 Excess body weight is considered by many experts to be the primary modifiable etiological factor in knee osteoarthritis (OA) development. However, the relationship among body mass index (BMI), the anatomical manifestations of knee OA, and knee pain is not clear-cut.
Excess body weight is considered by many experts to be the primary modifiable etiological factor in knee osteoarthritis (OA) development. However, the relationship among body mass index (BMI), the anatomical manifestations of knee OA, and knee pain is not clear-cut.
By Elizabeth Weiss, PhD
Knee pain affects one in 10 US adults older than 65 years.1 The most common cause of knee pain in adults is osteoarthritis (OA); it has been estimated that one in four adults has knee OA.2-3 The physical manifestations of OA include joint space narrowing, cartilage hardening and thickening, tears or lesions in cartilage, and formation of osteophytes. Although OA is common, especially as one ages, the age at which one develops knee OA and the of severity symptoms, which include pain and stiffening, depend on a variety of etiological factors, such as genetics,4 activity levels,5 anatomical variations,6 and body weight.7-9
Excess body weight is considered the primary modifiable etiological factor in knee OA development.7-8,10-11 Body mass index (BMI), which is calculated as weight/height2 (kg/m2), is the variable used most frequently to assess the effects of excess weight on knee OA. Studies from around the world have found an increase in BMI correlates with both knee OA anatomical manifestations (or traits) and pain; evidence of the relationship between BMI and knee OA has been found in populations from Norway,12 Vietnam,13 India,14 Australia,15 the UK,16 the US,9 France,17 the Netherlands,18 Lebanon,19 and the Philippines.20 Knee OA occurs about seven times more frequently in obese individuals than in nonobese individuals.21 In a sample of 3769 UK adults aged 50 years and older, Jinks et al16 found that risk of knee OA pain in obese individuals was more than double the risk in normal-weight individuals.

Obesity is the leading cause of the increase in knee replacement surgery. Incidence of knee replacement surgery increased eightfold between 1979 and 2002 in the US, and tripled between 1991 and 2006 in the UK.3 Liu et al’s clinical paper22 reported that in the UK, 69% of knee replacements in middle-aged women can be attributed to obesity. However, the relationship among BMI, knee OA traits, and knee OA pain is not clear-cut. Figure 1 illustrates the complex relationship between knee OA, pain, and excess body mass.
Pain and BMI
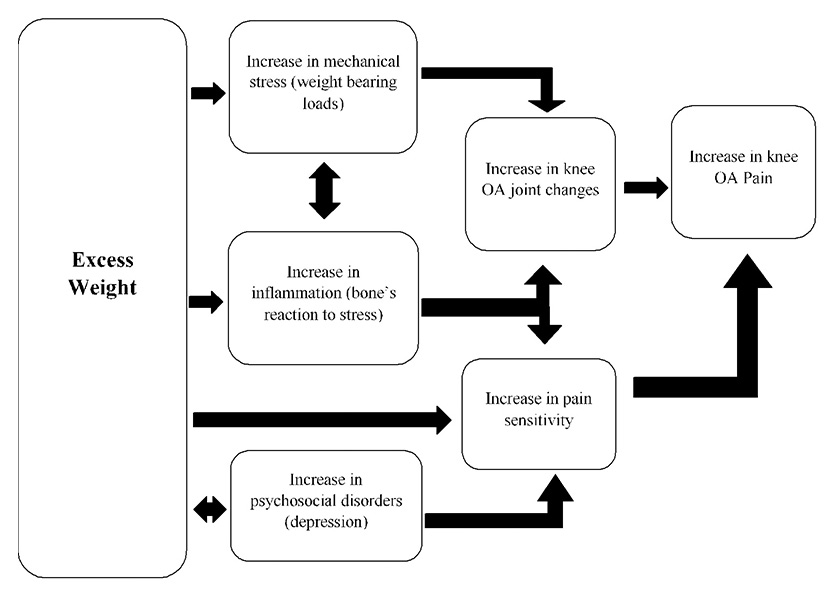
Figure 1. This chart illustates the different ways in which excess weight may affect knee OA pain.
