
By Angela Kelley, PA-C, MSM
Varicose veins affect nearly one third of the adult population and are considered early warnings of the more serious chronic venous insufficiency. Early recognition and prevention are key to suppressing potential life-threatening damage and maintaining patient quality of life.
 Varicose veins (VVs)—those bulging, twisted blood vessels typically seen on the legs—are more than an esthetic issue. They can be painful and affect patients’ quality of life; left untreated, they can lead to life-threatening chronic venous insufficiency and venous ulcers and warrant a clinician’s attention.
Varicose veins (VVs)—those bulging, twisted blood vessels typically seen on the legs—are more than an esthetic issue. They can be painful and affect patients’ quality of life; left untreated, they can lead to life-threatening chronic venous insufficiency and venous ulcers and warrant a clinician’s attention.
VVs are a common occurrence noted in healthcare. This article is the second of a 2-part-primer and includes information on treatment, prevention, and complications of this condition. Part I appeared last month and included information on anatomy, physiology, and pathophysiology, how to diagnose VVs, risk factors for occurrence, clinical presentation, and differential diagnoses. This article will focus on treatment, prevention, and complications of this condition. There are additional terms that will be explored such as chronic venous insufficiency (CVI), and chronic venous disease (CVD); however, it is important to note at the outset that these terms are not interchangeable with the term varicose veins.
Definitions
Varicose Veins
Varicose veins (VVs) are superficial veins that are dilated and bulging with diameters measuring 3 mm or greater that can progress to become more enlarged and more tortuous.1 Patients with VVs can be either asymptomatic or have pain and even bleeding if progression occurs. VVs are the most common manifestation of CVD and usually manifest as stage C2 in the CEAP (see below).2
