation (LEA)? In a just-published study from the University of Kansas Medical Center, researchers sought to understand how prevalent DN, PVD and foot ulceration are in patients with diabetes who subsequently had LEA. Of the 844 diabetes patients Alothman et al7 identified, nearly 80% (699) had one or more of the risk factors before LEA: 49% (414) had neuropathy, 48% (402) had a foot ulcer, and 58% (495) had a PVD diagnosis. Further investigations showed that multiple risk factors were not uncommon: 29% had two risk factors and 24% had three risk factors.
Diabetes affects biomechanics
Diabetic foot ulcers do not arise from diabetes alone; biomechanics play a role as well. While peak pressure was initially thought to be a key predictor, evolving technology is validating that peak shear stress may be more important.
For more than a decade, Metin Yavuz, PhD, and colleagues have been conducting studies examining the role shear plays in the breakdown of tissues under the skin that lead to ulceration.8-14 In a 2007 report that compared participants with diabetes to healthy controls, they found that in most of those with diabetes, stress peak pressure and peak shear sites under the foot did not overlap. Furthermore, there was more than 1 inch separating the site of maximum pressure from the site of maximum shear for 60% of the participants with diabetes.10 In a 2008 study that also compared participants with diabetes to healthy controls, Yavuz et al found no significant difference in peak pressure between the groups.10 However, in the group with diabetes, peak anteroposterior and resultant shear were reported to be 33% and 31% higher (p = .014 and p = .016, respectively) despite the fact they walked approximately 15% slower. In another 2008 study of 558 adults in Pittsburgh, Brach et al15 identified the improper pressure distribution of a shuffling gait as a potential causative factor for increased shear forces in those with diabetes.
More recent work by Yavuz identifies plantar shear as having a clinically significant role in ulceration and suggests the combination of both pressure and shear variables would be more effective in identifying and preventing ulceration.14 Writing for LER in 2010,16 Yavuz noted: “The fact that shear forces under the foot occur twice as frequently as vertical forces suggests that shear forces play a major role in ulceration despite lower magnitudes relative to pressure. The reason involves the principle of the ‘fatigue failure’ mechanism—the progressive failure of an object due to repetitive loading.”
Repetitive loading in the diabetic environment creates vulnerability in the diabetic foot, as the person with diabetic neuropathy does not have the painful sensation that would allow them to naturally change their gait in response to the negative stimuli. Strategically managing pressure, shear, and friction, is required.
Protecting the diabetic foot
Numerous studies have proven the benefit of diabetes self-care education in protecting the person with diabetes from numerous complications. For a discussion on protecting the diabetic foot with diabetes self-care education, see Richard Schilling’s Expert Commentary: Diabetes Self-care Adherence: Whose Responsibility Is It? What’s a Clinician’s Role?, page 26, as well as the excerpt from People with Diabetes Foot Complications Do Not Recall Their Education: A Cohort Study, page 27.
Despite spending the majority of their lives “inside,” socks can provide invaluable protection to the diabetic foot as they serve as the interface between the skin and the shoe. While the wrong sock can wreak havoc, the right kind of sock can provide multiple benefits, not the least of which is reducing friction and shear inside an off-the-shelf shoe. Modern knitting machines with nearly 200 needles allow manufacturers to use finer yarns and mix various kinds of fibers, creating a safer, non-irritating sock with flat—or even no—toe seams. Today’s highly engineered socks can be anatomically sculpted, provide non-constricting gradient pressure, or come with cushioned soles (forefoot, rearfoot, entire sole) or other custom-cushioning options. They can be latex-free; include copper-infused yarns, merino wool, or other moisture-wicking materials; or even have built-in sensors that monitor foot temperature throughout the day. And there are antimicrobial and antifungal finishes that can prevent reinfection. As the sports and fitness craze drives clothing technology, therapeutic socks are no longer something just for your grandmother.


Figure 1: A seesaw model illustrating how different factors affect adherence to wearing therapeutic shoes.
Notes: Box position represents the direction of the effect (toward adherence or nonadherence) and box size represents the weight of the factor. (A) A person believing that wearing therapeutic shoes reduces ulceration risks somewhat compared to other shoes, but this is outweighed by the fact that he finds his therapeutic shoes less attractive, a factor he gives more weight to. The net result is low adherence to wearing his therapeutic shoes. (B) The same person as in (A), after being convinced that wearing therapeutic shoes reduces ulceration risks substantially compared to other shoes. (C) The same person as in (A), after having reprioritized shoe appearance and ulceration risks.