Lee et al7 found a correlation between BMI and pain related to knee OA that has occurred within the last seven days; they also discovered that an increase in BMI was the primary variable in determining activity levels. Research suggests increasing activity level, especially among inactive individuals, alleviates knee pain and reduces the risk of disability from knee OA.7,23 The most common pain survey used in knee OA research is the WOMAC (Western Ontario and McMaster Universities Arthritis Index) pain subscale.24 The WOMAC scale includes questions regarding pain during everyday tasks (such as getting in and out of a car, putting on socks, going shopping, getting out of the bathtub, and getting on or off the toilet) and general motions (such as twisting/pivoting, straightening the knee fully, bending the knee fully, walking on a flat surface, going up or down stairs, lying or sitting, and standing).
Laberge et al25 assessed more than 100 individuals aged between 45 and 55 years for BMI, knee OA risk, and pain as measured through WOMAC self-reports; their results showed that higher BMI was associated with a greater risk of knee pain. Garver et al26 pointed out that, among a small sample of 174 individuals assessed using the WOMAC pain subscale, those in obesity class III (BMI, 40 or higher) had average pain scores twice as high as normal-weight indivduals (BMI, 18.5-24.9). In an Australian sample of more than 1000 individuals, Ackerman and Osborne15 found obese individuals had seven times higher odds of having diagnosed knee OA than normal-weight individuals; they also found that obesity was associated with higher levels of knee OA pain and stiffness. A study from India of 100 women found that 65% were obese and that 94% of the obese patients developed symptoms of knee OA pain and stiffness.14 And, in Lebanon, using a sample of 59 patients with symptomatic knee OA and 118 controls, El Ayoubi et al19 also found obesity was a significant risk factor for symptomatic knee OA.
Some authors have argued that obesity itself intensifies pain and, thus, the increased risk of knee OA pain associated with obesity is not necessarily related to the physical characteristics of OA.27,28 For instance, Guermazi et al,29 using a sample of more than 700 individuals from the Framingham Osteoarthritis Study cohort, found that 86% of patients with no knee OA pain had joint changes indicative of knee OA. Although, as mentioned above, Nguyen et al3 reported a surge in knee replacement surgery as a result of an increase in knee OA pain, there has not been a concomitant rise in radiographic evidence of knee OA. Riddle and Stratford30 looked at a sample of more than 3000 community-dwelling individuals aged between 50 and 79 years. They found an increase in BMI raised the risk of bilateral knee pain as measured with the WOMAC pain subscale, even in individuals with minimal or no x-ray evidence of OA as measured by the Kellgren and Lawrence scale.31 Riddle and Stratford30 also found that individuals who reported widespread pain symptoms had higher BMIs than those who did not report widespread pain.
Some researchers, such as Rogers and Wilder32 and Holla et al,18 have suggested knee pain in obese individuals is in part a result of depression. Rogers and Wilder’s study32 of 575 individuals with radiographic knee OA found that knee OA pain was less likely in normal-weight individuals than in obese individuals. After adjusting for knee OA severity, the odds of knee pain were nearly twice as high in overweight (BMI, 25-29.9) and obese (BMI, 30-34.9) individuals as in normal-weight individuals (BMI, 18.5-24.9), and 7.5 times as high in individuals with BMIs greater than 40 as in normal-weight individuals.32
Physical evidence of knee OA and BMI
High BMI is associated with increased knee OA trait severity as well, and studies have found knee OA traits correlate with pain. Ballegaard,33 for example, found that pain increased with knee inflammation as seen on dynamic magnetic resonance imaging (MRI). MRI seems to be more diagnostic than x-rays; plain radiographs can miss OA traits and, thus, lead researchers to conclude that pain symptoms are not the result of physical joint changes.33-35 Ho-Pham et al13 found that self-reported knee pain was significantly associated with radiographic knee OA, and that elevated BMI was also associated with a higher risk of radiographic knee OA.