Chronic Venous Disease
Chronic venous disease (CVD) is a general term describing complications in the venous system caused by dysfunctional valves and venous reflux.3 Differentials related to CVD should include causes of lower extremity edema including hypoalbuminemia, cardiac insufficiency, hypothyroidism, and more.2,4
Chronic Venous Insufficiency
Chronic venous insufficiency (CVI) is mainly caused by ambulatory venous hypertension due to abnormal blood flow from reflux of venous valves, obstruction of venous valves, or a combination of both.1 The causes of CVI include VVs as well as reticular veins, telangiectasias, pigmentation, edema, lipodermatosclerosis, eczema, venous ulcers, and atrophie blanche. These additional exam findings are important to note to determine differential diagnoses that could cause venous abnormalities.5
CEAP Classification
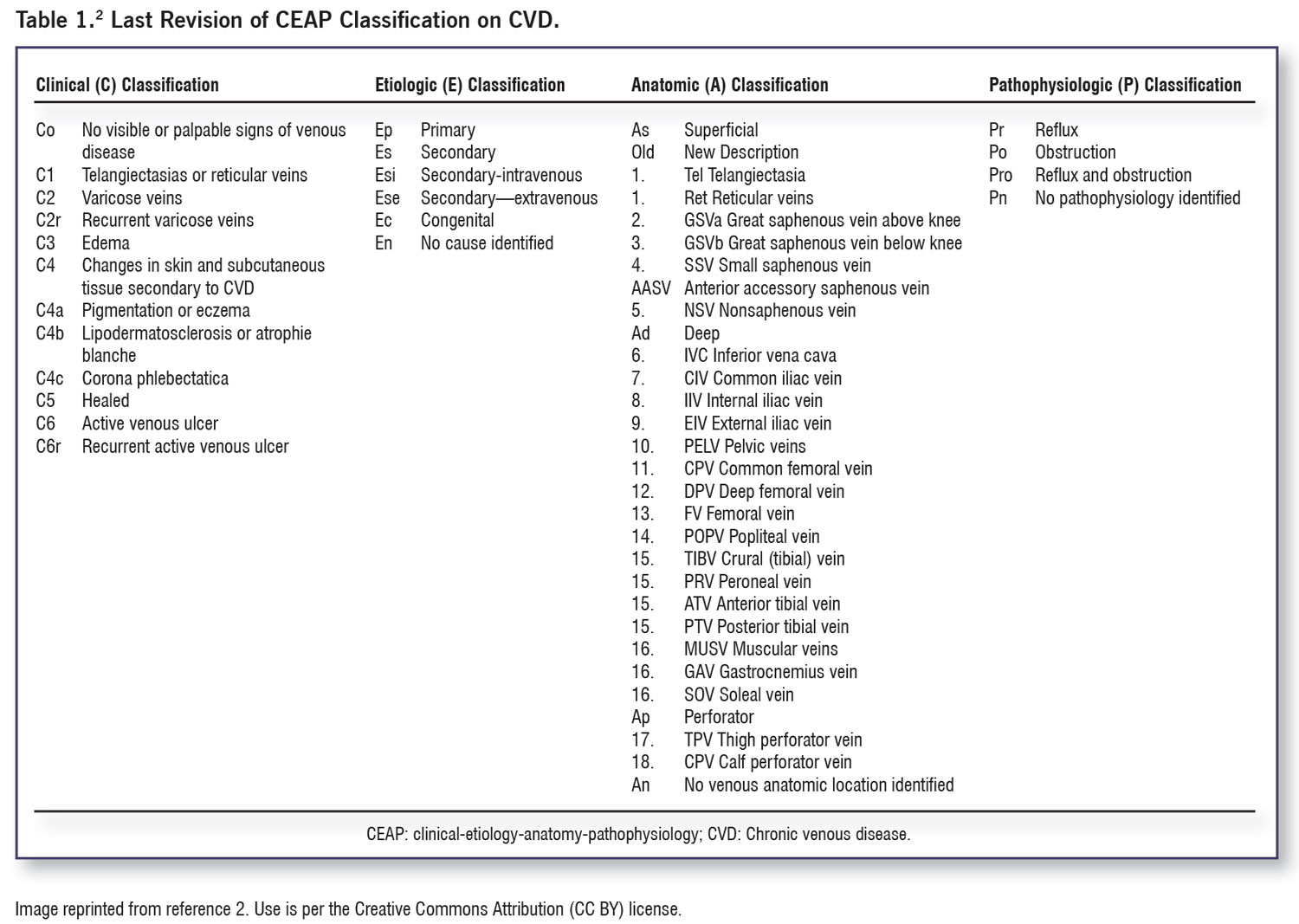
VVs represent one aspect of venous disease, which is generally reported using the international standard known as CEAP: Clinical-Etiology-Anatomy-Pathophysiology Classification (Table 1).2 CEAP, which is based on clinical manifestations of chronic venous disorders, helps to standardize diagnoses, improve communications among clinicians, and facilitates research. Class C0 represents no visible sign of venous disease; classes C1–3 typically denote CVD, while classes C4-6 are indicative of the more severe CVI.
Treatment

Figure 1: The lower extremity venous system, and changes to varicose veins. The lower extremity has an intricate system of superficial and deep veins connected by perforator veins. Excessive vein wall dilation and incompetent venous valves lead to superficial dilated spider veins or engorged and tortuous varicose veins. Image reprinted from Chen Y, Peng W, Raffetto JD, Khalil RA. Matrix Metalloproteinases in Remodeling of Lower Extremity Veins and Chronic Venous Disease. Prog Mol Biol Transl Sci. 2017;147:267-299. DOI: 10.1016/bs.pmbts.2017.02.003. Elsevier Copyright ©2017; all rights reserved.