Second line of defense: Offloading. Known as the gold standard for managing problems in the diabetic foot, it is used for preventing problems, treating wounds, and long-term maintenance of chronic conditions. Indeed, offloading devices have been shown to reduce forefoot peak pressures by 90% or more, compared to barefoot walking.17 Various types of offloading devices are available, both custom and off-the-shelf, and include: orthoses, total contact cast, knee- or ankle-height removable walker cast (boot), and extra-depth shoes. Each device has unique characteristics that were recently described by McGuire.18
Foot orthoses have 7 objectives:19
- Provide shock absorption and shock attenuation
- Relieve areas of high plantar pressure, redistributing weight bearing pressures over the entire plantar surface
- Support, splint, and protect healed fracture locations using the total contact concept
- Reduce shear
- Control, stabilize, support, or correct flexible deformities
- Limit motion of affected joints
- Accommodate fixed deformities.
Functional orthoses, which are typically made of semi-rigid material (eg, plastic or graphite) are prescribed to control abnormal motion that may be causing foot pain, or to treat injuries. Accommodative orthoses, which provide added support and cushioning, are crafted from softer materials and are often designed to break down over a period of months and be replaced on a schedule. These are commonly used to for diabetic foot ulcers.
Orthoses can be customized in myriad ways as manufacturers use thousands of standard materials (eg, Ethylene Vinyl Acetate [EVA], Plastazote, Poron, Duraform, dual and multi-laminates, cork) as well as some highly specialized components (eg, silver fibers) to address specific orthotic needs, such as shock absorption, moisture deflection, or coefficient of friction. As CAD-CAM machining is becoming a more common form of manufacture, products are being made available not only in a variety of colors, but also in a variety of widths and thicknesses, allowing for an even more precise fit.
Proper fit, especially of shoes, plays a major role in protecting the diabetic foot from the repetitive microtraumas of shear and high peak pressures that can lead to skin breakdown.19-21 Plantar pressures and frictional shear forces often work together to create calluses, which may be an important outward sign of improperly fitted shoes, as ulcers often occur in these locations. More importantly, however, frictional shear forces act first between the layers of the skin rather than at the surface so confirming proper fit—shoe size and shape are appropriate and shoe fits snugly—is mandatory.19,20
Janisse and Janisse identified three factors in selecting a therapeutic shoe for a given patient: the patient’s health, the patient’s foot shape and type, and the patient’s daily activities.19 Shoes need to match the shape of the patient’s foot as well as provide enough depth to contain any needed orthotic devices and prevent pressure from being applied across the dorsum. They identify a properly fitted shoe as one that leaves 1/2 inch between the end of the longest toe and the front of the shoe and that allows for some movement of the heel to accommodate changes during gait.
Medicare covers therapeutic shoes with additional orthotic inserts for patients with diabetes when prescribed by a physician or qualified non-physician practitioner. However, proper documentation with appropriate coding is required; forms for documentation can be obtained at www.cms.gov.
Will they wear them?
A recent systematic review by Jarl and Lundqvist in the journal Patient Preference and Adherence22 looked at the adherence to wearing therapeutic shoes among almost 500 patients across 6 studies. Traditional reasons cited for not wearing therapeutic shoes were that the shoes were unattractive, too big, uncomfortable, or difficult to walk in. The authors wanted to better understand other factors that may influence the decision to wear these shoes.
They found evidence that sex, diabetes duration, or ulcer history are not good predictors for who will use their shoes.22 Why a person does something, they wrote, may be due to how they weight the multiple factors involved. For example, Person A may find the shoes to be unattractive and not wear them for that reason, while Person B may find the shoes unattractive but wear them because he perceives there is some other benefit. Their model demonstrates how different patients may weight the same items (Figure 1).
Jarl and Lundqvist connect their findings to Knowles and Boulton’s assertion from 20 years ago23 that a person must be convinced of the severity of the foot condition to understand the benefit of wearing the therapeutic shoes. And they note that two recent studies found that adherence to use of assistive technology was associated with its perceived benefits.22
Understanding why patients choose to wear their therapeutic shoes as prescribed is a challenge for clinicians around the globe. While the evidence is clear that therapeutic shoes, boots, socks, and orthoses protect the diabetic foot, helping patients perceive—and act on—that reality remains a challenge.
- Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2017. Atlanta, GA: Centers for Disease Control and Prevention, U.S. Dept of Health and Human Services; 2017.
- Forbes JM, Cooper ME. Mechanisms of Diabetic Complications. Physiol Rev. 2013;93:137-188.