In my own research, using the Osteoarthritis Initiative public-use database with a sample of 4769 individuals, I found that knee pain does correspond to physical joint changes, but that, even when controlling for the Kellgren-Lawrence severity of OA, individuals with higher BMIs experience higher levels of pain (assessed using the WOMAC pain subscale) than those with lower BMIs.9 Garver et al26 too found that individuals in the highest BMI class had significantly more pain and poorer function than those with lower BMIs, even after controlling for radiographic OA severity. Other researchers have found that knee OA pain may be multifactorial, and could involve psychosocial,18,36 inflammatory,11,37,38 and mechanical factors.36,39
Inflammation and mechanical etiologies
Obesity more than triples the risk of infection after knee replacement surgery.38 Researchers who study the biochemicals active during bone healing, such as the hormone leptin that resides in adipocytes (fat cells), suggest that inflammation rather than weight bearing is the source of the association between OA and obesity.40-42 Individuals with high BMIs have excess leptin, which modulates with inflammatory state. Chronic low levels of inflammation are correlated with obesity.44 Dumond et al40 discovered an overexpression of leptin in the synovial fluid and cartilage of individuals with knee OA, and a significant correlation between BMI and leptin concentrations in synovial fluid.
 Furthermore, a review of the research has pointed out that hand OA correlates with BMI, which provides corroboration for the inflammatory response theory.41 In a sample of 95 obese patients with knee OA, Ballegaard33 found a correlation between knee pain and inflammation. Both Miller et al,37 using a sample of 87 obese individuals with OA knee pain, and Messier et al,11 using a sample of 388 overweight and obese individuals with OA, found inflammation, as assessed through blood analysis, and knee OA pain decreased with weight loss.
Furthermore, a review of the research has pointed out that hand OA correlates with BMI, which provides corroboration for the inflammatory response theory.41 In a sample of 95 obese patients with knee OA, Ballegaard33 found a correlation between knee pain and inflammation. Both Miller et al,37 using a sample of 87 obese individuals with OA knee pain, and Messier et al,11 using a sample of 388 overweight and obese individuals with OA, found inflammation, as assessed through blood analysis, and knee OA pain decreased with weight loss.
Other researchers have argued that mechanical factors should not be ruled out as a possible cause of the association between BMI and knee OA pain.10,36,39,44,46 Mechanical stress can result in the induction of inflammatory factors, which can contribute to pain.47 Even the National Institutes of Health’s MedlinePlus webpage on osteoarthritis notes, “Being overweight increases the risk of OA in the hip, knee, ankle, and foot joints. This is because extra weight causes more wear and tear.”45
Large sample data have supported the mechanical etiology of knee OA.48,49 Using a national database sample of 2597 individuals, a study of BMI and activity found that those who were at greatest risk of knee OA were individuals with high BMIs, particularly those who engaged in physical activities that involved lifting.48 Toivanen et al,49 with a sample of 8000 individuals, also found that the risk of developing knee OA was strongly associated with BMI and heavy physical work load.
A conundrum that spans both the inflammatory and mechanical etiologies is the sex difference reported in most studies. Women are more likely than men to have knee OA pain.9,13,50,51 The sex difference is also seen in radiographic evidence of knee OA, which demonstrates that women have more of the physical joint changes seen on x-ray than men.44 Some studies have suggested the higher rate of knee OA in women is related to the greater impact of obesity on women compared with men. Wills et al51 point out in their large study of more than 3000 individuals that there is a stronger relationship between BMI and knee OA risk in women than in men. Elbaz et al44 also found that BMI negatively affected knee OA pain in women to a greater degree than in men. In addition, weight loss seems to positively affect women more than men. When examining the effects of obesity and OA pain in more than 6000 individuals over a six-year period, Peltonen et al8 found women had greater knee pain relief after weight loss surgery than men.
However, some studies suggest that sex differences in OA pain are driven by factors other than obesity and weight bearing. Ho-Pham et al13 did not find that obesity explained the sex difference in knee OA pain. In a conference paper, I presented preliminary sex difference results on OA in nonweight-bearing and weight-bearing joints using data from the National Institutes of Health Osteoarthritis Initiative; I found that, in men, higher BMIs were associated with weight-bearing joints only, but, in women, BMI correlated with nonweight-bearing joints as well as weight-bearing joints.52 Researchers studying rodents have found that female animals displayed more pain sensitivity from inflammation than male animals.53,54
One way to assess whether mechanical stresses affect both knee OA traits and pain in relation to excess body weight is to look at whether the weight-bearing components of the knee are more affected by BMI than nonweight-bearing components of the knee. It appears the medial compartment of the knee joint, which bears the vast majority of the weight, is affected more by obesity than the lateral compartment.39 In a comparative study with x-rays from Beijing, China, and Framingham, MA, Felson et al39 reported that Chinese patients had greater frequencies of lateral (nonweight-bearing) knee OA than Caucasian patients, while the opposite trend occurred on the medial (weight-bearing) side; this difference may be because the Caucasian patients were heavier than the Chinese patients, but Felson et al wrote that adjustments for BMI differences did not erase the population differences. Thompson et al,55 however, used Osteoarthritis Initiative data and found BMI was associated with an increased risk of localized, regional, and diffuse knee OA pain, but that elevated BMI had the strongest relationship with diffuse pain, which is less likely to involve weight-bearing structures.