Treatment for VVs depends upon the cause, symptomatology, and severity of the condition. Treatment of the underlying causes, conservative management, combination therapy, and interventional treatments all have their place.5 Cosmetic treatment may also be chosen if patients are asymptomatic and more concerned with appearance12; however, the potential lack of medical coverage for cosmetic procedures must be discussed with patients.19
Conservative Management
Treatment options for VVs vary based on the concern for appearance as well as the level of pain and potential for progression of the condition. Conservative management for VVs includes modifications of lifestyle, such as avoiding straining or prolonged standing and wearing clothing that is nonrestrictive; interventions to decrease edema in lower extremities; and reduction of cardiovascular risk.5 Additional measures such as compression stockings and phlebotonics, such as dietary supplements, are available; however, long-term evidence is lacking as compression stockings have only been recommended as first-line treatment for VVs in pregnant patients.1,5,6 Compression stockings have been noted, however, to allow for venous return, reduce venous hypertension, and reduce effects of higher hydrostatic pressure.6 If compression stockings do reduce symptomatology in patients, there are different classes of stockings with specific pressures that can be prescribed based upon the level of pressure a given patient can tolerate; however, a thorough examination to determine sufficiency of arterial supply should be performed prior to prescribing compression stockings to avoid vascular complications.6 Some recent research has shown that compression stockings could potentially prolong the time to progression of VVs toward CVI.3,12 Weight loss and elevation of the lower extremity may be helpful in some patients, as well as advice on skin care.5,6,12
Medical Treatment
Certain venoactive or venotrophic drugs have been used to treat VVs when the patient is symptomatic.1,19 The goals of these drugs are to improve capillary permeability and venous tone; however, there is a lack of data to support their use and the exact mechanism of these medications is unknown.1 There is data to show that micronized purified flavonoid fraction (MPFF)10 can reduce symptoms of pain and heaviness in the legs, frequency of leg cramps at night, and great saphenous vein reflux in the evening.10,20 These medications are only used for symptomatic support and do not treat underlying causes of venous reflux.19
Although minimal data exists within the last 5 years, a 2016 article published in the Journal of the American Heart Association indicated that 2 medications, atorvastatin and rosuvastatin, partially inhibited varicose vein development by interfering with proteins involved with stress mediating activity in venous smooth muscle cells.21 The authors also theorized that these medications may also reduce recurrence of VVs after surgical repair of varicosities. In a 2022 paper where researchers were studying the effects of atorvastatin on the venous system, they also found that the anti-inflammatory properties of statins may slow the progression of CVD in general.22 This study referred to other data regarding the relationship between statins and thromboembolism as well as CVI, but noted that additional studies need to be performed with long-term data to determine the full effects of statins on CVD.
Non-surgical Cosmetic Treatment

