 By Bijan Najafi, PHD, MSc
By Bijan Najafi, PHD, MSc
The current model for managing diabetic foot syndrome is characterized as reactive and fragmented, contributing to a global crisis where a limb is lost to amputation every 20 seconds. Dr. Bijan Najafi, a bioengineer and research director at UCLA Center for Advanced Surgical and Interventional Technology (CASIT), says that “we can’t manage what we can’t measure,” advocating for a shift toward decentralized, proactive care facilitated by digital health technologies.
Key takeaways from the analysis of remote patient monitoring (RPM) and intervention tools include:
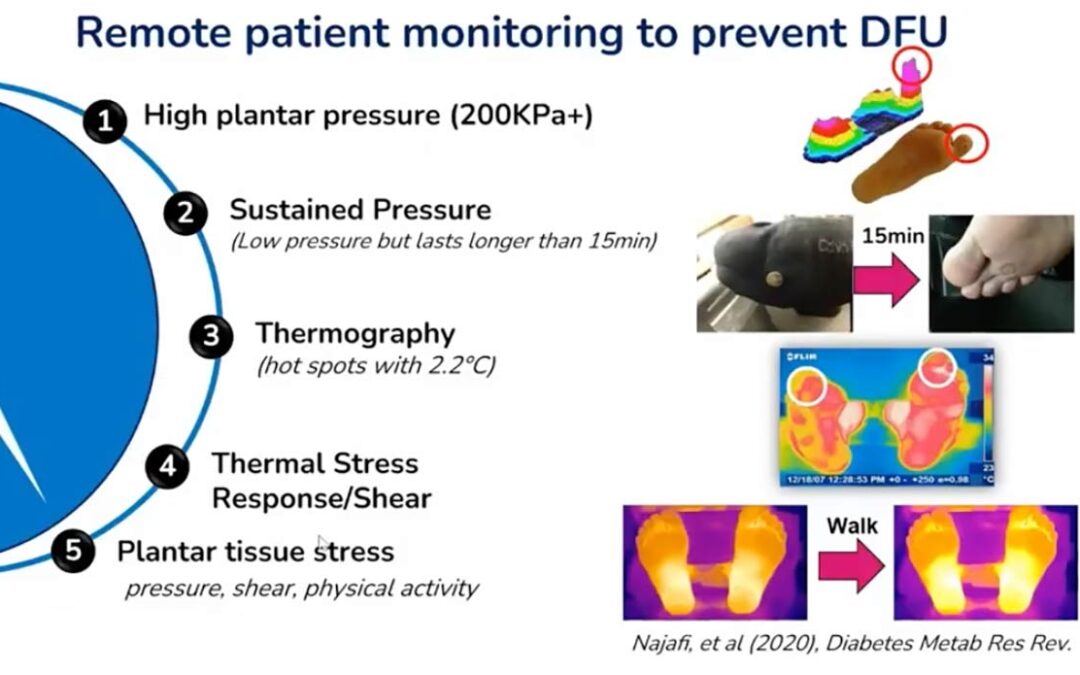
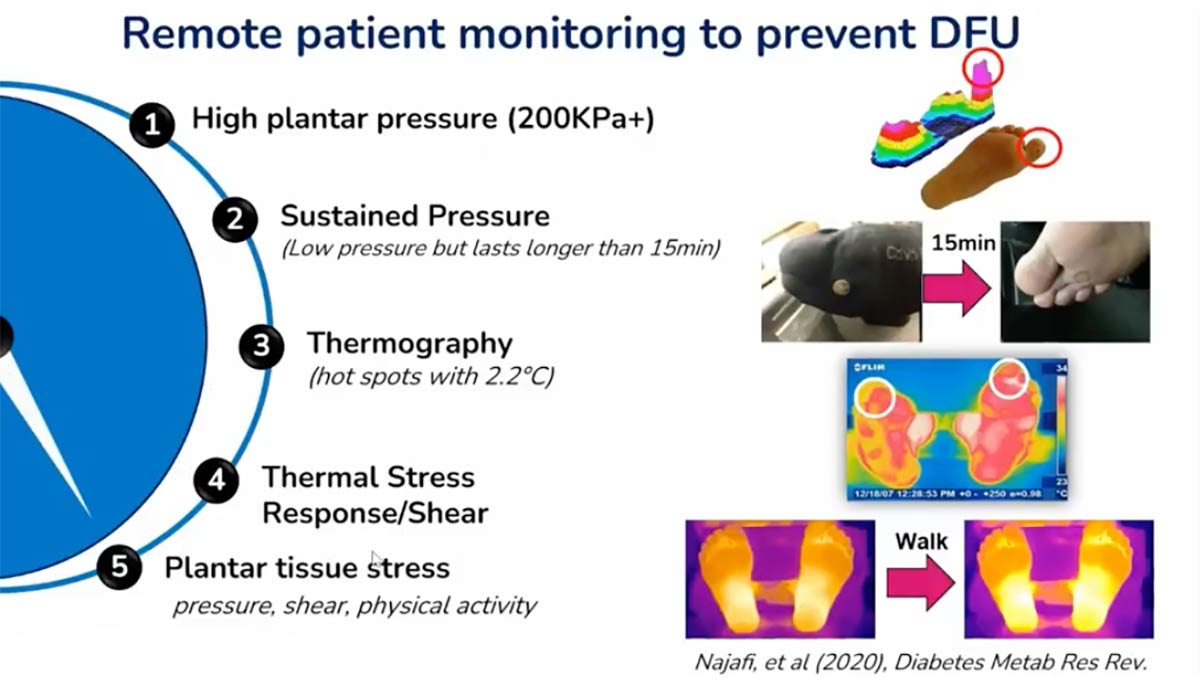
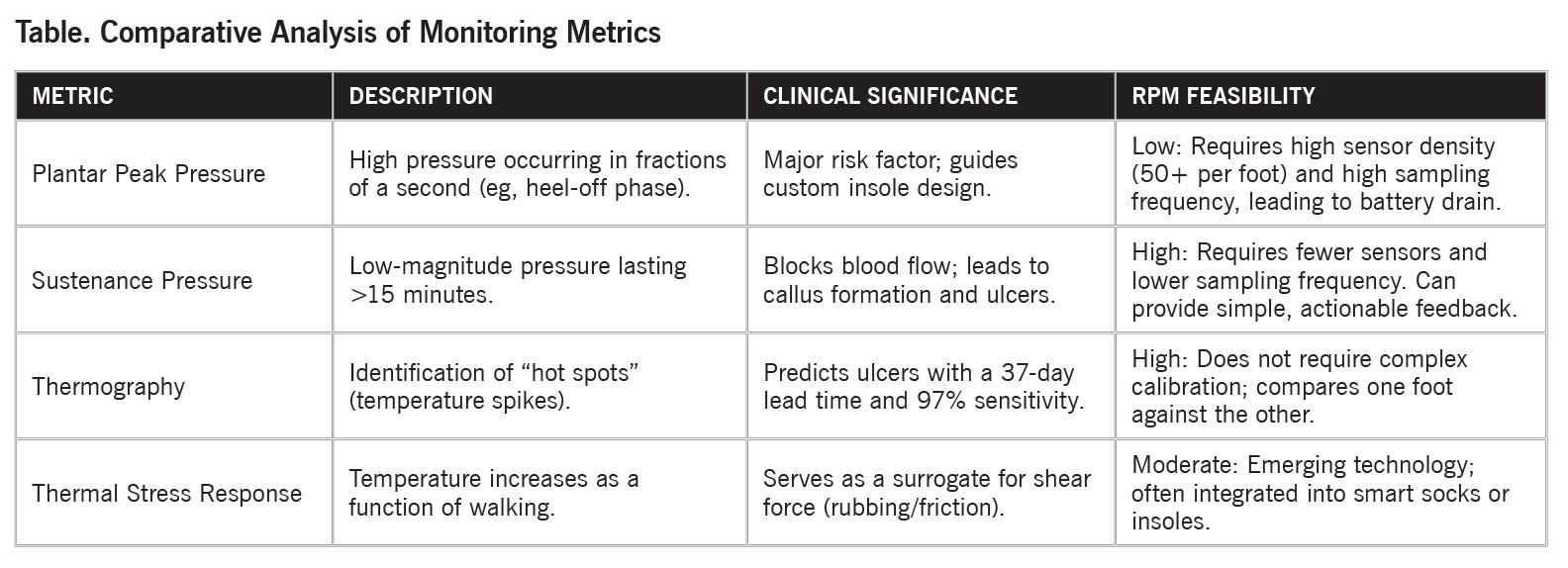
- Measurement Metrics: Critical factors for ulcer prediction include plantar peak pressure (eg, pressures exceeding ~200 kPa), sustenance pressure (prolonged low-magnitude pressure lasting longer than 15–20 minutes, similar to loading conditions associated with pressure ulcer development), and thermography (identifying inflammation “hot spots”).