Reducing knee OA pain
Knee OA, which affects more than 30% of adults, is not reversible and worsens over time. There may be ways to reduce the painful effects, however.26 Regardless of which etiological factors have the greatest effect on knee OA, a reduction in excess body weight is the primary trait that can be modified to reduce knee OA pain.7,9,10 Weight reduction in patients with knee OA reduces pain and increases mobility.15,26 Researchers have found that weight loss from diet and exercise alleviates knee OA pain and reduces inflammation.11
Efforts to reduce the risk of knee OA should begin by assuring that children and young adults maintain a healthy BMI; researchers have found that, even in children as young as 11 years, excess weight can create a predisposition for knee OA.51,55 When excess weight makes exercise difficult, weight loss may be more easily achieved through small dietary changes (eg, drinking water instead of a sugared drink). Overweight or obese patients who are considering knee replacement surgery should first attempt weight loss, which will decrease the risk of infection after surgery and may reduce knee pain to a level that would render surgery unnecessary.3,22,38 Finally, obese individuals may have other pain symptoms; if a patient has widespread pain, psychosocial factors may need to be investigated as possible root causes.18,32,36
Elizabeth Weiss, PhD, is a professor of anthropology at San Jose State University in California. Her research expertise lies in etiological explorations of bone health and disease from past and present populations to better reconstruct quality of life.
- Felson DT. The epidemiology of knee osteoarthritis: results from the Framingham Osteoarthritis Study. Semin Arthritis Rheum 1990;20(3 Suppl 1):42-50.
- Losina E, Walensky RP, Reichmann WM, et al. Impact of obesity and knee osteoarthritis on morbidity and mortality in older Americans. Ann Intern Med 2011;154(4):217-226.
- Nguyen U, Yuqing Z, Yanyan Z, et al. Increasing prevalence of knee pain and symptomatic knee osteoarthritis: survey and cohort data. Ann Intern Med 2011;155(11):725-732.
- Spector TD, MacGregor AJ. Risk factors for osteoarthritis: genetics. Osteoarthritis Cartilage 2004;12(Suppl A):S39-S44.
- Guilak F. Biomechanical factors in osteoarthritis. Best Pract Res Clin Rheumatol 2011;25(6):815-823.
- Hunter DJ, Niu J, Zhang Y, et al. Knee height, knee pain, and knee osteoarthritis: The Beijing Osteoarthritis Study. Arthritis Rheum 2005;52(5):1418-1423.
- Lee J, Song J, Hootman JM, et al. Obesity and other modifiable factors for physical inactivity measured by accelerometer in adults with knee osteoarthritis: data from the Osteoarthritis Initiative (OAI). Arthritis Care Res 2013;65(1):53-61.
- Peltonen M, Lindroos A, Torgerson J. Musculoskeletal pain in the obese: a comparison with a general population and long-term changes after conventional and surgical obesity treatment. Pain 2003;104(3):549-557.
- Weiss E. Knee osteoarthritis, body mass index and pain: data from the Osteoarthritis Initiative. Rheumatology 2014 Jun 17. [Epub ahead of print]
- King LK, March L, Anandacoomarasamy A. Obesity and osteoarthritis. Indian J Med Res 2013;138(2):185-193.
- Messier SP, Mihalko SL, Legault C, et al. Effects of intensive diet and exercise on knee joint loads, inflammation, and clinical outcomes among overweight and obese adults with knee osteoarthritis: the IDEA randomized clinical JAMA 2013;310(12):1263-1273.
- Mork PJ, Holtermann A, Nilsen TIL. Effect of body mass index and physical exercise on risk of knee and hip osteoarthritis: longitudinal data from the Norwegian HUNT Study. J Epidemiol Community Health 2012;66:678e683.