Sclerotherapy: Sclerotherapy with sclerosing agents and use of ultrasound has been shown to cause vasoconstriction, thrombosis, and occlusion in VVs,3 and has been noted to be the least invasive percutaneous technique for closure of VVs.1 Foam sclerotherapy could be considered in pregnant patients only if a bleeding VV causes transfusions or recurrent hospitalizations.6 Sclerotherapy is usually preferred for smaller and medium sized veins, 1–3 mm, and 3–5 mm respectively, or in the treatment of post-surgical recurrent VVs.5,23
Laser Treatment
 Thermal Ablation with Endovenous Laser Therapy or Radiofrequency Ablation: Ablation therapy uses heat to repair damaged veins. Two key methods, an external laser or an endovenous catheter used in endovenous laser therapy (EVLT) or radiofrequency waves, used in radiofrequency ablation (RFA), use heat to clot and close the vein in order to reroute the flow of blood to competent veins.5,24,25 EVLT, also known as endovenous later ablation (EVLA), has shown benefits such as reduction of damage to surrounding tissues and less downtime for patients who chose this option over surgical treatment.26 External laser ablation works best for telangiectasias, whereas EVLT is more appropriate for larger veins.5 Additional forms of endovenous thermal ablation include steam vein sclerosis (SVS) and endovenous microwave ablation.19
Thermal Ablation with Endovenous Laser Therapy or Radiofrequency Ablation: Ablation therapy uses heat to repair damaged veins. Two key methods, an external laser or an endovenous catheter used in endovenous laser therapy (EVLT) or radiofrequency waves, used in radiofrequency ablation (RFA), use heat to clot and close the vein in order to reroute the flow of blood to competent veins.5,24,25 EVLT, also known as endovenous later ablation (EVLA), has shown benefits such as reduction of damage to surrounding tissues and less downtime for patients who chose this option over surgical treatment.26 External laser ablation works best for telangiectasias, whereas EVLT is more appropriate for larger veins.5 Additional forms of endovenous thermal ablation include steam vein sclerosis (SVS) and endovenous microwave ablation.19
Non-Thermal, Non-Tumescent Ablation Techniques (NTNTs)
Mechanochemical Ablation and Cyanoacrylate Glue: One of the newer forms of treatment involves 2 additional options known as mechanochemical ablation (MOCA) and cyanoacrylate glue (CAG).27 These techniques, however, are not considered first line for VV treatment, due to a lack of long-term studies as well as the lack of indication in the algorithm provided by the National Institute of Clinical Evidence (NICE).27 These options have been successful for pain symptoms and a reduction in injury to surrounding nerves. A comprehensive review of treatments for chronic venous disorder published in 2021 discussed these new techniques, with terms of MOCA and cyanoacrylate embolization (CAE)28 as possibly establishing this technique as a newer novel system in the future for treatment options of venous disease. However, cost may outweigh the benefits of using cyanoacrylate treatment for VVs in today’s economic environment.2,29
Surgical Treatment
Surgical treatment options are dependent on VV location. For example, surgery is the main treatment for greater saphenous varicose veins (GSSV).30 For many years, the standard of treatment for VVs was open surgical therapy,3 with high litigation stripping of the greater saphenous vein, along with removing large VVs; however, due to complications, endovenous ablation therapy has become the more commonly used VVs surgical treatment.1,3 Treatment for VVs today mainly involves the use of venoactive drugs for CEAP levels C0–C2 along with sclerotherapy and endovenous treatment,31,32 although endovenous treatment needs further data for comparison to the surgical approaches.3 In a 5-year trial for different VVs treatments, participants were found to have improved quality of life after surgery or ablation compared to those treated with foam sclerotherapy.33 The authors of this trial did, however, note that long-term effectiveness needed additional evaluation.