- Technological Shift: While peak pressure measurement remains difficult to implement remotely due to technical constraints (high sensor density and battery drain), sustenance pressure and temperature monitoring offer more practical pathways for RPM.
- Patient Engagement: Data collection alone is insufficient. Successful prevention requires patient empowerment through actionable, easy-to-understand feedback. Studies indicate that timely and appropriately delivered alerts (eg, periodic notifications such as every 2 hours) can improve adherence to monitoring technologies without necessarily increasing alert fatigue, when designed carefully.
- Smart Offloading: The integration of sensors into offloading devices (smart boots) significantly improves patient compliance and wound healing rates compared to standard removable cast walkers.
- AI Integration: Artificial intelligence and chatbots serve as 24/7 companions, bridging the gap between clinical visits by providing personalized education, mood support, and timely behavioral reminders.
 The Crisis in Diabetic Foot Care
The Crisis in Diabetic Foot Care
The burden of diabetic foot ulcers (DFUs) remains high despite clinical progress. The primary challenges identified are:
- Reactive Care: Clinicians often wait for visible signs of ulceration, which frequently results in interventions occurring too late to prevent amputation.
- Access Gaps: Proximity to specialized care is a predictor of outcomes. Patients living 50 miles or more from an experienced hospital face a significantly higher likelihood of limb amputation.
- Information Retention: Patients typically forget 40% to 80% of the information discussed during a doctor’s visit, leading to poor adherence to home-care protocols.
Remote Patient Monitoring: Metrics and Technology
Effective prevention relies on identifying tissue stress before skin breakdown occurs. The following table outlines the primary metrics used in digital monitoring:
Limitations of Current RPM Tools
While smart mats and sensors are effective, they face specific hurdles:
- Specificity Issues: Some smart mats have a high false-alert rate (specificity as low as 57%), though some argue these alerts help maintain patient engagement.
- Context Deficiency: Many tools measure temperature or pressure without recording physical activity (step counts), making it difficult to determine if a temperature spike is due to inflammation or recent exercise.
 Enhancing Patient Engagement and Compliance:
Enhancing Patient Engagement and Compliance:
Overcoming Alert Fatigue
Research contradicts the assumption that frequent digital alerts lead to patient disengagement.
- Frequency: Patients receiving at least 1 alert every 2 hours demonstrated higher engagement and better response rates over a 3-month period than those receiving fewer alerts.
- Perception: Frequent, comprehensive alerts reassure patients that the technology is actively working for them. Conversely, a lack of alerts often leads patients to assume the device is non-functional, resulting in them stopping use.
The Impact of Smart Offloading
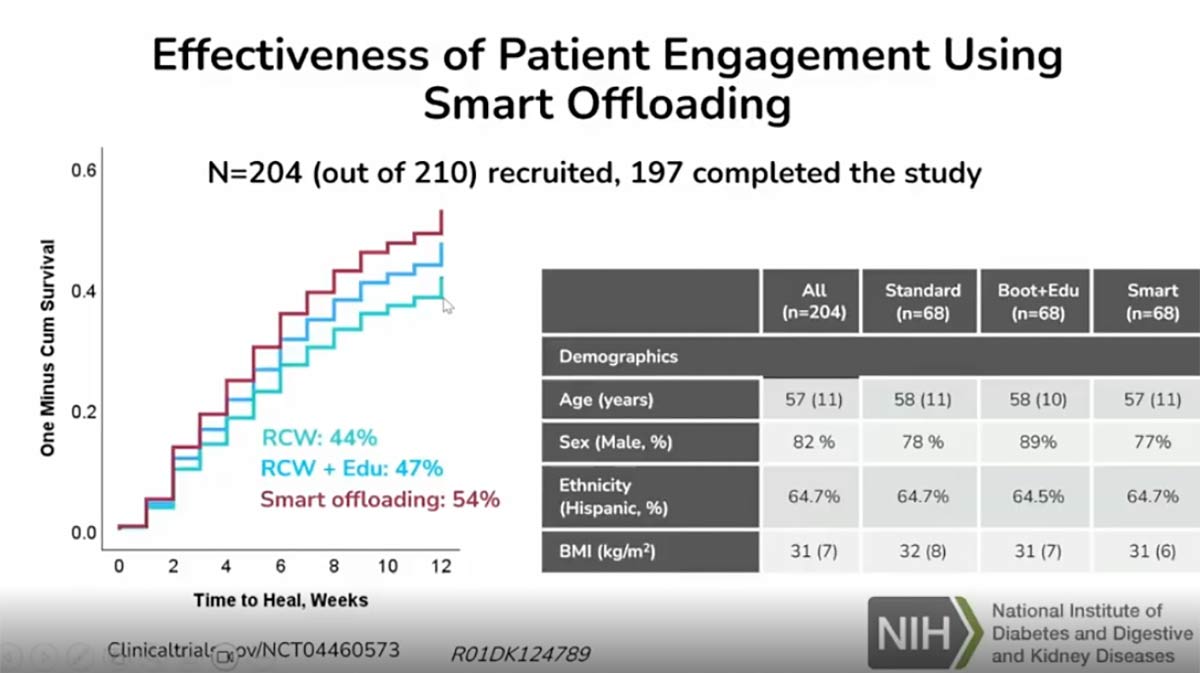
Offloading is the most critical intervention for healing DFUs, yet compliance with removable cast walkers is notoriously low. A study comparing standard walkers, education-reinforced walkers, and smart boots (equipped with accelerometers) revealed:
- Healing Rates: The smart boot group achieved a 23% increase in successful wound healing over 12 weeks compared to the standard cast walker group.