- Ho-Pham LT, Lai TQ, Mai LD, et al. Prevalence of radiographic osteoarthritis of the knee and its relationship to self- reported pain. PLoS One 2014;9(4):e94563.
- Chavadaki RH, Neelkanta S. Association of obesity with osteoarthritis of knee joint in females. J Evolution Medical Dental Sci 2013;2(38):7272-7276.
- Ackerman IN, Osborne RH. Obesity and increased burden of hip and knee joint disease in Australia: Results from a national survey. BMC Musculoskelet Disord 2012;13:254
- Jinks C, Jordan K, Croft P. Disabling knee pain – another consequence of obesity: Results from a prospective cohort study. BMC Public Health 2006;6:258
- Forestier R, Francon A, Briole V, et al. Prevalence of generalized osteoarthritis in a population with knee osteoarthritis. Joint Bone Spine 2011;78(3):275-278.
- Holla JF, van der Leeden M, Knol DL. The association of body-mass index and depressed mood with knee pain and activity limitations in knee osteoarthritis: results from the Amsterdam osteoarthritis cohort. BMC Musculoskeletal Disord 2013;14:296.
- El Ayoubi N, Chaaya M, Mahfoud Z, et al. Risk factors for incident symptomatic knee osteoarthritis: a population-based case control study in Lebanon. Int J Rheum Dis 2013;16(2):211-218.
- Penserga EG, Tanque AAG. Predictors of disability among Filipinos with knee osteoarthritis. Int J Rheum Dis 2008;11(3):251-256.
- Coggon D, Reading I, Croft P, et al. Knee osteoarthritis and obesity. Int J Obes Relat Metab Disord 2001;25(5):622-627.
- Liu B, Banks E, Cooper C, et al. Relationship of height, weight, and body mass index to the risk of hip and knee replacements in middle-aged women. Rheumatology 2007;46(5):861-867.
- Deyle GD, Henderson NE, Matekel RL, et al. Effectiveness of manual physical therapy and exercise in osteoarthritis of the knee. A randomized, controlled trial. Ann Intern Med 2000;132(3):173-181.
- Bellamy N, Buchanan WW, Goldsmith CH, et al. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol 1988;15(12):1833-1840.
- Laberge MA, Baum T, Virayavanich W, et al. Obesity increases the prevalence and severity of focal knee abnormalities diagnosed using 3T MRI in middle-aged subjects–data from the Osteoarthritis Initiative. Skeletal Radiol 2012;41(6):633-641.
- Garver MJ, Focht BC, Dials J, et al. Weight status and differences in mobility performance, pain symptoms, and physical activity in older, knee osteoarthritis patients. Arthritis 2014;2014:375909.
- Bliddal H, Christensen R. The management of osteoarthritis in the obese patient: practical considerations and guidelines for therapy. Obes Rev 2006;7(4):323-331.
- Janke E, Collins A, Kozak A. Overview of the relationship between pain and obesity: What do we know? Where do we go next? J Rehabil Res Dev 2007;44(2):245-261.
- Guermazi A, Niu J, Hayashi D, et al. Prevalence of abnormalities in knees detected by MRI in adults without knee osteoarthritis: population based observational study (Framingham Osteoarthritis Study). BMJ 2012;345:e5339.
- Riddle DL, Stratford PW. Knee pain during daily tasks, knee osteoarthritis severity, and widespread pain. Phys Ther 2014;94(4):490-498.
- Kellgren JH, Lawrence JS, eds. The Epidemiology Of Chronic Rheumatism: Atlas of Standard Radiographs of Arthritis. Vol 2. Oxford: Blackwell Scientific; 1963.
- Rogers MW, Wilder FV. The association of BMI and knee pain among persons with radiographic knee osteoarthritis: A cross-sectional study. BMC Musculoskelet Disord 2008;9:163
- Ballegaard C, Riis RGC, Bliddal H, et al. Knee pain and inflammation in the infrapatellar fat pad estimated by conventional and dynamic contrast-enhanced magnetic resonance imaging in obese patients with osteoarthritis: A cross-sectional study. Osteoarthritis Cartilage 2014;22(7):933-940.
- Duncan RC, Hay EM, Saklatvala J, Croft PR. Prevalence of radiographic osteoarthritis—it all depends on your point of view. Rheumatology 2006;45(6):757-760.