Treatment Discussion That May be Covered for Advanced Classification
(C3 and higher)
 As mentioned, VVs are noted at level C2 in the CEAP classification. Conditions rated higher than C2 are related to CVI and treatments may not be covered by insurance due to differences in approval of treatments for higher levels of classification. Many of these treatments are specific for first-line options depending upon the CEAP grade as well as the specific vein location. Therefore, only an overview will be discussed for additional treatment options. Both ambulatory, micro-phlebotomy, and transilluminated power phlebotomy have data indicating benefits of post-procedural evaluations.3 A study published in 2022 noted that patients who underwent subfascial endoscopic perforator surgery (SEPS) along with EVLT had outcomes that showed reduced blood loss, operative time, hospitalization time, and stress response on the body, as well as improved treatment effect.30 Stab phlebotomy, also known as hook phlebectomy, mini-phlebectomy, and ambulatory phlebectomy, was used prior in conjunction with vein stripping or ligation, but currently is used with ablation of the saphenous vein. More advanced surgical techniques such as stent implantation and bypass surgery are typically reserved for patients with advanced CVI who have failed previous interventions.1 Valvuloplasty procedures, where a valve from either the axillary or brachial vein is used for surgical reconstruction of incompetent valves, are also reserved for patients with more advanced disease.1 Earlier referral to a vascular surgeon for VVs, however, should be considered if the patient is at risk for thromboembolism after treatment or if the patient develops severe CVI that would warrant a surgical intervention.6
As mentioned, VVs are noted at level C2 in the CEAP classification. Conditions rated higher than C2 are related to CVI and treatments may not be covered by insurance due to differences in approval of treatments for higher levels of classification. Many of these treatments are specific for first-line options depending upon the CEAP grade as well as the specific vein location. Therefore, only an overview will be discussed for additional treatment options. Both ambulatory, micro-phlebotomy, and transilluminated power phlebotomy have data indicating benefits of post-procedural evaluations.3 A study published in 2022 noted that patients who underwent subfascial endoscopic perforator surgery (SEPS) along with EVLT had outcomes that showed reduced blood loss, operative time, hospitalization time, and stress response on the body, as well as improved treatment effect.30 Stab phlebotomy, also known as hook phlebectomy, mini-phlebectomy, and ambulatory phlebectomy, was used prior in conjunction with vein stripping or ligation, but currently is used with ablation of the saphenous vein. More advanced surgical techniques such as stent implantation and bypass surgery are typically reserved for patients with advanced CVI who have failed previous interventions.1 Valvuloplasty procedures, where a valve from either the axillary or brachial vein is used for surgical reconstruction of incompetent valves, are also reserved for patients with more advanced disease.1 Earlier referral to a vascular surgeon for VVs, however, should be considered if the patient is at risk for thromboembolism after treatment or if the patient develops severe CVI that would warrant a surgical intervention.6
Treatment Options & Complications