- Retention: Patients using smart boots showed higher resiliency and lower dropout rates. The technology—utilizing simple feedback like “happy” and “sad” faces on a smartwatch—improved the patient’s perception of the treatment’s importance.
The Role of Artificial Intelligence and Data Visualization:
AI Chatbots as Care Extensions
AI-driven chatbots address the fragmented nature of care by acting as a 24/7 companion.
- Behavioral Prompts: AI can detect when a patient is not wearing their offloading boot and send personalized, tone-specific reminders (eg, action-oriented or encouraging messages).
- Education and Support: Unlike generic AI, these tools provide validated, personalized information and mental health support, helping patients manage the frustration and mobility limitations associated with DFU treatment.
 Clinical Decision Support
Clinical Decision Support
To prevent clinician overwhelm, complex sensor data is synthesized into simplified visualizations.
- Normalized Metrics: Various data points (age, compliance, weakness, gait) are converted to a 0–10 scale.
- Visual Triage: Using “green” (healthy) and “red” (unhealthy) benchmarks allows clinicians to quickly identify which specific risk factors are impeding a patient’s healing process, facilitating personalized adjustments to care plans.
The integration of digital tools—from smart insoles to AI companions—represents a fundamental shift toward a proactive healthcare framework. By empowering patients with real-time data and bridging the gap between clinical visits with intelligent monitoring, these technologies aim to significantly reduce the incidence of diabetic-related amputations over the next decade. Success in this field requires continued collaboration between engineers and clinicians to ensure these tools are both scalable and medically sound.
Dr. Najafi is a dedicated professional in digital health, committed to advancing healthcare equity through decentralized models. As co-founder and leader of NSF IUCRC C2SHIP, he has brought together academic institutes, community health organizations, and industrial partners to support a care-in-place model, empowered by digital technologies. This program has received recognition from the National Science Foundation and Industry-University Research Partnerships program.
As a professor at UCLA and Research Director of founder of Center for Advanced Surgical & Interventional Technology (CASIT), he and his team have pioneered the use of wearable sensors, mobile health platforms, and AI to transform patient care beyond the clinic. Their innovative work emphasizes continuous monitoring of chronic conditions, fall prevention, and personalized care solutions that empower patients and support caregivers. By integrating cutting-edge technology with healthcare, his goal is to make care more accessible, proactive, and personalized, ultimately improving health outcomes and quality of life for older adults and individuals with chronic illnesses. Dr. Najafi is a strong advocate for diversity and inclusion in digital health research and has mentored over 300 junior researchers. He has received numerous awards and recognition, including being listed as one of the most Influential Health and Medical Leaders and among the top 1% of scholars worldwide in the field. With 200+ scientific publications, 20 patents, and 80+ grants totaling over $100 million, he brings extensive knowledge and experience to the table. His editorial and advisory roles, co-founding of a successful startup, and successful commercialization of various remote patient monitoring technologies showcase his ability to conduct creative research, manage grants and teams, and provide scientific and administrative leadership.
This article is a summary of Dr. Najafi’s presentation, “Digital Solutions for Early Detection, Prevention and Personalized Treatment” from the Diabetes Technology and Prevention Summit November 15, 2025. To view the full presentation with questions and answers—and see the agenda for the program, visit https://diabetestech.lerexpo.com/ . Continuing education credits are available for this and many of the lerEXPO programs.