- Schiphof D, Oei EHG, Hofman A, et al. Sensitivity and associations with pain and body weight of an MRI definition of knee osteoarthritis compared with radiographic Kellgren and Lawrence criteria: a population-based study in middle-aged females. Osteoarthritis Cartilage 2014;22(3):440-446.
- Maly MR, Costigan PA, Olney SJ. Mechanical factors relate to knee osteoarthritis. Clin Biomech 2008;23(6):796-805.
- Miller GD, Nicklas BJ, Loeser RF. Inflammatory biomarkers and physical function in older, obese adults with knee pain and self‐reported osteoarthritis after intensive weight‐loss therapy. J Am Geriatr Soc 2008;56(4):644-651.
- Samson AJ, Mercer GE, Campbell DG. Total knee replacement in the morbidly obese: a literature review. ANZ J Surg 2010;80(9):595-599.
- Felson D, Nevitt T, Zhang MC, et al. High prevalence of lateral knee osteoarthritis in Beijing Chinese compared with Framingham Caucasian subjects. Arthritis Rheum 2002;46(5):1217-1222.
- Dumond, H, Presle N, Terlain B, et al. Evidence for a key role of leptin in osteoarthritis. Arthritis Rheum 2003;48(11):3118-3129.
- Gabay O, Hall D, Berenbaum F, et al. Osteoarthritis and obesity: Experimental models. Joint Bone Spine 2008;75(6):675-679.
- Grabiner MD. Obesity and lower extremity osteoarthritis: Is body mass destiny? Quest 2004;56(1):41-49.
- Weisberg SP, McCann D, Desai M, et al. Obesity is associated with macrophage accumulation in adipose tissue. J Clinic Invest 2003;112(12):1796-1808.
- Elbaz A, Debbi EM, Segal G, et al. Sex and body mass index correlate with Western Ontario and McMaster Universities Osteoarthritis Index and quality of life scores in knee osteoarthritis. Arch Phys Med Rehabil 2011;92(10):1618-1623.
- Medline Plus website. http://www.nlm.nih.gov/medlineplus/ency/article/000423.htm. Updated August 3, 2013. Accessed August 20, 2014.
- Viester L, Verhagen EA, Oude Hengel KM, et al. The relation between body mass index and musculoskeletal symptoms in the working BMC Musculoskelet Disord 2013;14:238.
- Berenbaum F, Eymard F, Houard X. Osteoarthritis, inflammation and obesity. Curr Op Rheumatol 2013;25(1):114-118.
- Martin KR, Kuh D, Harris TB. Body mass index, occupational activity, and leisure-time physical activity: an exploration of risk factors and modifiers for knee osteoarthritis in the 1946 British birth cohort. BMC Musculoskelet Disord 2013;14:219.
- Toivanen AT, Heliövaara M, Impivaara O, et al. Obesity, physically demanding work and traumatic knee injury are major risk factors for knee osteoarthritis—a population-based study with a follow-up of 22 years. Rheumatology 2010;49(2):308-314.
- Übner M, Õun K, Mägi M. Relations between some anthropometric parameters of knee osteoarthritic patients and some indicators of the disease. Papers Anthropol 2013;22:289-300.
- Wills AK, Black S, Cooper R, et al. Life course body mass index and risk of knee osteoarthritis at the age of 53 years: evidence from the 1946 British birth cohort study. Ann Rheum Dis 2012;71(5):655-660.
- Weiss E. Non-weight-bearing joint pain and body mass index: Data from the Osteoarthritis Initiative and their implications for understanding osteoarthritis etiology. Am J Phys Anthropol 2014;153(Suppl):269.
- Aloisi AM, Albonetti ME, Carli G. Sex differences in the behavioural response to persistent pain in rats. Neurosci Lett 1994;179(1-2):79-82.
- Gierman LM, van der Ham F, Koudjis A. Metabolic stress-induced inflammation plays a major role in the development of osteoarthritis in mice. Arthritis Rheum 2012;64(4):1172-1181.
- Macfarlane G, de Silva V, Jones G. The relationship between body mass index across the life course and knee pain in adulthood: results from the 1958 birth cohort study. Rheumatology 2011;50(12):2251-2256.