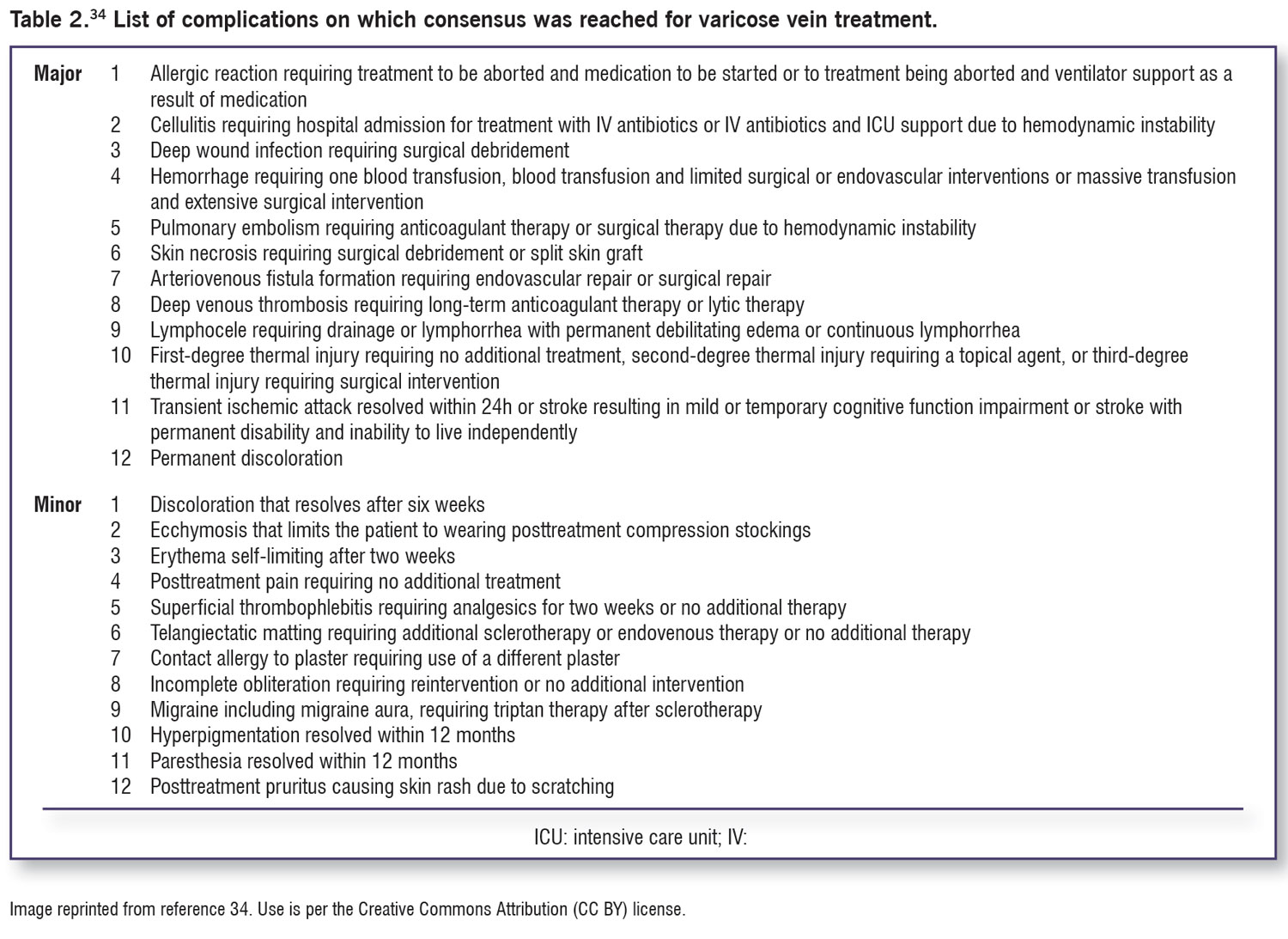
VVs can increase the potential for superficial thrombophlebitis, pain, external hemorrhage, and progressive disease that may include the development of leg ulcers, infection, and other signs of CVI.5,6 Complications of treatments can include recurrence of VVs,6,12 staining of the skin, nerve injury, thrombophlebitis, bleeding, and allergic reactions.6 Weighing the risk/benefit ratio for treatment will be important, as well as discussing costs, particularly if the cost of the chosen procedure is not covered by health insurance. Additional complications of treatments for VVs are noted in Table 2,34 which is a consensus of 43 clinicians that includes 12 major and 12 minor complications that should be communicated to patients who are considering treatments including sclerotherapy, open surgery, and endovascular treatments.
Prevention
Counseling patients to elevate legs and monitor skin for changes should be part of routine communication for prevention of VVs.12 Predisposing factors, such as being overweight or obese, and sedentary lifestyle risks should be communicated with patients to reduce the development of VVs as well as stall the progression time to later-stage CVI.3 In female patients, risks regarding pregnancy and the use of estrogen supplements should be discussed as preventtive measures, particularly if there is a family history of VV.
“Varicose Veins of the Lower Extremities: A Primer Part I” appeared in the August issue of Lower Extremity Review and can be found here: https://lermagazine.com/article/varicose-veins-of-the-lower-extremities-a-primer-part-i
Angela Kelley, PA-C, is Associate Professor and Director of Didactic Education, Physician Assistant Program at Gannon University in Ruskin, Florida, and a Regional Director Health Coach with Optavia (www.optavia.com/us/en/coach/angela).
Suggested Further Readings
Gloviczki P, Lawrence PF, Wasan SM, et al. The 2023 Society for Vascular Surgery, American Venous Forum, and American Vein and Lymphatic Society clinical practice guidelines for the management of varicose veins of the lower extremities. Part II: Endorsed by the Society of Interventional Radiology and the Society for Vascular Medicine. J Vasc Surg Venous Lymphat Disord. 2024 Jan;12(1):101670. doi: 10.1016/j.jvsv.2023.08.011.
This Part II of their guidelines focuses on evidence supporting the prevention and management of varicose veins with compression, drug therapies and nutritional supplements, evaluations of varicose tributaries and superficial venous aneurysms, and management of complications.
Singh A, Gattani R. A Narrative Review of Advancements in Understanding and Treating Varicose Veins. Cureus. 2023 Nov 1;15(11):e48093. doi: 10.7759/cureus.48093.
Varicose veins, marked by the presence of dilated and tortuous subcutaneous vessels, precipitate both physical discomfort and cosmetic concerns, frequently necessitating meticulous clinical evaluation coupled with ultrasound studies to secure a precise diagnosis.
Tan J, Chen Y, Huang J, Xu W. A systematic review of endovenous ablation for the treatment of small saphenous varicose veins. Vasa. 2023 Nov;52(6):355-365. doi: 10.1024/0301-1526/a001091.
This systematic review summarizes the results of existing studies on endovenous ablation for the treatment of small saphenous varicose veins, compares its role and efficacy, and provide insights into the future development of endovenous ablation for treating small saphenous varicose veins.
Fonseca MM, Mocelin FJ, Poltronieri LR, Guimaraes Filho JL. Treatment of varicose veins using the Cryo laser after foam technique. J Vasc Surg Cases Innov Tech. 2024 May 29;10(4):101549. doi: 10.1016/j.jvscit.2024.101549.