- Boulton AJM, Vileikyte L, Ragnarson-Tennvall G, Apelqvist J. The global burden of diabetic foot disease. Lancet 2005;366: 1719-24.
- Boulton AJM. The diabetic foot. In De Groot LJ, Chrousos G, Dungan K, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Updated Oct. 26, 2016. Accessed Oct. 20, 2018 at https://www.ncbi.nlm.nih.gov/books/NBK409609/.
- Abbott CA, Malik RA, van Ross ER, Kulkarni J, Boulton AJ. Prevalence and characteristics of painful diabetic neuropathy in a large community-based diabetic population in the UK. Diabetes Care. 2011; 34: 2220-2224.
- Sun PC, Lin HD, Jao SH, Ku YC, Chan RC, Cheng CK. Relationship of skin temperature to sympathetic dysfunction in diabetic at-risk feet. Diabetes Res Clin Pract. 2006 Jul;73(1):41-6.
- Alothman S, Alenazi A, Waitman LR, LeMaster J, Kluding P. Neuropathy and Other Risk Factors for Lower Extremity Amputation in People with Diabetes Using a Clinical Data Repository System. J Allied Health. 2018 Fall;47(3):217-221.
- Yavuz M, Botek G, Davis BL. Plantar shear stress distributions: Comparing actual and predicted frictional forces at the foot-ground interface. J Biomech. 2007;40:3045-3049.
- Yavuz M, Erdemir A, Botek G, Hirschman GB, Bardsley L, Davis BL. Peak plantar pressure and shear locations: Relevance to diabetic patients. Diabetes Care. 2007;30(10):2643-2645.
- Yavuz M, Tajaddini A, Botek G, Davis BL. Temporal characteristics of plantar shear distribution: Relevance to diabetic patients. J Biomech. 2008;41(3):556-559.
- Yavuz M. American Society of Biomechanics. Clinical Biomechanics Award 2012: plantar shear stress distributions in diabetic patients with and without neuropathy. Clin Biomech (Bristol, Avon). 2014;29:223-229.
- Yavuz M, Brem RW, Glaros AG, et al. Association between plantar temperatures and triaxial stresses in individuals with diabetes. Diabetes Care. 2015;38:e178-e179.
- Yavuz M, Master H, Garrett A, Lavery LA, Adams LS. Peak Planta Shear and Pressure and Foot ulcer locations: a call to revisit ulceration pathomechanics. Diabetes Care. 2015;38:e184-e185.
- Yavuz M, Ersen A, Hartos J, Schwarz B, Garrett AG, Lavery LA, Wukich DK, Adams LS. Plantar Shear Stress in Individuals with a history of diabetic foot ulcer: an emerging predictive marker for foot ulceration. Diabetes Care. 2017;40:e14-e15.
- Brach JS, Talkowski JB, Strotmeyer ES, Newman AB. Diabetes mellitus and gait dysfunction: possible explanatory factors. Phys Ther. 2008 2008;88:1365-1374.
- Yavuz M. Plantar shear: Casting light on ‘dark matter.’ Lower Extremity Review. 2010. Available at https://lermagazine.com/article/plantar-shear-casting-light-on-dark-matter.
- Gutekunst DJ, Hastings MK, Bohnert KL, Strube MJ, Sinacore DR: Removable cast walker boots yield greater forefoot off-loading than total contact casts. Clin Biomech (Bristol, Avon) 2011; 26: 649-654.
- McGuire J. Expert Opinion: Advances and alternatives in diabetic ulcer offloading. Lower Extremity Review. 2018. Available at https://lermagazine.com/article/expert-opinion-advances-and-alternatives-in-diabetic-ulcer-offloading
- Janisse D, Janisse E. Pedorthic management of the diabetic foot. Prosthetics and Orthotics International. 2015;391);40-47.
- Sulzberger MB, Cortese TA, Fishman L, et al. Studies on blisters produced by friction. J Invest Dermatol 1966; 47: 456-465.
- Michaud TC. Orthotic Dispensing, Shoe Gear, and Clinical Problem Solving. In: Foot orthoses and other forms of conservative foot care. Michaud TC (ed.) Newton, MA: Michaud Chiropractic Center, 1997, pp. 223-235.
- Jarl G, Lundqvist L-O. Adherence to wearing therapeutic shoes among people with diabetes: a systematic review and reflections. Patient Prefer Adherence. 2016;10:1521-1528.
- Knowles EA, Boulton AJ. Do people with diabetes wear their prescribed footwear? Diabetes Med. 1996;13(12):1064-1068.