Cryo laser after foam sclerotherapy is a procedure to treat reticular veins in the lower extremities that utilizes first foam sclerotherapy with polidocanol then immediately followed by transdermal Nd:YAG 1064 laser treatment and can treat veins ≤5 mm.
- Youn YJ, Lee J. Chronic venous insufficiency and varicose veins of the lower extremities. Korean J Intern Med. 2019;34: 269–283. doi.org/10.3904/kjim.2018.230.
- Ortega MA, Fraile-Martinez O, Garcia-Montero C, et.al. Understanding chronic venous disease: A critical overview of its pathophysiology and medical management. J Clin Med. 2021;10(15):3239. doi: 10.3390/jcm1015323.
- Raffetto JD, Khalil RA. Mechanisms of lower extremity vein dysfunction in chronic venous disease and implications in management of varicose veins. Vessel Plus. 2021;5:36. doi: 1020517/2574–1209.2021.16.
- Trayes KP, Studdiford, JS, Pickle S, Tully AS. Edema: diagnosis and management. Am Fam Phys. 2013;88:102–110.
- Raetz J, Wilson M, Collins K. Varicose veins: diagnosis and treatment. Am Fam Phys. 2019;99(11):682–688.
- Atkins E, Mughal NA, Place F, et al. Varicose veins in primary care. BMJ. 2020;370:m2509. doi.org/10.1136/bmj.m2509.
- Onida S, Lane TR, Davies AH. Improving the management of varicose veins. Practitioner. 2013 Nov-Dec;257(1766):21-4, 2–3.
- Pollack AA, Taylor BE, et al. The effect of exercise and body position on the venous pressure at the ankle in patients having venous valvular defects. J Clin Invest. 1949;28(3):559–63.
- Shadrina AS, Sharapov SZ, Shashkova TI, Tsepilov YA. Varicose veins of the lower extremities: Insights from the first large-scale genetic study. PLOS Genet. 2019;15(4): e1008110. PMID: 30998689. doi: 10.1371/journal.pgen.1008110.
- Davies AH. The seriousness of chronic venous disease: A review of real-world evidence. Adv Ther. 2019;36(Suppl 1):S5-S12. doi.org.10.1007s12325-019-0881-7.
- Raffetto JD, Ligi D, Maniscalco R, et al. Why venous leg ulcers have difficulty healing: Overview on pathophysiology, clinical consequences, and treatment. J Clin Med. 2021;10(1)29. doi.org/10.3390/jcm10010029.
- Lumley E, Phillips P, Aber A, et al. Experiences of living with varicose veins: A systematic review of qualitative research. J Clin Nurs. 201928(7-8):1085-1099. doi: 10.1111/jocn14720.
- Racette S, Sauvageau A. Unusual sudden death: two case reports of hemorrhage by rupture of varicose veins. Am J Forensic Med Pathol. 2005;26(3):294–296. doi: 10.1097/01.paf.0000176283.19127.0e.
- Sudoł-Szopi´nska I, Bogdan A, Szopinski T, Panorska AK, Kołodziejczak M. Prevalence of chronic venous disorders among employees working in prolonged sitting and standing postures. Int. J Occup Saf Ergon. 2011;17(2):165–173. doi: 10.1080/10803548.2011.11076887.
- Sharma S, Vashist M, Vashist MG. Family history as major predisposing factor in varicose veins disorder. Eur J Biomed Pharm Sci. 2017;4(12):392–396.
- 16. Vlajinac HD, Radak DJ, Marinkovi´c JM, Maksimovi´c MŽ. Risk factors for chronic venous disease. Phlebology 2012,27, 416–422. doi.org/10.1258/phleb.2011.011091.
- Gloviczki P, Comerota AJ, Dalsing MC, et al. The care of patients with varicose veins and associated chronic venous diseases: clinical practice guidelines of the Society for Vascular Surgery and the American Venous Forum. J Vasc Surg. 2011;53(5 suppl):2S–48S. doi.org/10.1016/j.jvs.2011.01.079
- National Institute for Health and Care Excellence. Varicose veins: diagnosis and management. Clinical guideline 168. July 2013. https://www.nice.org.uk/guidance/cg168. Accessed May 21, 2018.
- Whiteley MS. Current best practice in the management of varicose veins. Clin Cosmet Investig Dermatol. 2022; 15: 567–583. doi.org/10.2147/CCID.S294990.
- Tsukanov YT, Tsukanov AY. Diagnosis and treatment of situational great saphenous vein reflux in daily medical practice. Phlebolymphology. 2017;24(3):144–151.
- Eschrich J, Meyer R, Kuk H, et.al. Varicose Remodeling of Veins Is Suppressed by 3-Hydroxy-3-Methylglutaryl Coenzyme A Reductase Inhibitors. J Am Heart Assoc. 2016 Feb 23;5(2):e002405. doi: 10.1161/JAHA.115.002405.
- Matei SC. Statins – From Lipid-Lowering Benefits to Pleiotropic Effects. Statins Effects on Venous Wall in Patients with Chronic Venous Disease. Intech Opening.2023. doi: 10.5772/intechopen.1001303.
- Tisi PV, Beverley C, Rees A. Injection sclerotherapy for varicose veins. Cochrane Database Syst Rev. 2006(4):CD001732.
- Reichert D. Evaluation of the long-pulse dye laser for the treatment of leg telangiectasias. Dermatol Surg. 1998;24(7):737–740.
- Paravastu SC, Horne M, Dodd PD. Endovenous ablation therapy (laser or radiofrequency) or foam sclerotherapy versus conventional surgical repair for short saphenous varicose veins. Cochrane Database Syst Rev. 2016(11):CD010878.
- Kremastoptis J, Jfri A, Litvinov IV. Treatment modalities for varicose veins of lower extremities. J Cutan Med Surg. 2020. 24(2) 203-204. doi: 10.1177/1203475419891082.
- Chan SJ, Chan YC, Walsh SR, et.al. Endovenous cyanoacrylate ablation for chronic venous insufficiency and varicose veins among Asians. Ann Acad Med Singap. 50 (3). 2021. doi.annals.edu.sg
- Chaitidis N, Kokkinidis DG, Papadopoulou Z, et.al. Treatment of chronic venous disorder: A comprehensive review. Dermatol Ther. 2022;35:e15238. 1–15. doi.org/10.1111/dth.15238.
- Cavezzi,A. Medicine and Phlebolymphology: Time to Change? J.Clin.Med.2020,9,4091.
- Wang, L. Du, J., Zhang, H. Study of Subendoscopic Perforator Surgery Combined with Endovenous Laser Treatment in the Treatment of Great Saphenous Varicose Veins. J. Healthc. Eng. 2022. doi.10.1155/2022/1801099.
- Mansilha, A. Early stages of chronic venous disease: medical treatment alone or in addition to endovenous treatments. Adv Ther. 2020 37:S13-S18. doi.org/10.1007/s12325-019-01217-9.
- Nicolaides A, Kakkos S, Baekgaard N, et al. Management of chronic venous disorders of the lower limbs. Guidelines according to scientific evidence. Part I. Int Angiol. 2018;37(3):181–254. doi: 10.23736/S0392-9590.18.03999-8
- Brittenden J, Cooper D, Dimitrova M, et.al. Five-year outcomes of a randomized trial of treatments for varicose veins. N Engl J of Med. 2019. 381:10. 912–922. doi: 10.1056/NEJMoa1805186.
- deMik SML, Stubenrouch FE, Legemate DA, et.al. Treatment of varicose veins, international consensus on which major complications to discuss with the patient: A Delphi study. Phlebology. 2018. 34(3) 201–207. doi: 10.1177/0268355518785482.






Advancements in vein reduction have made it easier than ever to treat unwanted veins safely. Whether it’s for cosmetic reasons or health concerns, having access to the right treatments can make a real difference in overall vascular health